

Abstract
Objective. To determine the effects of changing from oral to subcutaneous (SC) methotrexate (MTX) in patients with rheumatoid arthritis (RA) on red blood cell MTX polyglutamate (RBC MTXGlun) concentrations, disease activity, and adverse effects.
Methods. Thirty patients were changed from oral to SC MTX. Trough RBC MTXGlun concentrations were measured for 24 weeks and concentrations fitted to a first-order accumulation model. Disease activity was assessed by 28-joint Disease Activity Score (DAS28).
Results. MTXGlu3, MTXGlu4, and MTXGlu5 concentrations, but not MTXGlu1 and MTXGlu2, increased significantly over 24 weeks, reaching 90% of new steady-state concentrations by about 40 weeks. A decrease in DAS28 was associated with increased RBC MTXGlu5 (p = 0.035) and RBC MTXGlu3–5 (p = 0.032). No change in adverse effect frequency occurred.
Conclusion. Changing to SC MTX results in increased long-chain MTXGlun. However, it takes at least 6 months for RBC steady-state concentrations to be achieved. Increased long-chain MTXGlun concentrations were significantly associated with reduced disease activity.
Despite the introduction of new biological agents, methotrexate (MTX) remains the first-line therapy for patients with rheumatoid arthritis (RA) due to its efficacy, favorable adverse effect (AE) profile, and low cost. It is recommended that MTX begin at a low dose (10–15 mg/week), with dose escalation according to tolerability and response until the maximum dose is reached (20–30 mg/wk)1. In some patients, higher doses of MTX are associated with an increase in AE, while in other patients RA remains active despite higher MTX doses. Therapeutic options when RA fails to respond or for patients with AE associated with oral MTX include changing to or adding an alternative disease-modifying or biological agent, or changing to subcutaneous (SC) or intramuscular (IM) administration of MTX.
Lack of response to higher doses of MTX may, at least in part, result from the lower oral availability of MTX at high dose, which occurs because of the saturation of the active MTX transport mechanism within the gut2. For example, the oral availability of MTX is reduced by 13.5% at a dose of 17 mg compared to 7.5 mg3. SC or IM administration bypasses gut transport, thereby improving availability. The mean relative availability of SC and IM administration is not significantly different, suggesting that these 2 routes of administration are interchangeable4,5. Self-injection of MTX has been shown to be safe and convenient as well as time-saving and cost-saving to patients6.
Parenteral administration has been reported to reduce disease activity in patients who have an inadequate response to oral MTX7,8,9,10. Conversely, a change from parenteral to oral MTX has been associated with disease flare11. In a study of 384 MTX-naive patients, SC administration resulted in more rapid disease control, with more patients achieving an American College of Rheumatology 20 response at 24 weeks in the SC group compared to the oral MTX group (78% vs 67%; p < 0.05). Significantly more patients also achieved DAS28 < 2.8 in the SC group as compared to the oral group (34% vs 24%; p < 0.05)3,12. Although not all studies have shown improvement with parenteral compared to oral MTX administration13, the majority of studies are supportive and the parenteral route is being used increasingly.
Following administration and absorption, serum MTX concentrations fall rapidly14. MTX is transported into a variety of cells including red blood cells (RBC), white blood cells, and synoviocytes by the reduced folate carrier 1. Within the cell, glutamate moieties are added by folylpolyglutamate synthetase and MTX is retained as MTX polyglutamates (MTXGlun). Terminal MTX glutamates are removed by γ-glutamyl hydrolase, returning MTX to its monoglutamate form, which is rapidly transported out of the cell by multidrug resistance proteins. Polyglutamation results in longer retention of MTX within cells, with increased retention as the number of glutamate moieties increases15. The major determinants of MTXGlun concentrations are age, renal function, and MTX dose16. Route of MTX administration has also been reported to be an important determinant of MTXGlun concentrations in children with juvenile idiopathic arthritis (JIA)17.
It remains unclear whether there is an association between red blood cell (RBC) MTXGlu concentrations and disease activity in cross-sectional studies of patients receiving MTX for RA18,19. Further, there is no convincing evidence that MTXGlu concentrations are associated with AE in patients with RA18,20,21. However, in patients with JIA, a relationship between higher concentrations of MTXGlu3–5 and gastrointestinal AE and increased liver function tests has been reported22.
