

Abstract
Objective. To examine the construct validity of the 28-tender joint count (TJC-28) using item response theory (IRT)-based methods.
Methods. A total of 457 patients with early stage rheumatoid arthritis (RA) were included. Internal construct validity of the TJC-28 was evaluated by determining whether the TJC-28 fit a 2-measure logistic IRT model. As well, we tested whether the discrimination and difficulty parameters of the joints properly reflected the known left-right symmetry of joint involvement. External validity was evaluated by correlations with other established measures of disease activity, including pain, disability, general health, erythrocyte sedimentation rate (ESR), and the 28-swollen joint count.
Results. The TJC-28 showed a good fit with the 2-parameter logistic model, with no relevant differential item functioning across sex, age, and time and with excellent reliability. The 28 joints covered a reasonable range of disease activity, even though they were mainly targeted at patients with moderate or high disease activity levels. The joint parameters reflected the left-right symmetry of joint involvement for all pairs of joints except one. All disease activity measures, except ESR, were significantly correlated with the TJC-28. Most correlations were of the expected magnitude.
Conclusion. The TJC-28 showed good internal and acceptable external construct validity for patients with early-stage RA. The IRT analyses did point to some potential limitations of the instrument, a major problem being its limited measurement range. Future research should examine whether instrument modifications might lead to a more robust assessment of disease activity in patients with RA.
- 2-PARAMETER LOGISTIC MODEL
- 28-TENDER JOINT COUNT
- COHORT STUDY
- CONSTRUCT VALIDITY
- ITEM RESPONSE THEORY
- RHEUMATOID ARTHRITIS
Rheumatoid arthritis (RA) is a systemic autoimmune disease, decreasing life expectancy by 3 to 10 years compared to the general population1,2. People with RA experience chronic inflammation of joints and periarticular tissues3, characterized by symmetric pain and swelling in the joints4,5,6,7. The disease generally follows an unpredictable course, often with alternating periods of mild and severe disease activity3.
RA treatments are aimed at reaching a state of remission as soon as possible8. Because joint tenderness is an important characteristic of RA, joint counts that measure the extent of joint tenderness are used for the assessment of RA severity9. A joint count is a specific quantitative clinical measure to assess the status of a patient with RA10. Therefore, it forms a major component of indices of disease activity11 and remission12. Although various joint counts have been developed, ranging from the evaluation of 28 to 80 joints, the 28-joint count is currently the most widely used measurement instrument.
Earlier studies showed the 28-tender joint count (TJC-28) to be a reliable and valid joint index9,13,14,15. However, these studies have used only classical test theory (CTT) methods. To date, the construct validity of the TJC-28 has never been analyzed using item response theory (IRT)-based methods. IRT is a sophisticated psychometric approach that has been adopted to supplement the more traditional approaches16 to enable a more thorough evaluation of an instrument’s psychometric characteristics. IRT has already been frequently and successfully applied in evaluating and improving health outcome questionnaires17, but it has rarely been applied to clinical measures, such as tender joint counts. Therefore, the aim of our study was to examine both the internal and external construct validity of the TJC-28 using IRT-based methods.
MATERIALS AND METHODS
Patients with early-stage RA participating in the Dutch Rheumatoid Arthritis Monitoring remission induction cohort18 were included in this study. This observational, multicenter cohort was established in 2006 to evaluate a treatment strategy aimed at reaching a state of remission. The patients were asked for inclusion in the cohort by their rheumatologists. Patients were qualified for inclusion at the moment of clinical diagnosis of RA. Symptom duration was a maximum of 1 year, and patients had to be at least 18 years old. Any who had previously used disease-modifying antirheumatic drugs or prednisolone were excluded from the cohort.
