

Abstract
Objective. To evaluate the efficacy and safety of pregabalin monotherapy versus placebo for symptomatic pain relief and improvement of patient global assessment in patients with fibromyalgia (FM) enrolled from countries outside the United States.
Methods. This international, multicenter, double-blind, placebo-controlled trial randomly assigned 747 patients with FM to placebo or 300, 450, or 600 mg/day pregabalin twice daily for 14 weeks. Primary efficacy measures were endpoint mean pain scores and Patient Global Impression of Change (PGIC). Secondary outcomes included assessments of sleep and function.
Results. Patients in the 450 mg/day pregabalin group showed significant improvements versus placebo in endpoint mean pain score (−0.56; p = 0.0132), PGIC (73% improved vs 56% placebo; p = 0.0017), and function [Fibromyalgia Impact Questionnaire (FIQ) total score −5.85; p = 0.0012]. PGIC was also significant for 600 mg/day pregabalin (69% improved; p = 0.0227). Results for these endpoints were nonsignificant for pregabalin at 300 mg/day and for pain and FIQ score at 600 mg/day. Early onset of pain relief was seen, with separation from placebo detected by Week 1 in all pregabalin groups. All pregabalin doses demonstrated superiority to placebo on the Medical Outcomes Study-Sleep Scale Sleep Disturbance subscale and the Sleep Quality diary. Dizziness and somnolence were the most frequently reported adverse events.
Conclusion. Pregabalin demonstrated modest efficacy in pain, global assessment, and function in FM at 450 mg/day, and improved sleep across all dose levels, but it did not provide consistent evidence of benefit at 300 and 600 mg/day in this study. Pregabalin was generally well tolerated for the treatment of FM. (Clinical trial registry NCT00333866).
Fibromyalgia (FM) is a common, chronic pain disorder characterized by widespread pain and tenderness, frequently accompanied by a variety of other symptoms, such as fatigue, sleep disturbance, and mood disorders1,2,3,4. Recent epidemiology data suggest comparable prevalence of FM across developed countries. A 2008 epidemiologic survey of FM using American College of Rheumatology (ACR) criteria4 in France, Germany, and the United Kingdom found the prevalence of FM in the general population to be 1.4%–3.2%5,6,7. Prevalence estimates for other European and non-European countries were 0.7%–5.9%8,9,10,11,12,13,14,15,16,17,18,19,20,21. At the time this study was initiated, there were no randomized clinical trials in FM published outside the United States, and it was not known whether results of treatment with pregabalin would be consistent across regions, as perceptions of the disease and treatment approaches may have regional variation. The subsequent 2008 FM treatment guidelines issued by the European League Against Rheumatism22 show that of the 14 pharmacologic clinical trials considered eligible for evaluation, only 5 (36%) were conducted outside the United States, with 4 (29%) conducted in Europe.
Patients and physicians rank pain as their most important symptom domain23. Other key symptom domains include fatigue, sleep disturbance, health-related quality of life, comorbid depression, and cognitive difficulty23. Few current FM therapies have demonstrated consistent or adequate efficacy in these domains in large controlled clinical trials.
Four previous randomized controlled trials conducted in the United States demonstrated the efficacy and safety of pregabalin, an α2δ ligand with analgesic, anxiolytic, and anti-convulsant activity24, in the treatment of FM25,26,27,28, leading to pregabalin’s approval by the US Food and Drug Administration as the first drug indicated for the management of FM. Consistent improvement of pain and patient global assessment were demonstrated in the US studies in dosages from 300 to 600 mg/day.
The present trial was designed to determine the efficacy and tolerability of pregabalin in patients with FM from Europe and other non-US regions. The primary objectives assessed the efficacy and safety of pregabalin (300, 450, and 600 mg/day) administered twice daily compared with placebo for symptomatic pain relief and improvement of patient global assessment in patients with FM. Key secondary objectives evaluated the effect of pregabalin at improving sleep and function in FM.
MATERIALS AND METHODS
This randomized, double-blind, placebo-controlled monotherapy trial was conducted at 73 centers in Europe (Denmark, 2 centers, France 5, Germany 5, Italy 6, Portugal 4, Spain 4, Sweden 4, Switzerland 3, The Netherlands 5, and UK 5) or in Asia, Australia, and the Americas (Australia 4, Canada 12, India 4, Korea 3, Mexico 4, and Venezuela 3). The study was approved by the respective institutional review boards and/or independent ethics committees. Patients provided written informed consent before trial procedures were initiated. The trial was registered under NCT00333866 at http://www.clinicaltrials.gov and received the EudraCT number 2006-000425-57.
The methodology used and screening criteria, similar to those used in other pregabalin studies, have been reported27. Briefly, male and female subjects were at least 18 years old, met the 1990 ACR FM classification criteria4, had at least moderate pain [average pain score ≥ 4 on an 11-point numeric rating scale (NRS)] during baseline assessment, and had a score ≥ 40 mm on the 100-mm pain visual analog scale (VAS) of the Short-Form McGill Pain Questionnaire29 at screening and randomization. Exclusion criteria included patients who demonstrated a high placebo response (≥ 30% decrease on the VAS following the 1-week run-in period compared with screening).
