

Abstract
Objective. To investigate whether the frequency of peripheral blood (PB) regulatory T cells (Treg) correlates with the clinical disease activity of rheumatoid arthritis (RA).
Methods. PB Treg cells, defined as the CD4+CD25highCD127low/- population, were examined by flow cytometry in 48 patients with RA, including 13 who had never received disease-modifying antirheumatic drugs (DMARD), 19 with active disease who were receiving (n = 14) or had received (n = 5) DMARD, and 16 receiving DMARD whose disease was in remission. The clinical disease activity of the patients was defined by the 28-joint Disease Activity Score (DAS28). The association of DAS28, C-reactive protein (CRP), or erythrocyte sedimentation rate (ESR) with the frequency of PB Treg cells was examined.
Results. The frequency of PB Treg cells in patients with RA was significantly low compared with that of healthy controls (n = 14). Among the 3 populations of patients with RA, Treg cell frequency was lowest in patients with active RA. In contrast, the Treg cell frequency of patients with RA in remission was similar to that of healthy controls. Accordingly, the frequency of CD4+CD25highCD127low/- Treg cells negatively correlated with DAS28, CRP, and ESR in patients with RA.
Conclusion. The data suggest that Treg cells, defined as the CD4+CD25highCD127low/- population, may contribute to the pathogenesis of RA and be an indicator of disease activity.
CD4+ regulatory T cell (Treg)-cell deficiency or absence is known to correlate with the development or exacerbation of autoimmune diseases, implying a crucial role for Treg cells in maintaining immunological self-tolerance1,2. In recent years, Treg cell counts and function have also been examined in patients with rheumatoid arthritis (RA)3,4,5,6,7,8. Treg cell function in patients with active RA is assumed to be impaired, a trend that seems to be reversed by tumor necrosis factor (TNF) antagonist therapy6,7; however, Treg cell counts in peripheral blood (PB) have varied across studies3,4. These discrepancies can probably be ascribed to differences in the labeling and definition of CD4+CD25+ T cells9. Among CD4+CD25+ T cells, those exerting suppressive effects9,10 are only those expressing large amounts of CD25, e.g., CD4+CD25high T cells, which highly express forkhead box P3 (FOXP-3). The intracellular staining process for FOXP-3 is somewhat time-consuming as compared with cell surface staining in clinical practice; thus, a more convenient marker on the cell surface closely correlating with FOXP-3 expression is awaited. In this regard, Saleem, et al recently reported that the frequency of CD62L+ Treg cells in PB from RA is associated with sustained remission during TNF antagonist therapy11.
Another candidate cell surface molecule for the identification of Treg cells is CD127. Two recent studies have demonstrated that downregulation of the interleukin (IL)-7 receptor α chain, CD127, distinguishes Treg cells from activated T cells, demonstrating a significant correlation between the FOXP-3 and CD127low/- phenotype at the same time that it functionally suppresses the CD127low/- population12,13.
We examined whether the frequency of Treg cells correlates with the clinical disease activity of RA by staining cells with CD4, CD25, and CD127. The frequency of CD4+CD25highCD127low/- Treg cells negatively correlated with the 28-joint Disease Activity Score (DAS28), C-reactive protein (CRP), and the erythrocyte sedimentation rate (ESR). This is a more convenient method of detecting Treg cells in clinical practice and may follow the data of Saleem, et al11, suggesting that Treg cells contribute to the pathogenesis of RA.