The aim of our study was to determine the effect on RBC MTXGlu concentrations of changing from oral to SC MTX in patients with RA disease activity and AE associated with MTX.
MATERIALS AND METHODS
Ethical approval was obtained from the Upper South B Regional Ethics Committee, New Zealand. Written informed consent was obtained from each patient.
Patients and study protocol
This was a 6-month study undertaken in a single center in Christchurch, New Zealand. Patients ≥ 18 years of age with RA, as defined by the American Rheumatism Association23, were recruited. Patients on stable-dose weekly oral MTX with inadequate disease control and/or AE were changed to the SC route of administration at the same MTX dose. Patients were seen for clinical assessment at baseline and Weeks 8, 16, and 24. Blood samples for measurement of trough RBC MTXGlun concentrations were collected weekly until Week 8, then fortnightly until Week 16 and then every 4 weeks until Week 24. This study was registered with the Australian and New Zealand Clinical Trials Registry (ACTRN012606000275561).
Clinical assessment
Standard demographic and clinical details were collected. Disease activity was assessed using swollen joint count (SJC), tender joint count (TJC), modified Health Assessment Questionnaire (mHAQ), physicians’ global scores, and patient pain and global scores. SJC and TJC were determined by a single trained observer to avoid interobserver variability. DAS2824 was calculated and responders were defined as having a reduction in DAS28 > 0.6.
A standardized questionnaire related to common MTX AE in the month preceding the study visit was used at Weeks 0, 8, 16, and 24. AE were self-reported symptoms and grouped into 3 categories: (1) gastrointestinal (nausea, vomiting, diarrhea, mouth ulcers, and decreased appetite); (2) central nervous system (fatigue, loss of concentration, headache, dizziness, blurred vision, sleep disturbance, and weepiness); and (3) other (hair loss, cough, fever, and shortness of breath).
Laboratory measurements
These assessments included full blood count, creatinine and liver function tests, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Estimated creatinine clearance (eGFR; glomerular filtration rate) was calculated using the Modification of Diet in Renal Disease study equation25. Total RBC folate was measured using the Abbott Architect Folate Assay (Abbott Laboratories, Abbott Park, IL, USA).
Trough RBC MTXGlun concentrations were measured by high-performance liquid chromatography, as described26. All samples were analyzed in duplicate and the mean concentration of each RBC MTXGlun from each sample was used.
Pharmacokinetic analysis
A subgroup of patients, representing the majority, who changed from oral MTX 20 mg/week to SC MTX 20 mg/week and had no change in MTX dose during the study period were used for the pharmacokinetic analysis. Median MTXGlu concentrations for all patients at each timepoint were graphed and analyzed using GraphPad Prism 5 Software (San Diego, CA, USA; www.graphpad.com). A first-order exponential model [C = C0 + (plateau – C0)*(1 – exp(–k*t)] was fitted to the data to calculate a half-life of accumulation (ln2/k) and goodness-of-fit was calculated. Visual and statistical analysis of the accumulation curves confirmed that the first-order exponential model was appropriate. Using the accumulation rate constant in the first-order exponential model, as calculated in GraphPad Prism 5, the time for each RBC MTXGlun to reach 90% of the modeled maximum concentration was calculated.
Statistical analysis
Statistical analyses were undertaken using SPSS Version 17. The changes in concentrations and proportions of MTXGlu from Week 0 to Week 24 and changes in disease activity were tested using the nonparametric Wilcoxon signed-rank test. The changes from Week 0 to Week 24 in laboratory variables were tested using paired t tests. Where patients did not complete a 24-week study visit, the last study visit observations were carried forward. The associations between the changes in RBC MTXGlu concentrations and disease activity measures from Week 0 to Week 24 were tested using Spearman’s correlation coefficient. The change in MTXGlu concentrations from Week 0 to Week 24 was compared between responders and nonresponders using Mann-Whitney U tests. The changes in MTXGlu concentrations over all time periods were compared between responder and nonresponder groups using mixed-effect linear models. These models included individual patient as a random effect, and time as a continuous measure nested within patients with an unstructured covariance matrix; additionally, a term testing the interaction between time and responders group was included. A 2-tailed p value < 0.05 was taken to indicate statistical significance.