The result was a total baseline sample of 457 patients. Measurements were performed during each hospital visit. The data from the first timepoint (i.e., at inclusion) were used for all analyses. In addition, one of the fit analyses (i.e., evaluating differential item functioning across time) was based on data from the first 3 timepoints (t1 = at inclusion, t2 = 8 weeks after inclusion, t3 = 12 weeks after inclusion). Because the duration since inclusion varied among patients, followup measurements involved a decreasing number of patients. At the third timepoint, the remaining sample consisted of a total of 391 patients.
Measures
The TJC-28 and the 28-swollen joint count (SJC-28) were administered separately at each visit by a trained nurse practitioner or rheumatologist. The 28 joints were scored on a dichotomous scale, with 0 indicating “no pain” or “no swelling” in the joint, and 1 indicating “pain” or “swelling” in the joint9,19. Both 28-joint counts include the shoulders, elbows, wrists, and knees, the 10 metacarpophalangeal (MCP) joints, and the 10 proximal interphalangeal (PIP) joints20.
Besides the TJC-28 and the SJC-28, patients were asked to complete the Health Assessment Questionnaire-Disability Index (HAQ-DI)21, which measures physical function, and visual analog scales for pain (VAS pain) and general health (VAS GH). The alternative disability index (HAQ-ADI)22, which does not correct for the use of aids and devices, was derived from the HAQ-DI and was scored on a scale from 0 to 3 (higher scores indicating more physical disability). Pain and general health were measured using a 100-mm VAS scale, 0 indicating “no pain” or “very good”, and 100 indicating “unbearable pain” or “very bad.”
Laboratory samples were collected before each hospital visit, including the erythrocyte sedimentation rate (ESR), which is a nonspecific measure of inflammation19.
Statistical analyses
When using an IRT framework, the relationship between item scores and the underlying construct of interest (i.e., the latent trait variable θ, representing the degree of joint tenderness in our study) can be modeled. When applying CTT approaches, sum scores of different combinations of joints can be obtained. However, this does not imply that the sum score reflects a meaningful underlying construct. IRT has several beneficial properties compared to the traditional CTT approach, enabling a more thorough evaluation of an instrument’s psychometric characteristics. If the TJC-28 fits an IRT model, this supports the construct validity of the instrument, because this shows that the observed responses can be explained by the underlying structure of the instrument23. Further, if attenuation is present (i.e., underestimated correlations between measurements due to unreliability caused by measurement error), IRT can deal with this problem more precisely than the CTT approach since it considers latent correlations instead of sum-score based observed correlations. In addition, IRT can successfully handle incomplete item administration designs and missing data, and where CTT often assumes a normal distribution of the true scores, IRT can deal with various distributions of latent variables23.
IRT models the probability of a joint being scored as tender on the basis of characteristics of the patient (the degree of joint tenderness: θ) and the item (such as the difficulty and discrimination level). Each single joint is regarded as an item and has a corresponding IRT model curve. Two widely applied IRT models are the Rasch model (also known as the 1-parameter logistic model) and the 2-parameter logistic (2-PL) model, both shown in Figure 1. The y-axis shows the probability of a joint to be scored as tender, while the x-axis shows the latent trait that corresponds to the degree of joint tenderness a patient experiences (θ, scaled around zero). Figure 1A shows the Rasch model, including 3 joints with different difficulty parameters24. The value of the difficulty parameter of a specific joint equals the point on the x-axis at which the patient has a probability of 0.5 of having a painful joint24,25. So for joint 1, its value will be equal to −1. Figure 1B shows the 2-PL model. In it, the curves intersect because of addition of the discrimination parameter. This parameter is proportional to the slope of the curve; the higher its value, the steeper the slope, and the better the joint discriminates between patients with various degrees of joint tenderness25.