MATERIALS AND METHODS
Study population
Patients with RA (n = 48) and healthy controls (n = 14) were included in our study. All of the patients fulfilled the 1987 criteria of the American College of Rheumatology for RA14. All patients were seropositive for rheumatoid factor and/or anticitrullinated protein antibodies. Informed consent was obtained from all patients and controls. The Institutional Review Board of Nagasaki University approved the study. Clinical response to the therapy was evaluated by DAS28 (high disease activity > 5.1, moderate disease activity < 5.1 and > 3.2, low disease activity < 3.2, remission < 2.6). Patients were divided into 3 groups: (1) those naive to disease-modifying antirheumatic drugs (DMARD; n = 13); (2) those with active RA (n = 19) whose disease activity was moderate (DAS28 > 3.2), including both those who were receiving (n = 14) or had received (n = 5) DMARD; and (3) those whose disease was in clinical remission (DAS28 < 2.6) with concomitant use of DMARD (n = 16). All patients in the group with active RA and the remission group were on stable therapy. Patient characteristics are shown in Table 1. For the controls, the median (range) of age was 34.5 (27–50) years and the sex ratio was 4:10 (men:women). They were statistically younger than patients with RA. We examined a correlation of age and each population of T cell frequency among 14 controls by Spearman’s rank correlation and did not find any association (data not shown).
Patient characteristics. Within-group comparisons were made using the Mann-Whitney U test and the chi-squared test (Fisher’s exact probability test when appropriate).
Cell isolation and analysis by flow cytometry