RESULTS
Demographics
Thirty-two patients were recruited between October 2005 and February 2008. Two patients who discontinued SC MTX after 1 dose were excluded, leaving 30 patients in the analysis. Of these 30 patients, 76.7% were women, the mean age was 51.8 years (range 32–70 yrs), and 90% were New Zealand European. The mean duration of RA was 7.7 years (range 0.75–21 yrs). Rheumatoid nodules were seen in 16.7% of the patients; 56.7% had radiographic erosions, 86.7% were rheumatoid factor-positive, and 92.9% were positive for anticyclic citrullinated peptide antibodies. The median dose of MTX was 20 mg/week (range 10–20 mg/wk) and all patients received folic acid 5 mg/week, taken 3–4 days after MTX. Patients had been receiving MTX for a median of 39.5 months (range 6–144 mo) prior to study entry, and receiving the dose of MTX at study entry for a median of 7 months (range 1–106 mo). Sixteen out of 30 patients (55.3%) were receiving nonsteroidal antiinflammatory drugs (NSAID), 17/30 (56.7%) another disease-modifying antirheumatic drug (DMARD), 8 salazopyrin and hydroxychloroquine (HCQ), 5 HCQ alone, 2 leflunomide (LEF), 1 both LEF and HCQ, and 1 adalimumab. Thirteen out of 30 (43.3%) were receiving oral prednisone at a mean dose of 9.8 mg/day (range 2.5–25 mg/day). Characteristics of the responders and nonresponders are outlined in Table 1. There was no significant difference in use at baseline of NSAID, prednisone, or other DMARD between responders and nonresponders.
Demographics of the whole cohort, responders, and nonresponders.
The dose of MTX during the study period was 10 mg/week in 1 patient, 12.5 mg/week in 1 patient, 15 mg/week for 4 patients, and 20 mg/week in 25 patients. No patients had the dose changed during the study period.
One patient was noncompliant with SC MTX therapy as determined by a gradual decline in RBC MTXGlun concentrations, and 2 patients discontinued SC MTX at Week 16 (1 because of lack of improvement and 1 because of AE), leaving 27 patients in this analysis.
Effect on RBC MTXGlun concentrations of changing from oral to SC MTX
There was a significant increase in RBC MTXGlu3, MTXGlu4, MTXGlu5, MTXGlu3–5, and MTXGlu1–5 concentrations from Week 0 to Week 24 but no significant increase in MTXGlu1 or MTXGlu2 concentrations (Figure 1). There was a significant reduction in the proportion of RBC MTXGlu1 and MTXGlu2 and an increase in the proportions of RBC MTXGlu4, MTXGlu5, and MTXGlu3–5 contributing to the total MTXGlu from Week 0 to Week 24 (Figure 2).

RBC MTXGlu concentrations on oral MTX (Week 0) and after 24 weeks on SC MTX (Week 24).
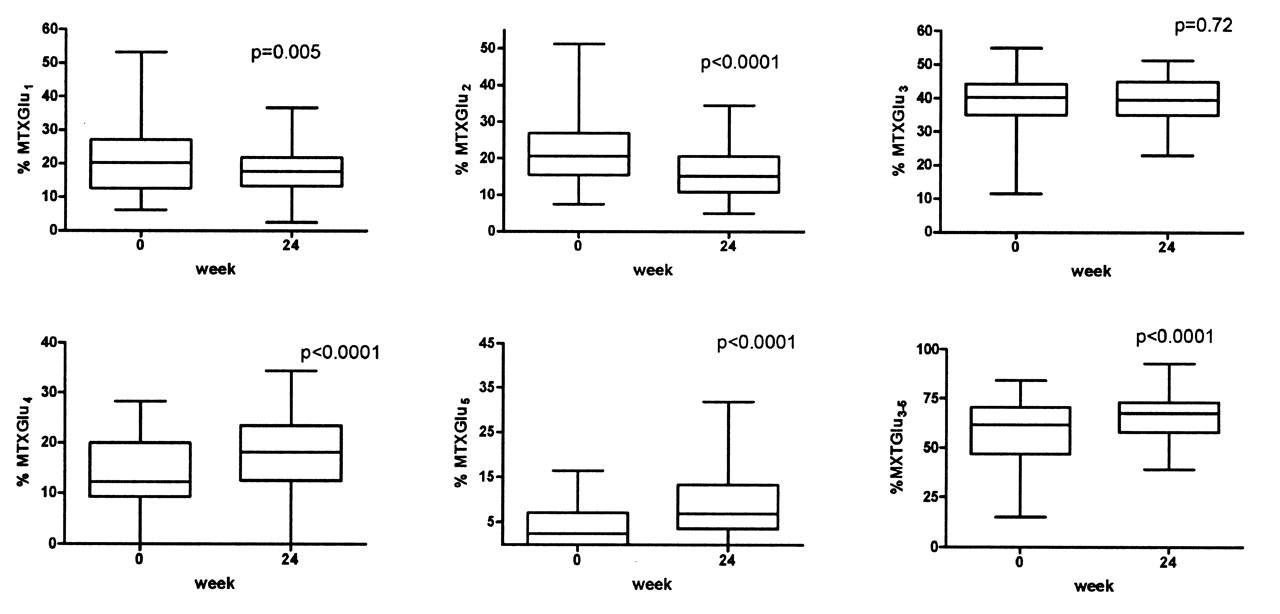
The percentage of each MTXGlu contributing to the total on oral MTX (Week 0) and after 24 weeks on SC MTX.