After the 1-week placebo run-in phase, patients who fulfilled the screening criteria were randomized to pregabalin 300, 450, or 600 mg/day or to placebo, administered daily in 2 divided doses. Pregabalin treatment was started at 150 mg/day, was escalated to the randomized dose within 2 weeks of treatment, and was maintained for 12 additional weeks.
Efficacy assessments
The primary endpoint was mean pain score from patients’ daily pain diaries, as measured by the 11-point NRS recorded daily upon awakening. Patients rated their pain during the previous 24 hours using an appropriate number between 0 (no pain) and 10 (worst possible pain). The proportion of responders, defined as patients with a ≥ 30% or ≥ 50% reduction in mean pain score from baseline to endpoint30,31, and weekly mean pain score were determined as supplemental measures of primary efficacy.
A second primary endpoint, the Patient Global Impression of Change (PGIC), administered at the termination visit, also was used to evaluate the efficacy of pregabalin. The PGIC is a patient-rated instrument measuring change in patients’ overall status on a scale from 1 = very much improved to 7 = very much worse32.
Secondary efficacy measures
There were 2 key secondary endpoints: the Medical Outcomes Study-Sleep Scale (MOS-SS) Sleep Disturbance subscale33 and the Fibromyalgia Impact Questionnaire (FIQ) total score34 completed at baseline and termination (Week 14). In addition, patients rated their sleep quality on an 11-point NRS (0 = best possible sleep to 10 = worst possible sleep) daily upon awakening35 and completed the Hospital Anxiety (HADS-A) and Depression (HADS-D) scales at randomization and termination36. HADS-A and HADS-D are 7-item subscales that measure the presence and severity of anxiety and depression symptoms, respectively, on a scale of 0 to 3. Total scores ≤ 7 indicate no clinically relevant symptoms, 8 to 10 mild symptoms, 11 to 14 moderate symptoms, and ≥ 15 (maximum 21) indicate more severe symptoms.
Safety assessments
Adverse events (AE) were recorded at each visit. Investigators rated the severity of each AE and its relationship to study drug. Clinical laboratory evaluations, physical examinations, abbreviated neurologic examinations, and 12-lead electrocardiograms were performed at regular intervals.
Statistical analysis
Based on results from previous pregabalin FM studies (treatment difference of about 0.9 and standard deviation of about 2.025,26,27,28), the sample size of 185 patients per group was expected to provide > 95% power to detect a difference between at least 1 of the doses of pregabalin and placebo in endpoint mean pain, assuming 2-sided testing at the 0.0167 level to allow for Hochberg control of the type I error rate at 5%. This sample size was also expected to be sufficient for the PGIC.
Primary and secondary efficacy analyses were performed on all randomized patients taking at least 1 dose of study medication. Statistical testing comparing each pregabalin treatment to placebo was 2-sided and performed at the 0.05 level. The method of last observation carried forward was used for endpoint analyses, with the exception of a duration-adjusted average change (DAAC) sensitivity analysis of the mean pain score, which incorporates a penalty proportional to the amount of the study not completed.
The primary and sensitivity analyses of endpoint mean pain score and the secondary analyses of FIQ total score, the MOS Sleep Disturbance subscale score, and endpoint mean sleep quality scores used analysis of covariance, with terms for treatment, center, and baseline score37. Responder analyses (for endpoint mean pain score) were performed using the Cochran-Mantel-Haenszel procedure38, adjusting for center. The weekly mean pain scores and sleep quality scores were analyzed using repeated measures analyses, including factors for treatment, center, week, treatment by week, and baseline score. The PGIC was analyzed for shifts in the distribution of response categories between each pregabalin group and placebo (at the α = 0.05 level for each test) using the Cochran-Mantel-Haenszel procedure adjusting for center.
Additional covariates — region and the baseline HADS-A and HADS-D subscale scores — were defined to investigate the generalizability of the efficacy analyses. Each covariate was a binary categorical variable. Region indicated whether centers were European or non-European, and the HADS subscale scores indicated whether subjects had normal/mild (score ≤ 10) or moderate/severe (score ≥ 11) symptoms at baseline39. Tests for treatment by region, treatment by HADS-A interaction, and treatment by HADS-D interaction were performed at a significance level of α = 0.05. Statistical comparisons of each pregabalin treatment group with placebo within each region and for each HADS category were not performed owing to smaller sample sizes.