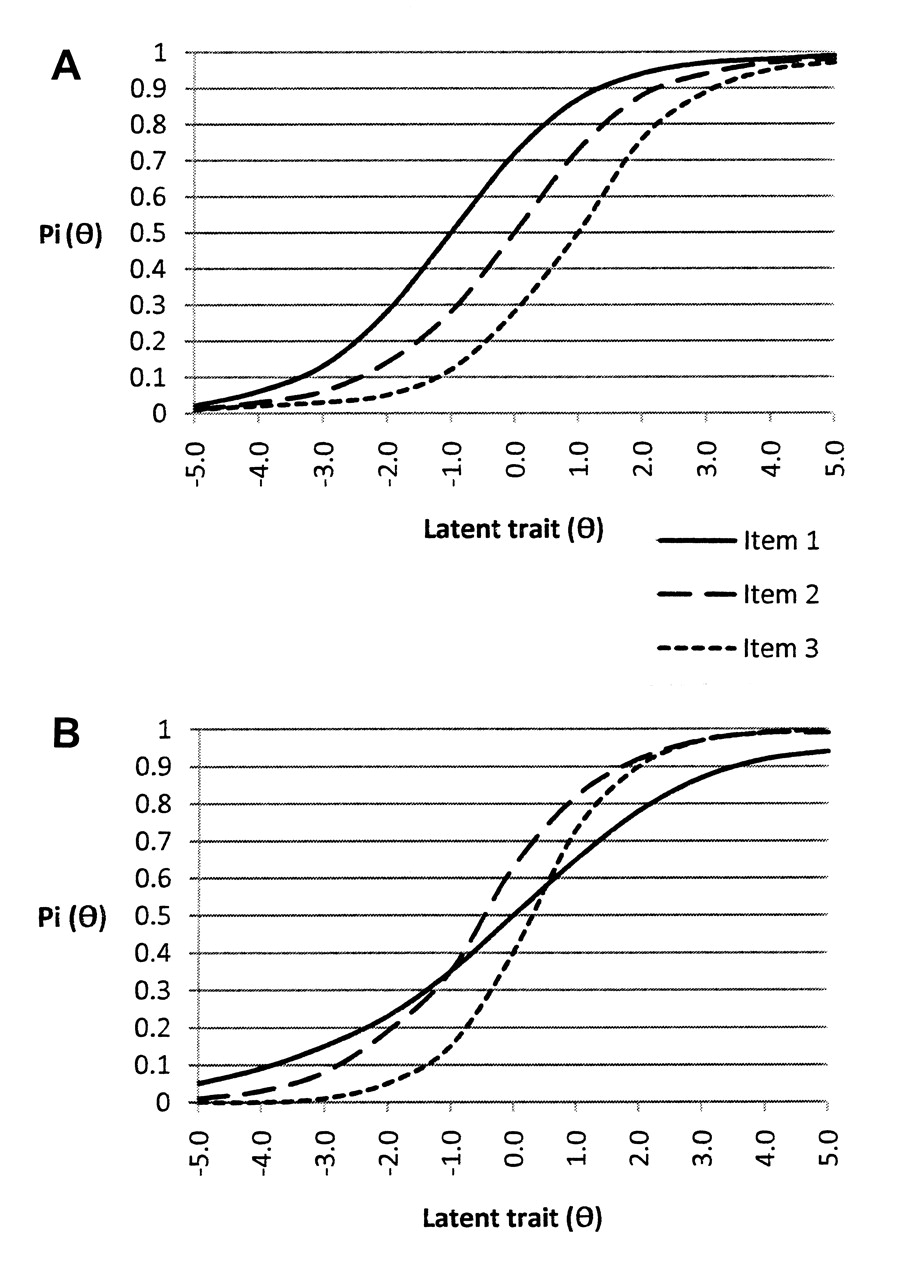
Graphic representation of the Rasch model (A) and the 2-parameter logistic model (B), where Pi(θ) is the probability of a joint being scored as tender.
In our study, a 2-PL model was used to analyze the construct validity of the TJC-28. This was motivated by both practical and empirical reasons. First, we wanted to examine whether the symmetry that characterizes RA is reflected in both the difficulty and the discrimination parameters of the IRT model. Second, a log-likelihood ratio test showed that the 2-PL model had a significantly better fit to the TJC-28 than the Rasch model (log-likelihood ratio test = 163.81, df = 27, p < 0.01).