Pharmacokinetic modeling of RBC MTXGlu concentrations after changing from oral to SC MTX
Pharmacokinetic analysis was undertaken in the subgroup of 22 patients who changed from oral MTX 20 mg/week to SC MTX 20 mg/week and had no change in MTX dose during the study period. MTXGlu3, MTXGlu4, MTXGlu5, and MTXGlu3–5 concentrations fit the first-order exponential accumulation model well, while MTXGlu1 and MTXGlu2 fit poorly (Figure 3). The half-life of accumulation was 8.9 weeks for MTXGlu3, 12.2 weeks for MTXGlu4, 9.9 weeks for MTXGlu5, and 10.4 weeks for MTXGlu3–5. The time to achieve 90% of steady state was 29.8 weeks for MTXGlu3, 40.4 weeks for MTXGlu4, 33.2 weeks for MTXGlu5, and 34.5 weeks for MTXGlu3–5.

Median MTXGlu concentrations in 22 patients changing from oral to SC MTX. Median MTXGlu at each timepoint is plotted, with the curve fit to a nonlinear exponential accumulation (first-order) model, calculated using GraphPad Prism 5.
Effect of changing from oral to SC MTX on disease activity measures
In the group as a whole there was an improvement in the following disease activity variables between Week 0 and Week 24 [median (interquartile range); SJC 2 (0–4) vs 0 (0–2; p = 0.001)], pain visual analog scale 24.5 (10–47.8) vs 17 (9.5–25.8; p = 0.014), patient global score 29.5 (17–52.3) vs 16 (7.5–32.3; p = 0.04), and mHAQ 0.25 (0–0.687) vs 0.125 (0–0.375; p = 0.03). There was a trend toward improvement in DAS28 [3.27 (2.02–3.85) vs 2.56 (1.92–3.590); p = 0.064]. There was no significant improvement in TJC, patient fatigue, CRP, or ESR (data not shown). Of the 26 patients with complete DAS28 scores, the mean change in DAS28 from Week 0 to Week 24 was 0.47 (range −1.5 to 5.19).
Association between change in RBC MTXGlun concentrations and change in disease activity variables
There was a statistically significant correlation between a reduction in DAS28 and an increase in RBC MTXGlu5 and MTXGlu3–5 concentrations (Table 2). However, the correlation was modest at best and the clinical significance unclear. The improvement in DAS28 from Week 0 to Week 24 was ≤ 0.6 in 16 patients (nonresponders) and > 0.6 in 10 patients (responders). There was no significant difference in RBC MTXGlun concentrations between responders and nonresponders (p > 0.05 for all) at Week 0 or 24. However, there was a significantly greater increase in MTXGlu5, MTXGlu3–5, and MTXGlu1–5, and a trend toward a greater increase in MTXGlu4 between Week 0 and Week 24 in the responders compared to nonresponders (Table 3). Further analysis revealed that the earliest time at which the difference in the change in MTXGlu1–5 concentrations was statistically significant was 12 weeks after changing to SC MTX (Figure 4). At Week 12 the mean increase in MTXGlu1–5 in nonresponders was 23.1 nmol/8*1012 RBC compared to 64.5 nmol/8*1012 RBC in responders (p = 0.01). However, the change in MTXGlu3 was not significant (p = 0.18).