Peripheral blood samples were collected in heparin. Peripheral blood mononuclear cells (PBMC) were isolated by standard Ficoll-Hypaque density centrifugation and used for flow cytometry. Freshly isolated PBMC were stained with 3 colors: FITC-labeled CD4; PE-Cy5-labeled CD25 and PE-labeled CD127; or PE-Cy5-labeled CD4, PE-labeled CD25, and FITC-labeled FOXP-3 (clone: PCH101, intracellular staining) by the standard protocol. All antibodies were products of eBioscience (San Diego, CA, USA). For flow cytometric analysis, lymphocytes were gated morphologically.
Statistical analyses
Within-group comparisons were made using the Mann-Whitney U test. Changes from the baseline were compared using Wilcoxon’s signed-rank test. Correlations were assessed with Spearman’s correlation coefficient test. The overall significance level for statistical analysis was 5% (2-sided). P values < 0.05 were considered statistically significant.
RESULTS
Patient characteristics are shown in Table 1. CRP, ESR, and DAS28 in the remission group were significantly lower than in the other 2 groups. CRP and ESR in the patients with active RA who were receiving or had received DMARD were significantly higher than those of DMARD-naive patients with RA, but DAS28 was not significantly different between the 2 groups.
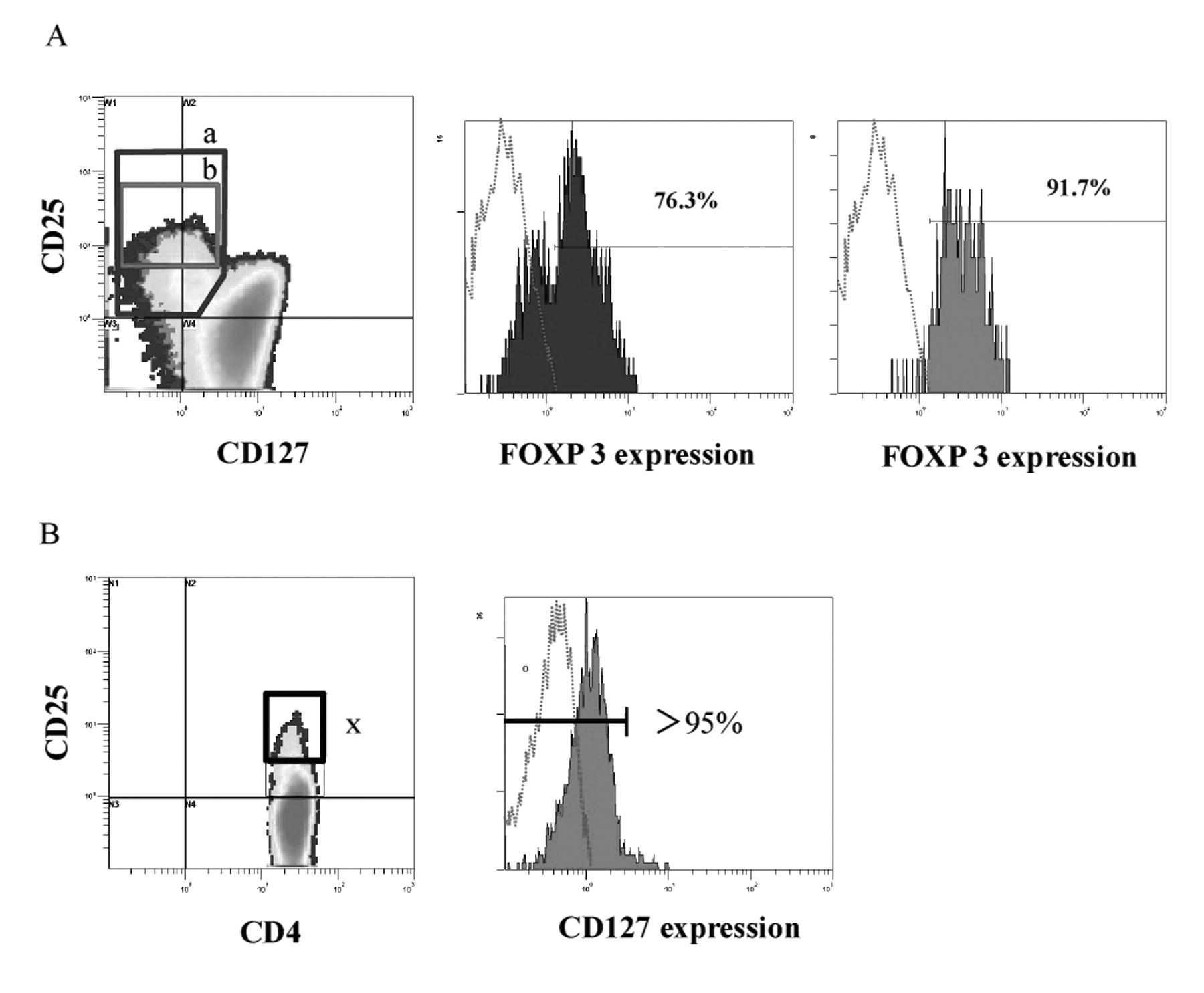
Although most CD4+CD25+CD127low/- T cells were positive for FOXP-3, a portion of this population was negative for FOXP-3 (Figure 1A). On the other hand, almost all CD4+CD25highCD127low/- T cells were positive for FOXP-3 (Figure 1A).
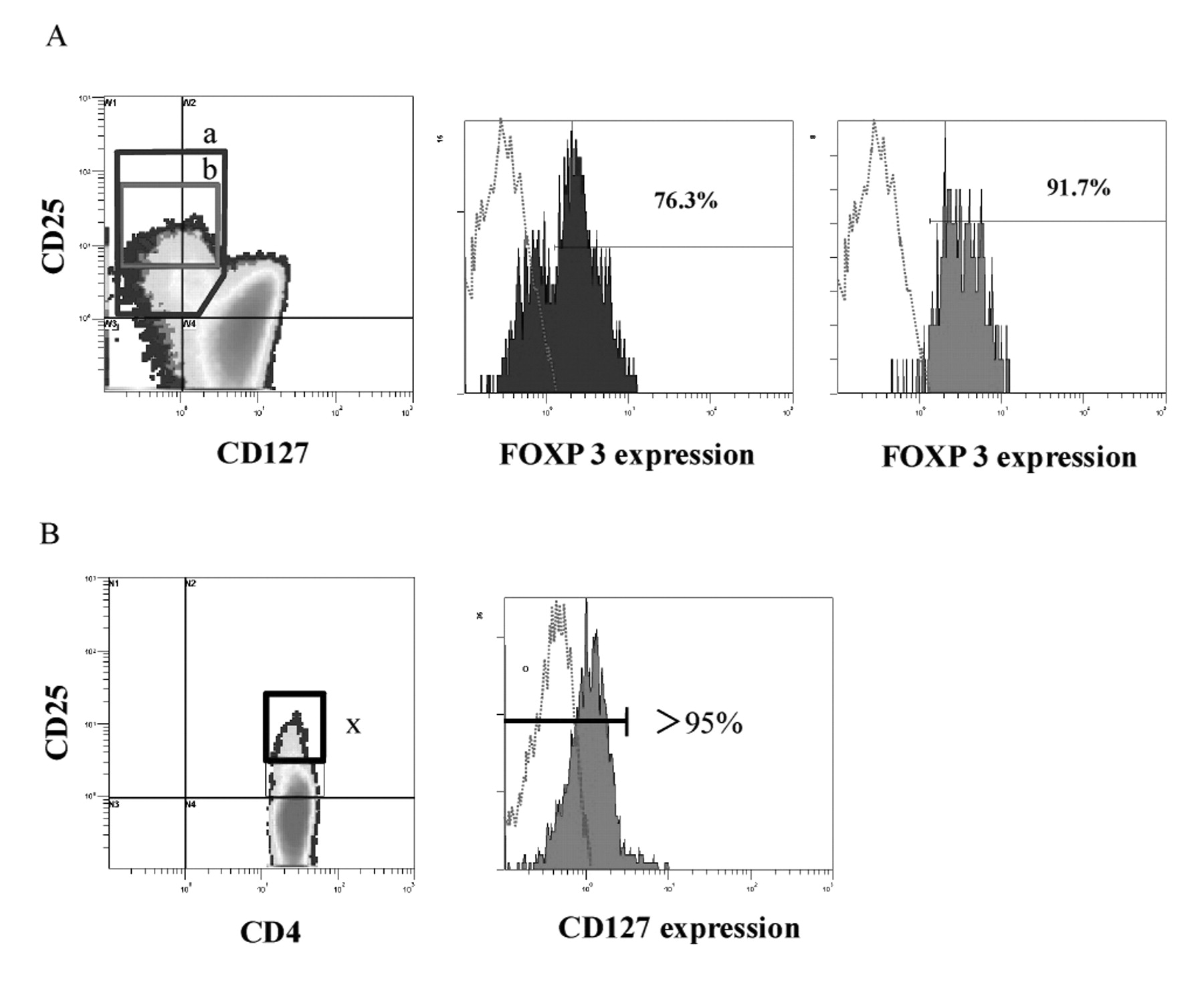