Internal construct validity
This was assessed by evaluating whether the TJC-28 could be fitted to the 2-PL model, whether the joint parameters truly reflected the known left-right symmetry of joint involvement in patients with RA4,5, and whether the TJC-28 had an acceptable reliability.
Fit analyses
IRT models rely on several assumptions. One of these concerns the shape of the response curves. Using a Lagrange multiplier test, the LM-Q1-test26, it was determined whether the shape of the curves belonging to the TJC-28 fit the shape of the curves assumed by the 2-PL model. This means the joint curves have various difficulty parameters, various discrimination parameters, and a lower zero asymptote. Two outcome values considered important for determining the fit of the curves with the LM-Q1-test are the p value of the test and the effect size27. A p value > 0.05 indicates a good item-model fit, but this statistic is sensitive to large sample sizes27. For large sample sizes, the absolute effect size should also be evaluated. The effect size is given by the difference between the observed and the expected average score on an item in a specific group and can, therefore, range between 0 and 1. An effect size of < 0.10 has been previously used as an acceptable measure for item model fit28. Well-fitting response curves can also be seen as strong evidence for unidimensionality of the TJC-2829.
Additionally, it was examined whether differential item functioning (DIF) across sex, age, and time was present. A joint shows DIF across sex or age if individuals from different groups (e.g., men vs women) but with the same latent trait value do not have the same probability of reporting a joint as being tender24. DIF across time is present when the joint difficulty parameters are unstable over time27. The stability of the parameters was examined over the first 3 timepoints.
Left-right symmetry of joint parameters
The symmetry of the difficulty and discrimination parameters was simultaneously tested for each pair of joints using a Wald test30. This test determines whether the parameter values of the left-side joint and the parameter values of the right-side joint are equal. Nonsignificant results (p > 0.05) indicate that the joint parameters properly reflect the known left-right symmetry of joint involvement.
Reliability and measurement precision
In IRT, the reliability of the TJC-28 is estimated as the ratio of the expectation of the posterior variance of the latent variable θ given the instrument score, and the total variance of θ29. A θ value > 0.70 is considered acceptable for group use, while a value of 0.85 or higher is required for individual use16. The IRT reliability coefficient is equivalent to Cronbach’s alpha.
When applying IRT, the range of θ for which a joint or the total TJC-28 is most reliable for measuring patients’ levels of joint tenderness can be depicted in an information curve. An information curve shows the range over θ where the individual joint or the total TJC-28 can best discriminate among individual patients31. Ideally, the instrument includes joints with high discrimination parameters that cover a broad spectrum of joint difficulties. In this way, the spectrum of joint tenderness can be measured as precisely as possible. The higher the information level of a joint, the more the joint contributes to the measurement precision of joint tenderness. Information curves of individual joints were plotted for evaluation of the performance of each single joint. The test information curve of the TJC-28 and its associated reliability levels [r = 1 – (1/test information at θ)] were plotted to evaluate the performance of the total TJC-28.
External construct validity
Previous studies used sum scores of the TJC to determine its correlation with other established measures of disease activity, while IRT uses latent trait values (θ). The external construct validity of the TJC-28 was evaluated by examining whether the baseline θ values and traditional sum scores of the TJC-28 showed an expected pattern of correlations with 5 other established measures of disease activity32: VAS pain, HAQ-ADI, VAS GH, ESR, and the SJC-28.
Correlations < 0.3 were defined as weak (low), between 0.3 and 0.6 as moderate, and > 0.6 as strong (high)33. All correlations were expected to be both positive and significant. Although highly variable correlations between the TJC and these variables were found in previous studies, moderate correlations were expected since they are all measures of disease activity9,14,34,35,36,37,38.