RESULTS
Patient disposition
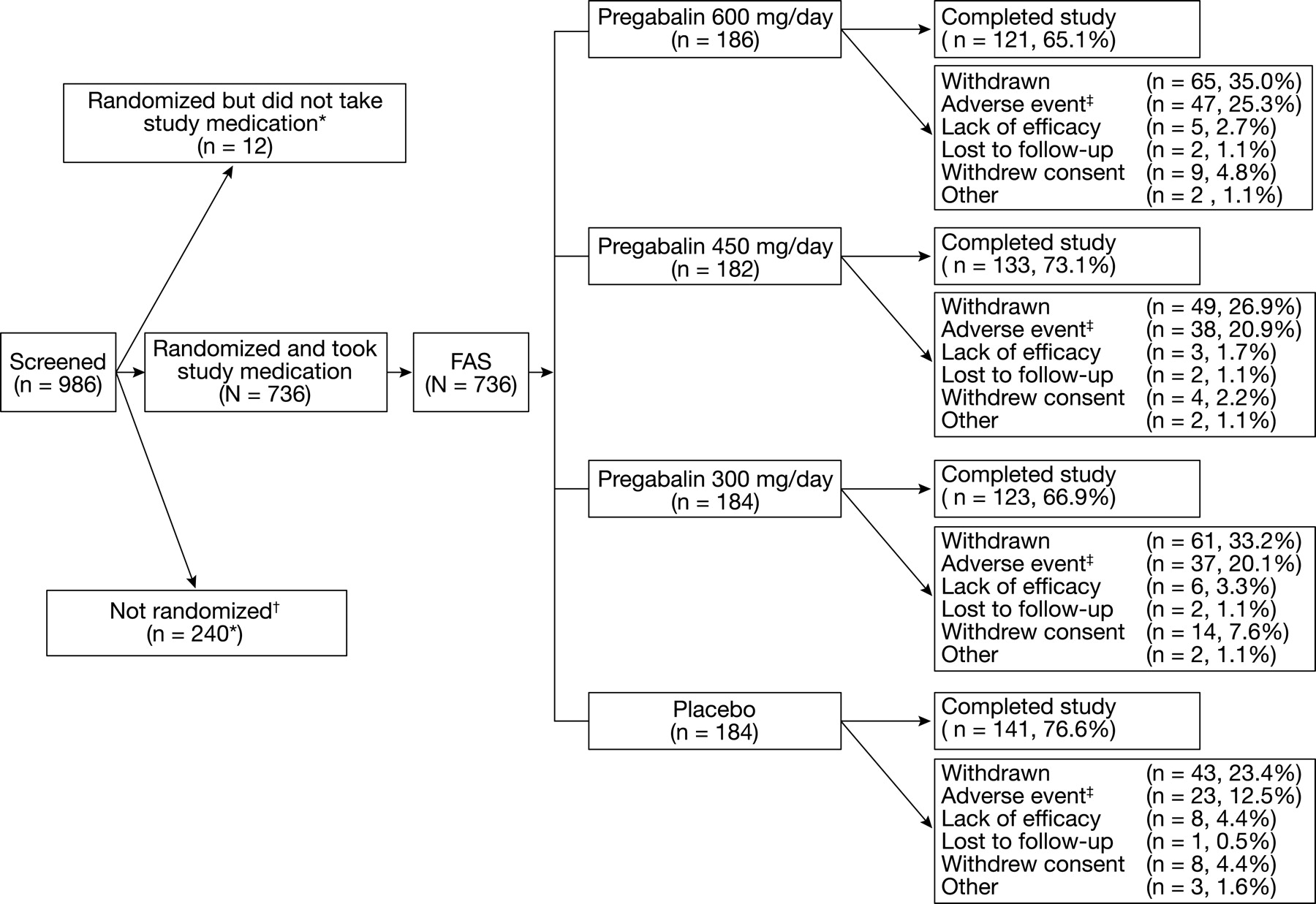
Altogether, 986 patients were screened and of these, 736 were randomized and received study medication. Thirty patients (3%) were discontinued after the 1-week placebo run-in phase because of ≥ 30% improvement on the pain VAS. Of the 736 patients who received study medication, 552 patients received pregabalin 300 mg/day (n = 184), 450 mg/day (n = 182), or 600 mg/day (n = 186), and 184 patients received placebo. Altogether, 218 patients (30%) withdrew during the double-blind treatment phase (Figure 1): 145 (20%) because of an AE, 22 (3%) because of lack of efficacy; 35 (5%) withdrew consent and 16 (2%) were either lost to followup or withdrew for other reasons.

Patient disposition. FAS: full-analysis set. *Includes 1 patient who was a screening failure, randomized in error, but who did not receive any treatment. †Includes 30 patients identified as placebo responders during the 1-week placebo run-in who were excluded from the study. ‡Includes discontinuations due to non-treatment-emergent adverse events (3 placebo patients, 2 pregabalin 300 mg/day patients, 2 pregabalin 450 mg/day patients).
Baseline characteristics
Demographic and clinical characteristics at baseline were generally similar across treatment groups (Table 1). Altogether, 379 (51%) patients were European and 357 (49%) were from non-European countries. Most patients were white (76%), female (91%), and aged between 18 and 64 years (92%). The mean age was 48.5 years (range 20–81 yrs). Altogether, 52% of women were post-menopausal. The mean duration of FM was 8.2 years. Demographic data were similar across regions with the exception of race: 96% of European patients were white compared with 55% of non-European patients.
Demographic and clinical characteristics of randomized patients.
Baseline scores for the efficacy endpoints were similar across regions (Table 1), reflecting a population with moderate to severe FM symptoms. The baseline mean pain score was 6.65, indicating moderate to severe pain; the MOS-SS Sleep Disturbance baseline mean score was 60.5; and the FIQ total score was 61.1. The baseline mean HADS-A and HADS-D scores fell into the mild category, with scores of 8.9 for anxiety and 7.5 for depression (range 0–21, mild = 8–10; higher scores indicate moderate-severe impairment)39.