The CD4+CD25highCD127low/- population as the phenotype of Treg cells. The graphs show representative data of several healthy samples. A. Plots are gated for CD4+ T cells. CD25+CD127low/- cells and CD25highCD127low/- cells are found in box a and box b. Expressions of FOXP-3 in boxes a and b are shown in the second and third panels. B. Mononuclear cells were stained for CD4, CD25, and CD127. Plots are gated for CD4+ T cells. The CD4+CD25high population, with the cutoff of CD127 expression at < 5% among CD4+ T cells (right side), is boxed as CD4+CD25highCD127low/- T cells (left side, box x). Box x is individually adjusted.
Phenotypes of peripheral blood CD4+ T cells of patients with RA and controls were compared (Table 2). There were no significant differences in the frequencies of CD4+CD25– T cells and CD4+CD25+ T cells between DMARD-naive patients with RA and healthy volunteers. The frequency of CD4+CD25+CD127low/- T cells (Figure 1A) was significantly lower in the patients with active RA who were receiving or had received DMARD than in controls (p < 0.05).
Phenotype of peripheral blood CD4+ T cells in patients with rheumatoid arthritis (RA) and in healthy controls. Data are percentage of CD4+ T cells; median (range). Within-group comparisons were made using the Mann-Whitney U test.
We counted the frequency of CD4+CD25highCD127low/- T cells, using the cutoff value of < 5% CD127 expression among CD4+ T cells (Figure 1B). We have adopted this method to identify the CD4+CD25highCD127low/- T cells accurately in each individual. The frequency of this population was lower in the DMARD-naive RA patient group than in the healthy controls (p < 0.01), and was lower in the active RA group taking DMARD than in the DMARD-naive RA group (p < 0.01). Further, the frequency of this population was higher in the remission group than in the active RA group with DMARD (p < 0.0001).