RESULTS
Demographics at inclusion
Baseline data were available from 457 patients (288 women and 169 men). The mean (SD) age at inclusion was 55.4 (15.2) years for the women and 59.8 (12.4) years for the men. Baseline measures of disease activity are summarized in Table 1. The TJC-28 had a mean score of 5.7. For interpretation, a TJC-28 score of 0 corresponded to an estimated θ score in the range of −1.65 to −0.69, and a TJC-28 score of 28 corresponded to estimated θ scores in the range of 2.82 to 3.25.
Mean scores (SD) of established measures of disease activity at baseline in 457 patients with early-stage rheumatoid arthritis.
Internal construct validity
Table 2 presents the results of the fit analyses. Although some joints showed a statistically significant misfit (p < 0.05), all effect sizes were well below 0.10. These results indicate that there was a good fit between the curves of the TJC-28 and the 2-PL model. In addition, there was no relevant DIF across sex, age (median split: ≤ 59 vs ≥ 60 years), and time.
Results of the fit analyses.
Left-right symmetry of joint parameters
Table 3 presents the parameter estimates generated by the 2-PL model. The Wald test showed a nonsignificant result for all pairs of joints except 1. This demonstrates that both the difficulty and the discrimination parameters properly reflected the left-right symmetry of joint involvement, which is characteristic of RA.
Average joint scores, item response theory joint parameter values, and Wald test results.
Reliability and measurement precision
The reliability of the TJC-28 was acceptable for group use as well as for individual use (r = 0.874).
Table 3 presents the discrimination parameter values, ranging from 0.670 to 1.049 for larger joints (shoulders, elbows, wrists, knees), and from 1.369 to 2.269 for smaller joints (the MCP and PIP). Joint difficulties covered only the positive half of the spectrum, ranging from 0.613 to 3.659, reflecting low response probabilities. This limited range of joint difficulties was also reflected in the information curves (Figure 2). The test information curve showed that the scale measured the patient’s level of θ with a reliability level acceptable for group use (r > 0.70) over the range from θ = 0.60 to θ = +3.0531. Outside this range, the test information curve and the scale’s reliability rapidly decreased, meaning that the corresponding levels of θ were estimated with reduced precision. Over the range from θ = 0.0 to θ = +2.5, the scale’s reliability was also acceptable for individual use (r > 0.85). The reliability was at its highest point (r > 0.93) at θ = +1.3. The item information curves showed that smaller joints (MCP and PIP) provided more information to the test than larger joints (shoulders, elbows, wrists, knees).

Top graph shows the test information curve of the 28-tender joint count with its associated reliability level. The graphs below represent the item information curves for the joints on the left side (left column) and right side (right column) of the body.
External construct validity
Spearman’s correlations with the other established measures of disease activity for both the θ estimations and the sum scores of the TJC-28 are shown in Table 4. The correlations based on the θ estimations of the TJC-28 were very similar to the correlations based on the sum scores. As expected, all correlations were positive. However, for both the θ estimates and the sum scores of the TJC-28, only 4 out of 5 correlations were significant. The HAQ-ADI, joint swelling, and the patient’s general health assessment did show the expected moderate correlations. Pain correlated less strongly with joint tenderness than expected, but the correlation was only just below the cutoff point of 0.30. However, a very low correlation was found with ESR.
Spearman’s correlations of the TJC-28 (using θ as well as the sum score) with the sum scores of the established measures of disease activity at baseline (n = 457). Except where indicated, p ≤ 0.01 (2 tailed).
DISCUSSION
This is the first study to examine the validity of the TJC-28 by applying IRT-based methods. As a result, the instrument’s psychometric characteristics can be evaluated more thoroughly than with CTT alone. The results showed that the TJC-28 is a valid and reliable measure for patients with early-stage RA. An acceptable fit of the TJC-28 to the 2-PL model was demonstrated, with no relevant DIF across sex, age, and time, and with excellent reliability. The joints included in the TJC-28 covered a reasonable range of disease activity, although measurement precision was limited for lower levels of disease activity. Additionally, the joint parameters properly reflected the left-right symmetry of joint involvement. Evaluation of the external validity showed that all correlations, except with ESR, were similar to the correlations found in previous studies.