Primary objective
Patients treated with pregabalin 450 mg/day demonstrated a statistically significant improvement in endpoint mean pain score compared with placebo-treated patients (−0.56; p = 0.0132; Table 2). Numeric improvements were observed versus placebo for pregabalin 300 mg/day (−0.33; p = 0.1694) and 600 mg/day (−0.23; p = 0.2361), but these improvements were not statistically significant. There was no evidence of a significant interaction between treatment and either center or baseline pain, which suggests that treatment effects were similar regardless of center or baseline pain. Patients in all 3 pregabalin treatment groups demonstrated a statistically significant improvement in weekly mean pain score beginning at Week 1 (Figure 2), the first timepoint analyzed. In the 450 mg/day treatment group, the statistically significant improvement was maintained throughout the study. The 600 mg/day dose demonstrated a reduction in pain severity through Week 8 and in the 300 mg/day group through Week 6.
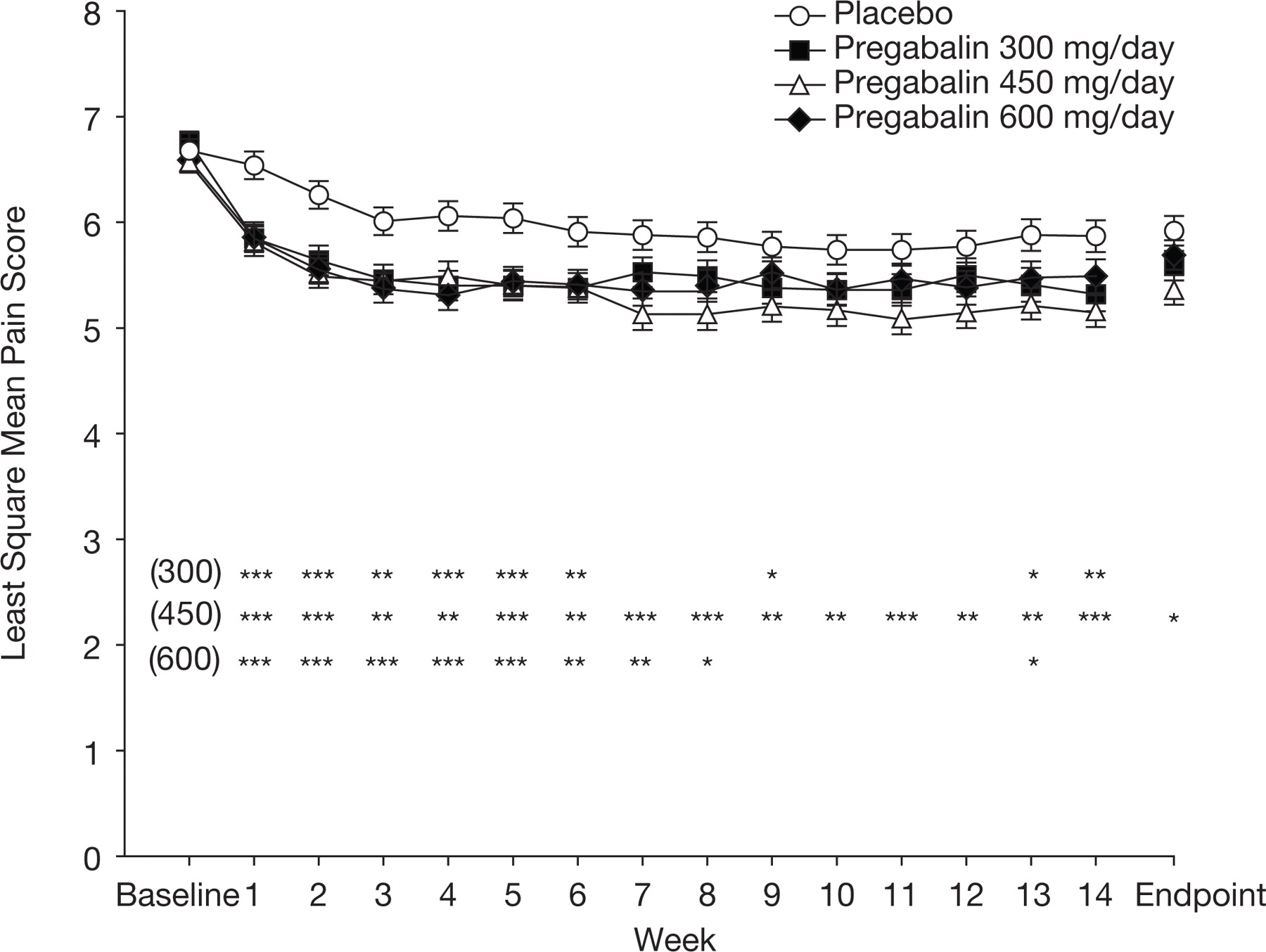
Weekly least-squares mean pain scores. Endpoint analyses based on last observation carried forward method. Error bars show ± standard error for each data point. *p < 0.05, **p ≤ 0.01, ***p ≤ 0.001 for all treatment groups versus placebo.
Endpoint values for outcome measures, full analysis set.
Subjects in all 3 pregabalin treatment groups showed a statistically significant improvement in the DAAC sensitivity analysis compared with placebo-treated subjects [mean differences −0.47, p = 0.0024 (300 mg/day); −0.61, p < 0.0001 (450 mg/day); and −0.47, p = 0.0023 (600 mg/day)].