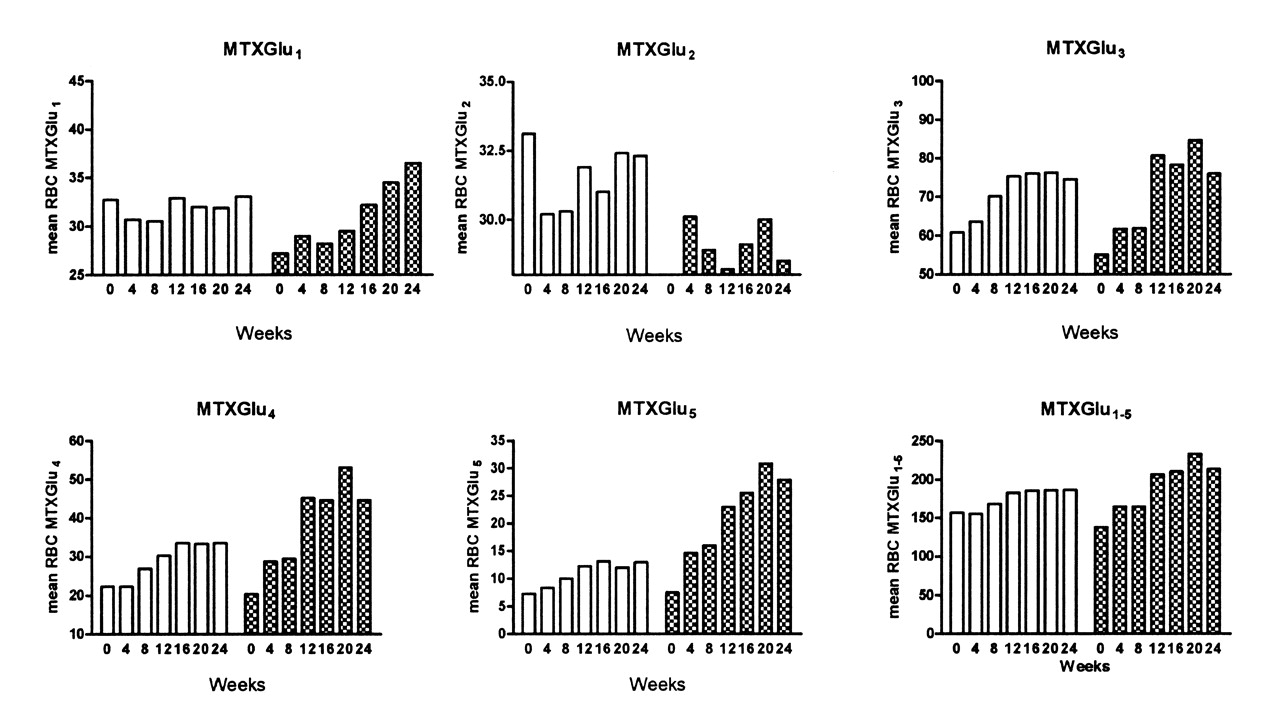
Mean RBC MTXGlu over 24 weeks after changing from oral to SC MTX in responders (ΔDAS > 0.6; shaded bars) compared to nonresponders (ΔDAS ≤ 0.6; white bars).
Relationship between change in disease activity variables and change in red blood cell polyglutamate concentrations.
Median change (interquartile range) in red blood cell MTXGlun concentration between Week 0 and Week 24 in responders (∅DAS28 > 0.6) and nonresponders (∅DAS28 ≤ 0.6).
No patients began additional DMARD or steroids during the study period. However, a small number were able to reduce steroids and NSAID because of response to MTX.
Responders had a higher mean DAS28 at baseline compared to nonresponders (4.0 ± 0.42 vs 2.6 ± 0.32; p = 0.011). All patients with a DAS28 > 3.0 at baseline responded to a change to SC administration of MTX, with a decrease in DAS28 > 0.6.