Statistical transformations of the ESR values, such as square root and natural logarithm transformations as performed in the Disease Activity Score for 28 joints15, did not improve the correlation with joint tenderness. A limited distribution of ESR values within the patient sample might explain the nonsignificance of this correlation. However, given the high SD (22.04) of the ESR values, this does not seem plausible. Moreover, secondary analyses did show significant and higher correlations between ESR and all other measures of disease activity (r between 0.17 for the VAS GH and 0.30 for the HAQ-ADI) and C-reactive protein (r = 0.64), another measure of inflammation. Evaluation of the correlations with the individual joints showed that ESR was significantly correlated with the larger joints (r between 0.10 and 0.14), but not with the smaller joints that constitute the largest part of the TJC-28. This higher correlation with larger joints is in accord with earlier findings37 and suggests that the ESR mainly reflects the volume of inflammation in the larger joints, while the TJC-28 is also in large part explained by the smaller joints. Future studies should evaluate the correlation between the TJC-28 and ESR in an RA population in which the patients have more inflamed smaller joints than in the current sample, to determine whether joint size affects this correlation.
Examination of the correlations showed that those based on the θ estimations of the TJC-28 were very similar to the correlations based on the sum scores of the TJC-28. This indicates that the θ scores and the sum scores corresponded highly to each other and that attenuation did not pose any serious problems in our study, diminishing the actual advantage of using IRT-based scores instead of sum scores for evaluating the external construct validity of the TJC-28. It also suggests that it is adequate to use sum scores for the calculation of a patient’s TJC.
The unequal discrimination parameters give additional support for use of the 2-PL instead of the Rasch model, since those parameters are assumed to be equal in the Rasch model. The parameter results also showed that the smaller joints especially showed high discrimination parameters, indicating that the MCP and PIP joints discriminate better between patients with different degrees of joint tenderness (θ) than do larger joints (shoulder, elbow, wrist, knee; Table 3). This is in line with the clinical experience of healthcare providers treating patients with RA. A point of interest regarding the joint difficulties is that the wrists show the lowest values (Table 3). They also have the highest average score (left wrist: 0.35, right wrist: 0.38), which is consistent with the clinical experience that the wrist is a commonly affected joint in RA39,40. This is also reflected in the minor degree of information the wrists provide to the test. However, the wrists do provide some information at the lower levels of disease activity, which can be regarded as a positive property given the limited measurement range of the instrument along the lower range of disease activity.
The results concerning the reflection of left-right symmetry of joint involvement in the joint parameters reflect several studies that emphasize that symmetry of joint involvement characterizes RA4,5,6,7, providing additional support for the construct validity of the TJC-28. From a strict test perspective it can be argued that this would imply that half of the joints can be removed from the TJC-28. After all, it can point to redundant items, which might be locally dependent and that make the test unnecessarily long. However, removing items might have an effect on the psychometric characteristics of the test by reducing the test information and its corresponding reliability. Moreover, from a clinical perspective it is probably undesirable to remove half of the joints, because a patient’s total number of tender joints are being used for individual diagnosis and treatment decisions.
The IRT analyses showed that the TJC-28 is a highly reliable instrument; however, this does not imply that the scale also has high interrater reliability. Interrater bias might still be embedded in the inaccuracies of the measure. It is clear, however, that this type of bias did not pose any serious problems in our study, since problems with interrater reliability have mainly been reported for graded or weighted joint counts19,41,42, while a nongraded TJC was used in our study.
The accuracy and broadness of the test, given the high discrimination parameters and the range of joint difficulties covered, make accurate measurement of change over time possible. The advantage of using IRT instead of the more traditional approaches is that latent trait values are used instead of sum scores. Even when there are data missing, the latent trait values can still be estimated.