Using a 30% pain reduction for the definition of pain response, the proportions of patients receiving pregabalin 300, 450, and 600 mg/day classified as pain responders were 33%, 34%, and 26%, respectively, compared with 19% for placebo. Using a 50% criterion, 18%, 18%, and 15% of patients receiving 300, 450, and 600 mg/day pregabalin, respectively, compared with 9% of placebo-treated patients were classified as responders. For both 30% and 50% responders, the comparisons of 300 and 450 mg/day pregabalin with placebo treatment were statistically significant, while the 600 mg/day pregabalin versus placebo comparison was nonsignificant.
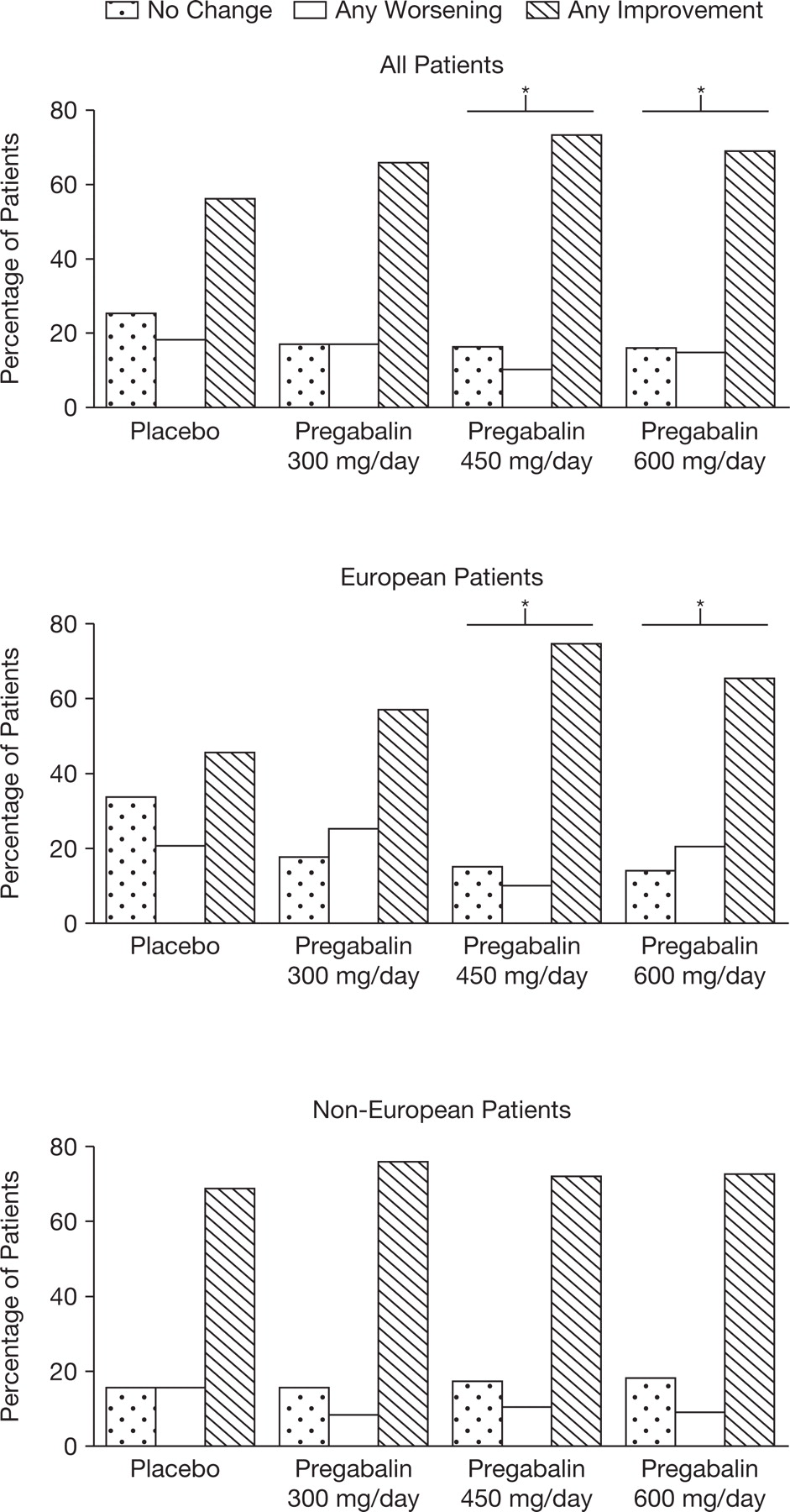
Significant differences in the second primary endpoint, PGIC, favoring pregabalin were observed with the pregabalin 450 and 600 mg/day groups versus placebo (p = 0.0017 and p = 0.0227 for 450 and 600 mg/day, respectively; Table 3, Figure 3). The pregabalin 300 mg/day versus placebo comparison did not achieve statistical significance (p = 0.0768). Overall, the percentage of patients reporting any improvement at endpoint was 66% for 300 mg/day, 73% for 450 mg/day, and 69% for 600 mg/day pregabalin, compared with 56% for placebo. The percentages of patients reporting “much improved” or “very much improved” on the PGIC at endpoint were 35%, 40%, and 43% with 300, 450, and 600 mg/day pregabalin, respectively, compared with 30% with placebo treatment.