We investigated the correlation between the phenotype of peripheral blood Treg cells and the markers of disease activity such as CRP, ESR, and DAS28 in the 48 patients with RA (Table 3). The frequencies of CD4+CD25+ T cells and CD4+CD25+CD127low/- T cells were not correlated with disease activity. However, the frequency of CD4+CD25high-CD127low/- T cells was negatively correlated with CRP, ESR, and DAS28, respectively (p < 0.0001).
The correlations between regulatory T cells (Treg) and rheumatoid arthritis (RA) disease activity in 48 patients with RA. The correlations were assessed using Spearman’s correlation coefficient test.
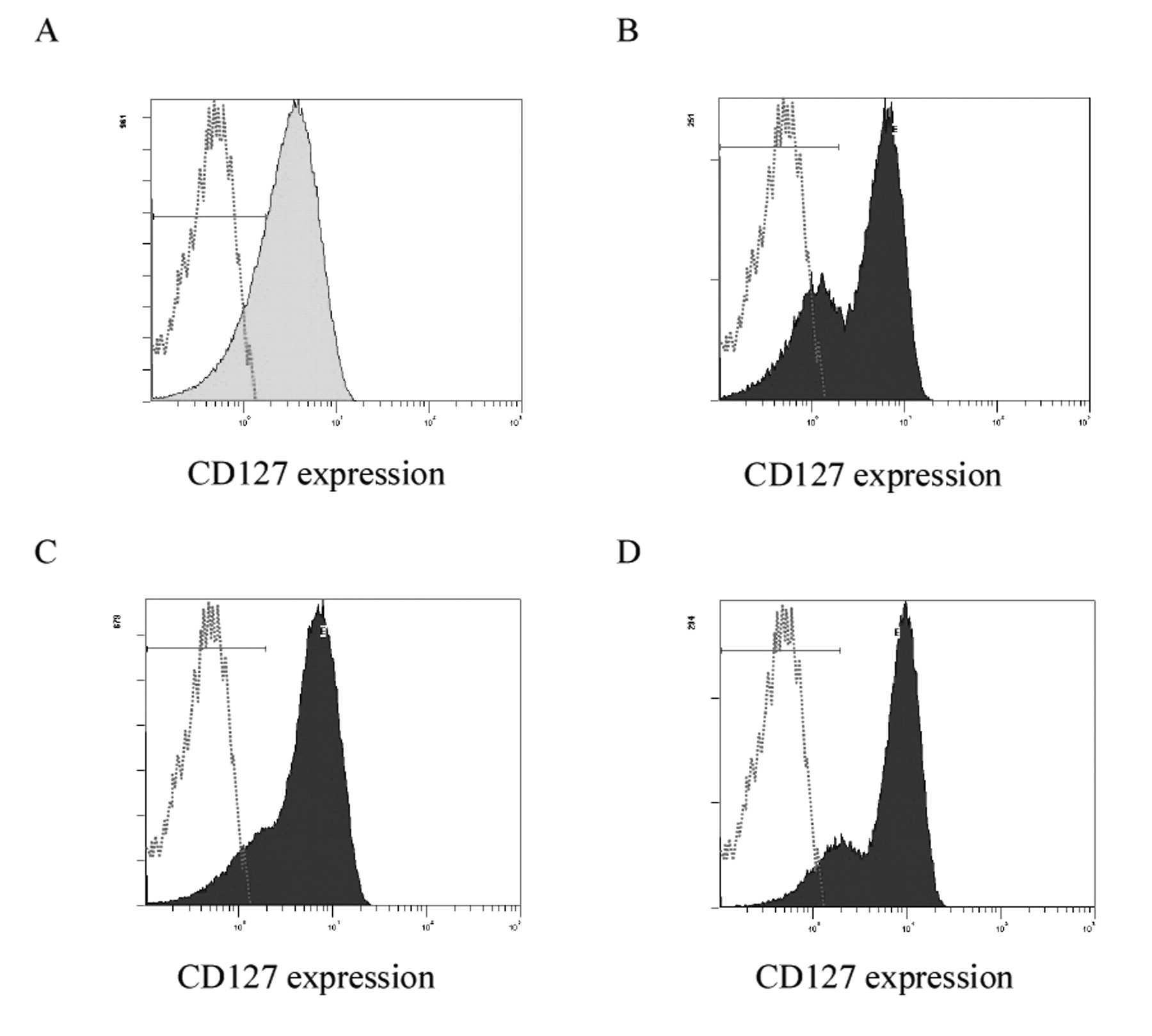
As mentioned, CD4+ T cells were almost all positive for CD127 (Figure 2A); however, a large CD127low/- population was detected among CD4+CD25+ T cells in healthy individuals (Figure 2B). In patients with RA, the expression of this population was lower than in healthy individuals (Figure 2C), but it recovered after the disease went into clinical remission (Figure 2D).