IRT has been successfully applied for the evaluation and improvement of questionnaires of health outcome measures17. Since the focus of IRT is at the item level instead of the test level, the contribution of each single joint can be evaluated without knowledge of the other joints in the instrument24, a feature that is not available in procedures based on CTT methods. Among others, this feature makes it possible to obtain joint counts with lesser joints without major loss of measurement precision24. However, IRT has rarely been applied for the evaluation or improvement of clinical measures, such as TJC. One demonstration of the application of IRT in a clinical trial can be found in Glas, et al43. They successfully applied IRT to tender point counts in fibromyalgia. They showed that tender point counts of patients diagnosed with fibromyalgia had a good fit with IRT models, and that items could be removed without facing a substantial loss of power. Our study extended this application to clinical measures by applying IRT to TJC in patients with early-stage RA. Future studies could investigate whether a modified or shorter TJC will perform equally well or perhaps even better than the TJC-28.
In contrast to CTT, IRT information curves can be obtained when applying IRT to the data. This provides insight into the performance of the total TJC-28 and of the individual joints, and exposes opportunities for scale improvement. The covered range of joint difficulties demonstrated that the TJC-28 mainly functions along the moderate and higher spectrum of disease activity. The test and item information functions also showed that θ is measured with the greatest precision for patients with a higher degree of joint tenderness, especially with joint tenderness in the smaller joints. This spectrum limitation was caused by the low number of painful joints experienced by the sample of patients with early-stage RA. Since the cohort we used represented a large sample size, and since it included patients from 6 hospitals from different regions in The Netherlands, it is expected that this cohort is representative of the patients with early-stage RA. However, to further examine the measurement precision of the TJC-28 and to make the results more generalizable, future research should expand our study by applying IRT to RA samples with a longer disease duration.
The rationale concerning which joints to include in a joint count has not yet been clearly outlined in the literature. The joints included in the TJC-28 were selected based on pragmatic logistic considerations and clinical experience20. Although the TJC-28 appears to be a reliable and valid instrument to assess joint tenderness, it does not include the feet and ankle joints. There have been several discussions about whether the feet and ankles really can be omitted from the instrument44,45. It has been argued that the 28-joint count might be useful in clinical trials, but that a more comprehensive joint count that includes the foot joints might be preferable for following the disease progress of patients in daily clinical practice13,19. IRT may provide clarity in this discussion, since IRT provides an opportunity to evaluate the contribution of each single foot joint and ankle joint24. The joints differ in the degree of information they provide, shown by the inequality in the parameter values. This means the joints contribute unequally to the precision of measurement. By evaluating whether foot and ankle joints provide any significant information, it can be decided whether they truly can safely be omitted from the joint count. Future research should apply IRT to more extensive joint counts, such as the TJC-68, to examine which joints provide important information to the instrument and should be included, and which joints provide limited information and can therefore be omitted from the joint count.
Our study confirmed that the TJC-28 has good internal and acceptable external construct validity for patients with early-stage RA. However, the IRT analyses also pointed to some potential limitations of the instrument — a major problem being its limited measurement range. Since test information was low for lower levels of disease activity, it might be appropriate to modify the TJC-28 to improve its measurement precision and range, for instance by expanding the TJC to joints that provide more information at the lower levels of disease activity. It is recommended that future studies examine both the TJC-28 and more extensive joint indices in RA samples with a longer disease duration to confirm our findings and to explore possibilities for further improvements of the TJC.
Acknowledgment
The authors thank the respondents who participated in our study and the rheumatologists from the Medisch Spectrum Twente (Enschede), Ziekenhuisgroep Twente (Almelo, Hengelo), Isala Klinieken (Zwolle), Universitair Medisch Centrum Groningen (Groningen), UMC St. Radboud (Nijmegen), and TweeSteden Ziekenhuis (Tilburg) for their assistance in patient recruitment and data collection.
- Accepted for publication July 29, 2011.








{kind=link}
{kind=link}