Patient Global Impression of Change scores. *p ≤ 0.05 versus placebo.
Summary of Patient Global Impression of Change at endpoint.
Key secondary efficacy
All 3 pregabalin treatment groups showed statistically significant improvements in MOS-SS Sleep Disturbance subscale at endpoint compared with placebo (all p values ≤ 0.0038; Table 2). Patients in the 450 mg/day pregabalin group experienced a statistically significant improvement in the FIQ total score at endpoint compared with placebo-treated patients (mean difference −5.85; p = 0.0012; Table 2), while the treatment differences versus placebo were nonsignificant for the pregabalin 300 and 600 mg/day treatment groups.
Other secondary efficacy
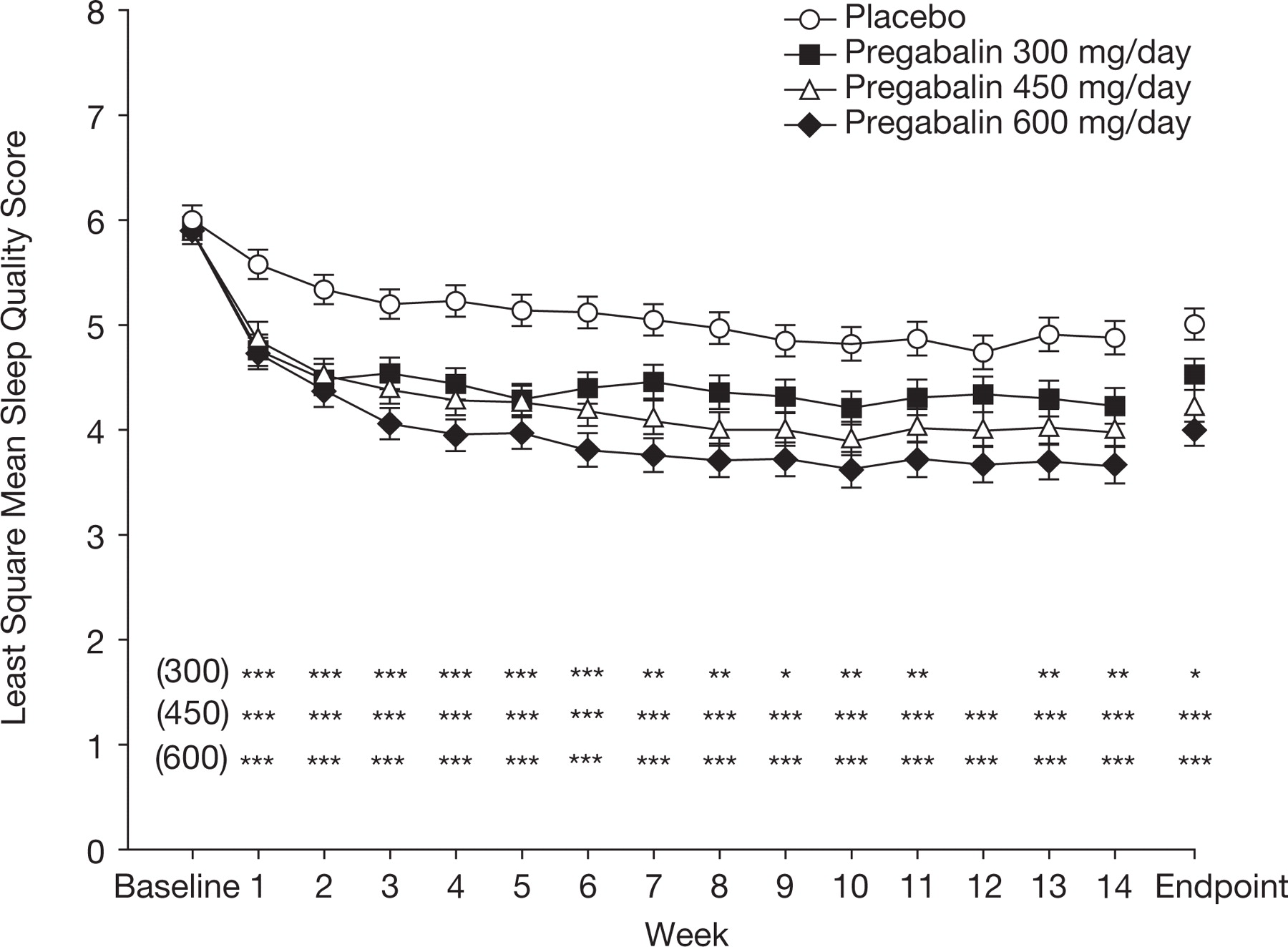
All 3 pregabalin dosages produced statistically significant improvements in sleep quality at endpoint (Table 2) and at each week (Figure 4) from Week 1 (all p values ≤ 0.0151) apart from 300 mg/day pregabalin at Week 12.

Weekly least-squares mean sleep quality scores. Endpoint analyses based on last observation carried forward method. Error bars show ± standard error for each data point. *p < 0.05, **p ≤ 0.01, ***p ≤ 0.001 for all treatment groups versus placebo.