Effect of changing from oral to SC MTX on laboratory variables
There was no significant change from Week 0 to Week 24 in hemoglobin (mean ± SD; 129.9 ± 11.3 g/l vs 128.3 ± 11.8 g/l; p = 0.08), alanine aminotransferase (25.3 ± 13.6 U/l vs 29.5 ± 15.9 U/l; p = 0.58), aspartate aminotransferase (21.7 ± 7.2 vs 23.7 ± 8.3; p = 0.66), albumin (43.1 ± 5.2 vs 44.4 ± 2.3; p = 0.21), or eGFR (83.1 ± 14.1 vs 84.2 ± 20.3; p = 0.35). There was a significant reduction in platelet count between Week 0 and Week 24 (306.4 ± 73.5 × 109/l vs 288.5 ± 69.4 × 109/l; p = 0.006) and an increase in mean RBC volume (93.2 ± 4.6 fl vs 94.1 ± 4.9 fl; p = 0.04). There was a trend toward a reduction in neutrophil count (5.2 ± 2.2 × 109/l vs 4.5 ± 1.5 × 109/l; p = 0.065), but not below the lower limit of normal (< 1.9 × 109/l).
There was no significant change in RBC folate from Week 0 to Week 24 (550.2 ± 383.2 nmol/l vs 604.3 ± 468.9 nmol/l; p = 0.29) in the group as a whole. There was an increase in RBC folate between Week 0 and Week 24 in the nonresponders (553 vs 653 nmol/l) and a decrease in RBC folate between Week 0 and Week 24 in the responders (586 vs 559 nmol/l). However, there was no significant difference in the change between responders and nonresponders (p > 0.05).
Association between change to SC MTX and MTX AE
There was no significant change in the number of patients with each of the AE between Week 0 (oral MTX) and after 24 weeks of SC MTX (data not shown). However, of the 6 patients who entered the study because of AE, 5 had a reduction in AE and 1 had an increase in AE after changing to SC administration of MTX.
DISCUSSION
MTX remains the first-line therapy for RA and in many countries patients must have RA that failed to respond to MTX as monotherapy and/or in combination with other DMARD before publicly funded biological therapies can begin. In the majority of cases, MTX is given orally, although it has been suggested that the SC route should be tried as a prerequisite to biological therapy9,27; this has not been widely accepted. We examined the effects on RBC MTXGlun concentrations, disease activity, and AE of changing from oral to SC MTX.
We have previously described the pharmacokinetics of oral MTX in RA15. In our study, changing from oral to SC MTX resulted in an alteration in the ratio of short- and long-chain MTXGlun, with a significant increase in the proportion of long-chain MTXGlun (MTXGlu4 and MTXGlu5). This alteration in ratio of long- and short-chain MTXGlun has been described. In a cross-sectional study of 99 patients with JIA, higher MTXGlu3–5 concentrations were reported in patients receiving SC MTX compared to those receiving oral MTX at the same dose17. In another smaller study of 10 patients with active RA, patients were switched from oral to SC MTX administration, resulting in increased MTXGlu4 and MTXGlu5 concentrations28.
Modeling of MTXGlun concentrations showed that after changing from oral to SC MTX, it took at least 6 months for long-chain MTXGlun to reach 90% of steady state. This is less than the time to reach steady state in patients commencing oral MTX, where it has been reported that the median to reach 90% of steady state in RBC was 6.2, 10.6, 41.2, 149, and 139.8 weeks, respectively, for MTXGlu1 to MTXGlu515. This may explain, at least in part, why patients starting on SC MTX achieve a more rapid response than those starting on oral MTX3,12. The shorter duration to achieve 90% of steady state with SC administration may reflect increased and more stable drug availability with SC as compared to oral administration. The better goodness-of-fit of the accumulation model seen with the long-chain MTXGlun probably reflects the greater accumulation of these polyglutamates compared to the short-chain polyglutamates. The greater accumulation may reflect greater stability of the long-chain MTXGlun in RBC because of the inability to cross the cell membrane, and longer half-life15.
While time to achieve steady state is less with SC administration, it still is a significant delay in an era where rapid disease control is desired. However, it would appear that in patients whose disease responds to the change to SC MTX, the increase in MTXGlun occurs more rapidly than in those patients whose disease does not respond after 6 months. Further analysis reveals that the earliest timepoint where the difference between responders and nonresponders is apparent is 12 weeks. This delay until efficacy is acceptable in the current clinical environment in which the majority of DMARD and biological agents require a similar timeframe for efficacy to be apparent. However, further studies in larger cohorts will be required to confirm the validity of making a clinical decision of changing therapy from SC MTX at 12 weeks in nonresponders.