Changes in the proportion of the CD127low/- population among CD4+CD25+ T cells. Expression of CD127 among CD4+ T cells (A) and CD4+CD25+ T cells (B–D) are shown. Panels A and B describe peripheral blood mononuclear cell (PBMC) samples collected from healthy individuals. Although CD4+ T cells are likely almost all positive for CD127 (A), the expression of CD127 among CD4+CD25+ T cells is differential, with both CD127low/- cells and CD127+ cells in healthy controls (B). Panels C and D describe PBMC samples collected from a patient with early RA (male, disease duration 3 months). The proportion of CD127low/- cells among CD4+CD25+ T cells decreased before this patient was treated (28-joint Disease Activity Score 4.27, panel C). After this patient’s disease went into clinical remission by treatment with bucillamine, the expression of CD127 among CD4+CD25+ T cells recovered to nearly the same level as that in healthy controls (D). The frequencies of CD4+CD25highCD127low/- cells were 5.73% before therapy and 7.21% after clinical remission.
DISCUSSION
Recent data obtained from patients with RA during TNF-antagonist therapy have suggested that TNF downmodulates the function of human CD4+CD25+ Treg cells6,7,8. Therefore, Treg cells may dynamically fluctuate, depending on the disease status of RA, and reflect the disease activity of RA. We have focused on a convenient cell surface staining method to identify Treg cells and tried to investigate the association of Treg cell frequency with the disease activity of RA.
CD25 and CD127 were used to identify the Treg cell population in our study. Since FOXP-3 is strongly expressed in CD4+CD25highCD127low/- population, CD4+CD25high- CD127low/- cells can be estimated as Treg cells12,13. Additionally, the clinical differences between patients with RA and controls as well as the clinical measures among patients with RA were most predominantly found in the CD4+CD25highCD127low/- population. We have set the cutoff of CD127 expression at < 5% in the individual case; thus, our definition may correctly identify the frequency of naturally arising Treg cells (Figure 3). The controls were younger than the patients with RA in our study. Although there was no correlation between Treg cell frequency and age of the control, a previous study4 demonstrated a weak negative correlation between age and Treg cell frequency. The use of glucocorticoids was more frequent in the active RA group as compared with the DMARD-naive RA group, as well as the remission group. The influence of glucocorticoids regarding the function or number of Treg cells might be controversial15,16. Therefore, age-matched studies involving glucocorticoid-naive patients are necessary to confirm our results.