Regional, anxiety, and depression effects
The magnitude of improvement in the efficacy endpoints differed somewhat by region, although there was no systematic pattern across endpoints suggestive of regional differences. The placebo-adjusted results demonstrated greater improvements in PGIC and sleep endpoints in European patients and greater improvement in pain and FIQ total score in non-European patients (Table 2, Figure 3). Importantly, no significant treatment by region interaction was observed with any of the endpoints. The test of treatment by baseline HADS-A and HADS-D interaction was nonsignificant, indicating that there was no evidence that baseline levels of anxiety and/or depression were influencing the magnitude of treatment response. In addition, mean changes from baseline to endpoint HADS-A and HADS-D scores were small (−0.14 to −0.6, on a scale of 1–21) and not statistically significant.
Safety
The safety profile for pregabalin was similar to that previously characterized. Of the 736 patients receiving study medication, 626 (85%) experienced at least 1 AE. The occurrence of AE increased with dosage (73%, 85%, 90%, and 92% for placebo, 300, 450, and 600 mg/day pregabalin patients, respectively; Table 4). The AE most frequently reported by pregabalin-treated patients were dizziness, somnolence, weight gain, headache, peripheral edema, fatigue, and dry mouth. Most AE were rated by investigators as mild or moderate in severity. Treatment-emergent AE are described in Table 4. A total of 18 patients experienced serious adverse events (SAE), 4 patients treated with placebo and 14 pregabalin (Table 4). Only 1 SAE, an incidence of chest pain in a patient in the 450 mg/day pregabalin group, was considered by the investigator to be related to treatment and the patient was withdrawn from the study. Eight other patients experienced an SAE that led to withdrawal from the study and 1 patient experienced an SAE that led to a dose reduction. Detailed information on all SAE is available under NCT00333866 at http://www.clinicalstudyresults.org. Withdrawal due to AE increased with dosage (11%, 19%, 20%, and 26% of placebo, 300, 450, and 600 mg/day pregabalin patients withdrew, respectively). The most common AE leading to discontinuation in pregabalin-treated patients were dizziness (42 patients, 7.6%), vertigo (17 patients, 3.1%), and somnolence (17 patients, 3.1%). The numbers discontinuing from the study with dizziness increased with pregabalin dose.
All-cause treatment-emergent adverse events.
Overall, 72 (13.0%) pregabalin-treated patients and 6 (3.3%) placebo patients reported weight gain as an AE. Of these, 7 pregabalin-treated patients discontinued because of weight gain. All AE of weight gain were rated by investigators to be mild to moderate in intensity. Fifty-seven (10.3%) pregabalin-treated patients experienced a clinically significant increase in body weight, measured to be 7% or more from baseline to end of treatment. There were no clinically relevant differences in clinical laboratory evaluations, vital signs, physical examination, or electrocardiogram findings.
DISCUSSION
Pregabalin at the 300 to 600 mg/day dose range has previously been demonstrated to reduce pain and improve function and other symptom domains important to FM25,26,27,28. Previous pregabalin FM studies were conducted entirely in the US. Our study was designed to evaluate the safety and efficacy of pregabalin for treating pain and other key symptom domains in patients with FM in non-US countries.
The patient demographic and FM disease characteristics were similar among treatment groups and were similar to those in US patients participating in pregabalin FM studies. Overall, patients had moderate to severe baseline pain, disturbed sleep, and impaired function. The baseline mean HADS-A and HADS-D scores fell into the mild category.
Treatment with pregabalin 450 mg/day resulted in statistically significant improvements in endpoint pain relief compared with placebo. Numerical improvements were observed in the other pregabalin treatment groups, but these improvements did not achieve statistical significance. A sensitivity analysis reflecting a penalty proportional to the missed amount of the study for any discontinuing patient demonstrated statistical significance for each pregabalin treatment group compared with placebo. Improvements were observed across the European and non-European regions. Onset was rapid, as all pregabalin groups separated from placebo at Week 1, the first timepoint analyzed. Statistically significant reductions in pain severity were seen for up to 8 weeks (300 mg/day) and were sustained throughout the 14-week double-blind period for the 450 mg/day dose. The pain response with pregabalin 600 mg/day was lower than anticipated, however. Previous studies consistently found greater mean reduction in endpoint mean pain scores at 600 mg/day than at lower doses. The reason for the lower than anticipated treatment effect at 600 mg/day is unclear, but may relate to a higher proportion of patients discontinuing because of AE (25%) in this treatment group.
Pain reduction of ≥ 30% is thought to represent clinically meaningful improvement in pain. The proportions of ≥ 30% and ≥ 50% pain responders were significantly greater than for placebo in the pregabalin 300 and 450 mg/day groups30. These results further support the clinical meaningfulness of the pain improvements noted in the primary analysis.
As a global measure, the PGIC allows patients to assess their own overall status, taking into consideration pain and other symptoms, physical and emotional functioning, and any AE. The 450 and 600 mg/day pregabalin dosages were associated with statistically significant improvement in PGIC ratings over placebo, indicating these changes were clinically relevant. The pregabalin 450 mg/day treatment group was also found to be superior to placebo with respect to functional improvement (FIQ total score).