The exact mechanisms underlying why patients respond to the change from oral to SC MTX remain unclear. There are likely a variety of effects including increased bioavailability with the SC vs oral route of administration, faster efflux of MTXGlu1 and MTXGlu2 from cells in nonresponders resulting in decreased substrate for conversion to the longer-chain polyglutamates, and genetic variation in enzymes involved in the transport and metabolism of MTX between responders and nonresponders.
Interestingly, we have shown no difference in the final mean MTXGlun concentrations between responders and nonresponders to SC MTX at 24 weeks. While we have previously reported a similar finding in a cross-sectional study of patients with RA, others have reported that patients responding to MTX have higher long-chain MTXGlun concentrations18,19. However, in our current study we have also shown that an improvement in DAS28 is associated with an increase in RBC MTXGlu5 and MTXGlu3–5 concentrations. Further, the increase is greater in patients whose disease responds to a change to SC MTX compared to nonresponders. This increase in the longer-chain MTXGlun has been suggested to result in the observed clinical improvements28. While we cannot define a therapeutic range from the data, this provides further evidence that the long-chain polyglutamates are the most important in determining the clinical effect of MTX. This is in keeping with the increase in potency of the longer-chain polyglutamates in inhibiting enzymes in the folate pathway and 5-aminoimidazole-4-carboxamide ribonucleotide transformylase, which are responsible for the antiinflammatory effects of MTX29. However, the correlation between DAS28 and long-chain MTXGlun was modest and thus the clinical importance of the observed correlation remains unclear.
In our cohort, 10 out of 26 (38.5%) patients had a response as defined by a decrease in DAS28 > 0.6. All patients with a DAS28 > 3.0 responded to a change to SC MTX with a reduction in DAS28. This may reflect those patients with more active disease (i.e., DAS28 > 3.0) responding in a relatively stronger fashion compared to those patients with less active disease. Although there was a trend toward a statistically significant reduction in DAS28 in the group as a whole, the absolute change in DAS28 was small. This reflects the poorer response in those patients who changed to SC MTX when their disease was reasonably controlled (DAS28 ≤ 3.0). These data provide some evidence for the clinical benefit of changing route of administration in patients with active RA, even in patients who have been taking MTX for some time. While the number of patients in our study was small, larger studies have shown similar results, with a reduction in disease activity with a change to SC MTX administration30.
We have shown no change in the AE profile between oral and SC MTX administration in the group as a whole. However, for 6 patients who entered the study because of AE, 5 had a reduction in AE. The data regarding AE in patients receiving SC MTX is variable. Wegrzyn, et al reported reduced gastrointestinal AE associated with parenteral MTX10, while others reported no difference in tolerability30. Of note, MTX pneumonitis has been reported to commence 4 weeks after changing route in a patient who had been on oral MTX for 2 years31. The authors suggest that the dose of MTX should be reduced by 2.5 mg when the change to SC administration is made. However, there is no evidence that such an approach will prevent severe AE. Although there is currently no evidence to support an association between less serious MTX AE and MTXGlun concentrations in patients with RA18, it remains unknown whether the more severe AE that necessitate discontinuation of MTX, such as pneumonitis and bone marrow failure, are related to increased MTXGlun concentrations. However, gastrointestinal AE and abnormal liver function tests have been associated with high MTXGlun concentrations in children with JIA22.
Changing from oral to SC MTX results in a significant change in the MTXGlun profile, with increased proportions of the long-chain polyglutamates. In those patients with a DAS > 3.0, clinical improvement may be observed. The clinical utility of measuring the MTXGlun profile to predict response in this setting merits further study.
Acknowledgment
We gratefully acknowledge the assistance of Jan Ipenburg, Rheumatology Clinical Nurse Specialist, with patient data collection.
Footnotes
-
Supported by the Health Research Council of New Zealand and Arthritis New Zealand.
- Accepted for publication July 20, 2011.








{kind=link}
{kind=link}
{kind=link}
{kind=link}