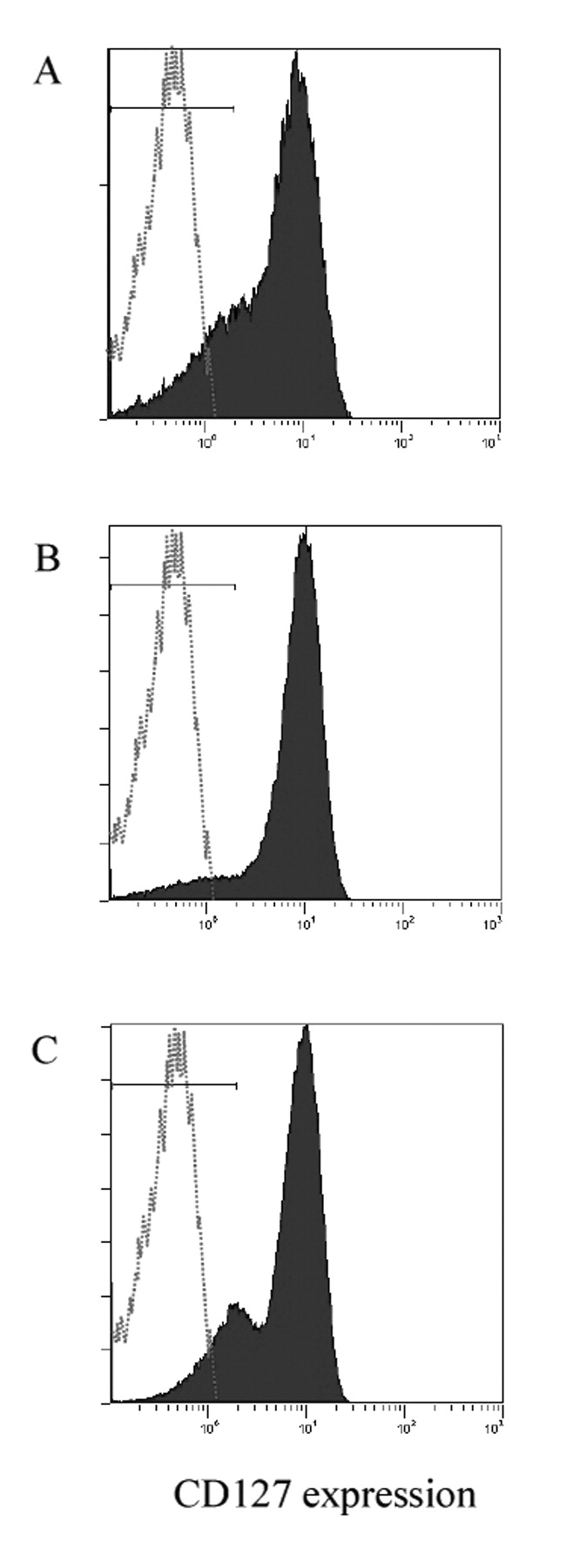
The proportion of the CD127low/- population among CD4+CD25+ T cells in the 3 RA groups. A. The group naive to disease-modifying antirheumatic drugs. B. The group with active RA. C. The remission group. Expressions of CD127 among CD4+CD25+ T cells are shown. The frequencies of CD4+CD25+CD127low/- cells were 3.28%, 2.24%, and 5.77% in panels A, B, and C, respectively.
DMARD may alter the function of T cells in patients with RA. However, we have found that Treg cell frequency may depend not on the use of DMARD but on the RA disease activity. The Treg cell frequency was lowest in patients with active RA, while that of patients with RA in remission was similar to that of controls, despite the administration of DMARD in both groups. In addition, the Treg cell frequency was not statistically different between DMARD-naive patients with RA and patients receiving DMARD whose RA was in remission, and an inverse correlation was found between the disease activity of RA and the Treg cell frequency. In fact, we found fluctuation of Treg cell frequency depending on the disease activity. The difference of our study as compared with previous reports is to estimate Treg cells as FOXP-3bright cells. As shown in previous reports3,4, the difference of CD4+CD25+ T cell frequency between the patients with RA and controls was not significant. In addition to CD127, a similar result is obtained when estimating Treg cells as CD62 ligand+ FOXP-3bright cells11. Since we have not performed followup analysis of Treg cell frequency in each case, a prospective followup study should be performed to establish that the CD4+CD25highCD127low/- Treg cell population does in fact reflect changes in the disease activity of RA. Further examinations, including studies with a larger number and with followup observation, are needed to confirm our findings.
- Accepted for publication July 26, 2011.








{kind=link}
{kind=link}
{kind=link}