Sleep disturbance is a key symptom domain in FM23. An Internet survey of more than 2500 patients with FM found that poor sleep is one of the most commonly occurring FM symptoms40. All 3 pregabalin doses demonstrated superiority to placebo on the MOS-SS Sleep Disturbance subscale and daily Sleep Quality diary. Statistically significant improvements in sleep quality were noted within 1 week and maintained throughout the course of treatment in all treatment groups, suggesting that pregabalin may be especially beneficial for patients with FM reporting pain and sleep disturbance.
The improvements in pain reduction, PGIC, FIQ total score, and MOS-SS Sleep Disturbance were consistent across regions and independent of baseline HADS-A and HADS-D scores.
The overall safety profile of pregabalin in this study was similar to that seen previously25,26,27,28. The most frequently reported AE were dizziness (43% pregabalin, 15% placebo) and somnolence (17% pregabalin, 6% placebo). The occurrence of AE increased with dose of pregabalin; in particular, dizziness increased from 37% to 50% across pregabalin treatment groups. Moreover, the proportions of patients withdrawing due to AE increased with dose, with 11%, 19%, 20%, and 26% of placebo, 300, 450, and 600 mg/day pregabalin patients withdrawing for this reason.
To determine whether AE may have biased the efficacy observed in this trial, pain, FIQ total, and sleep disturbance results were compared for patients reporting somnolence during the study and those not reporting somnolence. Pooled analyses of data from this trial and the other 12-week fixed-dose trials of similar design27,28 demonstrated that the magnitude of effect for each measure was comparable for pregabalin-treated patients, regardless of somnolence reporting (Atkinson, et al, unpublished observations).
To gain a better understanding of the benefit/risk profile of pregabalin in this study, the method of Cook and Sackett41 was used to calculate the number needed to treat (NNT). For pregabalin 450 mg/day, NNT to achieve ≥ 30% pain improvement was calculated to be 6.8 and NNT for ≥ 50% pain improvement was 11.1. The NNT (pregabalin 450 mg/day) to achieve any PGIC improvement, or to achieve much or very much PGIC improvement, were 5.9 and 10.0, respectively. The number needed to harm based on discontinuations due to AE (pregabalin 450 mg/day) was 11.1. These results indicate modest efficacy relative to risks on average. Substantial proportions of patients, however, demonstrated clinically meaningful benefit, with 40% of those treated with pregabalin 450 mg/day reporting much or very much improvement (30% for placebo) and 33% reporting ≥ 30% pain improvement (19% for placebo). Thus, a significant subset of patients reported meaningful benefit with pregabalin treatment, which was tolerated reasonably well.
Pregabalin demonstrated modest efficacy in pain, global assessment, and function in FM at dosages of 450 mg/day, and improved sleep across all dosages, but did not provide consistent evidence of a benefit at dosages of 300 mg/day and 600 mg/day in this study.
Acknowledgment
The authors thank Dr. Max Gough at Technical Typesetters Inc., and Dr. Alison Gagnon of UBC Scientific Solutions for editorial support during development of this report.
APPENDIX
List of study collaborators. The Study A0081100 Investigators: Australia: Geoffrey Littlejohn, Guy Bashford, Laurence Clemens, Mark Cook, Peter Nash. Canada: Jacques Brown, Christian Cloutier, Giuseppe D’Ignazio, Paul Latimer, Harvey Moldofsky, Anthony Wade, Nicole Giguere, Michelle Young, Mary Fitzcharles, Murray Baron, Ian Sutton. Denmark: Bente Danneskiold-Samsoe, Ketil Bjerregaard. France: Serge Perrot, Francis Blotman, Pierre Hatron, Bernard Laurent, Fabienne Riaux. Germany: Frank Buttgereit, Gerd-Ruediger Burmester, Andreas Krause, Dieter Pongratz, Thomas Weiss. India: Ramnath Misra, Yashpal Singh, Pradeep Mehta, Gajendra Bhandari, Pradeep Mehta, Sandeep Puri. Italy: Stefano Bombardieri, Maria Giamberardino, Marina De Tommaso, Nazzarena Malavolta, Roberto Gerli. Republic of Korea: Sang-Cheol Bae, Sang-Heon Lee, Chang-Hee Suh. Mexico: Roberto Hernandez-Paz, Carlos Abud-Mendoza, Mario Garza-Elizondo, Manuel Martinez-Lavin. Portugal: Rui André, Jaime Branco, Augusto Faustino, Rui Leitão. Spain: Javier Vidal Fuentes, Cayetano Alegre De Miguel, Eduardo Collantes, Jordi Carbonell. Sweden: Olof Zachrisson, Jan Sörensen, Yngve Hallstrom, Bjarne Mansson. Switzerland: Jean Dudler, Robert Theiler, Daniel Uebelhart. The Netherlands: E.N. Griep, H.R. Van Den Brink, J.R.M. Griep-Wentink, P.J. Barendregt, T.R. Zijlstra. United Kingdom: Selwyn Richards, David Marshall, David Walker, Timothy Johnson, Barbara Duncan. Venezuela: Graciela Bencosme, Veronica Liendo, Sol Villegas de Morales.
Footnotes
-
Supported by Pfizer Inc.
- Accepted for publication July 26, 2011.








{kind=link}
{kind=link}
{kind=link}
{kind=link}