

Abstract
Objective. To evaluate the risk of reactivation of resolved hepatitis B virus (HBV) by immunosuppressive therapy in patients with autoimmune diseases.
Methods. Thirty-five patients with autoimmune diseases were included in our study; all were hepatitis B surface antigen (HBsAg)-negative and antibody against hepatitis B core antigen-positive. They were followed for 8–124 weeks and clinical outcomes were analyzed, including serum levels of HBV-DNA and aminotransferase every 4 weeks during their immunosuppressive therapy for underlying autoimmune diseases. If HBV-DNA was detected during the immunosuppressive therapy, HBsAg, antibody against HBsAg (anti-HBs), hepatitis B e antigen (HBeAg), and antibody against HBeAg were also monitored every 4 weeks.
Results. HBV-DNA was detected in 6 out of 35 patients. Anti-HBs titer was significantly lower in the patients in whom HBV-DNA was detected compared with the others at baseline: 2.83 (range 0.24–168.50) mIU/ml vs 99.94 (range 0.00–5342.98) mIU/ml, respectively (p = 0.036). Outcomes of the 6 patients with HBV reactivation were as follows: HBV-DNA turned negative in 2 patients without nucleic acid analog (NAA) and 1 with NAA; 2 died due to bacterial sepsis; and 1 died due to autoimmune hemolytic anemia. Significant elevation of aminotransferase was found in only 1 patient, but HBsAg converted to positive in 2 patients and HBeAg converted to positive in 1 patient.
Conclusion. Reactivation of resolved HBV can occur during standard immunosuppressive therapy for autoimmune diseases. The low titer of baseline anti-HBs may carry its risk.
Reactivation of hepatitis B virus (HBV) in patients undergoing cytotoxic chemotherapy or immunosuppressive therapy is considered one of the most important complications of such treatments affecting prognosis1,2,3,4,5. Prophylactic administration of nucleic acid analog (NAA) is recommended for HBV carriers during moderate or high intensity immunosuppressive therapies6,7,8.
Clearance of hepatitis B surface antigen (HBsAg) with the appearance of antibody against HBsAg (anti-HBs) had been generally accepted as evidence of clinical cure of acute hepatitis B. However, in 2001 Dervite, et al first reported a possible relationship between HBV reactivation and use of rituximab in a patient with anti-HBs9. In 2006, a prospective study from Hong Kong revealed that 3.3% of patients who were HBsAg-negative developed HBV reactivation after chemotherapy10. HBV replication persists at low levels in the liver for decades after acute hepatitis B11,12,13,14,15. Hepatitis with reactivation of resolved HBV has frequently been reported16,17,18,19,20,21,22. From these data, negative HBsAg with positive antibody against hepatitis B core antigen (anti-HBc) has been recently accepted as occult HBV infection. High mortality is of great clinical significance in reactivation of resolved HBV. An epidemiological study revealed that reactivation of resolved HBV was found in 23 (4%) of 552 patients who were newly HBsAg-positive; fulminant hepatic failure developed in 5 (22%) of these 23 cases with 100% mortality, and all 5 patients had received a treatment regimen with rituximab23.
Most of these reports have come from the fields of oncology and transplantation. There has been little evidence regarding reactivation of resolved HBV in the autoimmune diseases24, including a few case reports of reactivation of resolved HBV during treatments with anti-tumor necrosis factor (TNF) or methotrexate (MTX)25,26,27 and one prospective study suggesting the risk of reactivation of resolved HBV during biologic treatments28. We investigated the risk of HBV reactivation during diverse immunosuppressive therapies for autoimmune diseases in patients who were HBsAg-negative.
MATERIALS AND METHODS
Study design and patients
A total of 414 patients with active autoimmune diseases who would have immunosuppressive therapy were screened for HBsAg, anti-HBc, and anti-HBs (all by the enzyme immunoassay method) in our institution during the period July 2007 through March 2010. A total of 35 HBsAg-negative and anti-HBc-positive patients were identified (Table 1). These 35 patients were followed for 24 (range 8–124) weeks and their clinical outcomes were analyzed including serum levels of HBV-DNA (by polymerase chain reaction method), aspartate aminotransferase (AST), and alanine aminotransferase (ALT) every 4 weeks during the immunosuppressive therapy for underlying autoimmune diseases. HBV-DNA was detected during the immunosuppressive therapy; HBsAg, anti-HBs, hepatitis B e antigen (HBeAg), and antibody against HBeAg (anti-HBe) were also monitored every 4 weeks (all by the enzyme immunoassay method). AST/ALT elevation was considered significant if elevated more than 3 times the upper limit of normal.
Patients’ characteristics (N = 35).
Our study was performed in accord with the Declaration of Helsinki and the Principles of Good Clinical Practice. Approval was obtained from the local ethics committee.
Statistical analysis
Statistical analysis was performed by Student’s t test, Mann-Whitney U test, chi-square test, or Fisher’s exact test, as appropriate. P values < 0.05 were considered significant.
RESULTS
Risk analysis of HBV-DNA detection (HBV reactivation)
Out of 414 patients screened in this study, 35 patients (8%) had negative HBsAg and positive anti-HBc. HBV-DNA was detected in 6 of these 35 patients during the immunosuppressive therapy. HBV-DNA turned positive between 4 and 8 weeks after the initiation of immunosuppressive therapy. There were no differences in sex, age, dose of prednisolone, and level of total serum immunoglobulin G between the patients in whom HBV-DNA was detected and the others (Table 2). Type of therapy, such as steroid pulse therapy, immunosuppressants, or biologics, did not correlate with the HBV reactivation. Baseline anti-HBs titer was significantly lower in the patients in whom HBV-DNA was detected compared with the other patients [2.83 (range 0.24–168.50) mIU/ml vs 99.94 (range 0.00–5342.98) mIU/ml, respectively; p = 0.036 by Mann-Whitney U test; Table 2].
Comparison of patients in whom HBV-DNA was detected (HBV reactivation) or not detected.
Outcomes of patients with HBV reactivation
Outcomes of the 6 patients with HBV reactivation were as follows: HBV-DNA turned negative in 2 patients without NAA and one with NAA; 2 died due to bacterial sepsis; and 1 died due to autoimmune hemolytic anemia (Table 3). Significant elevation of AST and/or ALT was found in only 1 patient, but HBsAg converted to positive in 2 patients and HBeAg converted to positive in 1 patient (Table 3). The mortality rate was slightly higher in patients with HBV reactivation than in those without: 50% (3/6) versus 17% (5/29), respectively (p = 0.10, Fisher’s exact test). Three representative clinical courses of patients with HBV reactivation are shown in Figure 1; a 77-year-old woman recovered with NAA (Figure 1A), a 78-year-old woman spontaneously recovered without NAA (Figure 1B), and a 58-year-old woman developed reverse seroconversions of both HBs and HBe (Figure 1C).

Representative clinical courses of patients with HBV reactivation. A. A 77-year-old woman treated with NAA. B. A 78-year-old woman who spontaneously recovered without NAA. C. A 58-year-old woman who developed reverse seroconversion of both HBs and HBe. PSL: prednisolone; LVD: lamivudine; ETV: entecavir; AST: aspartate aminotransferase; ALT: alanine aminotransferase.
Outcomes of patients with HBV reactivation.
Anti-HBs titer
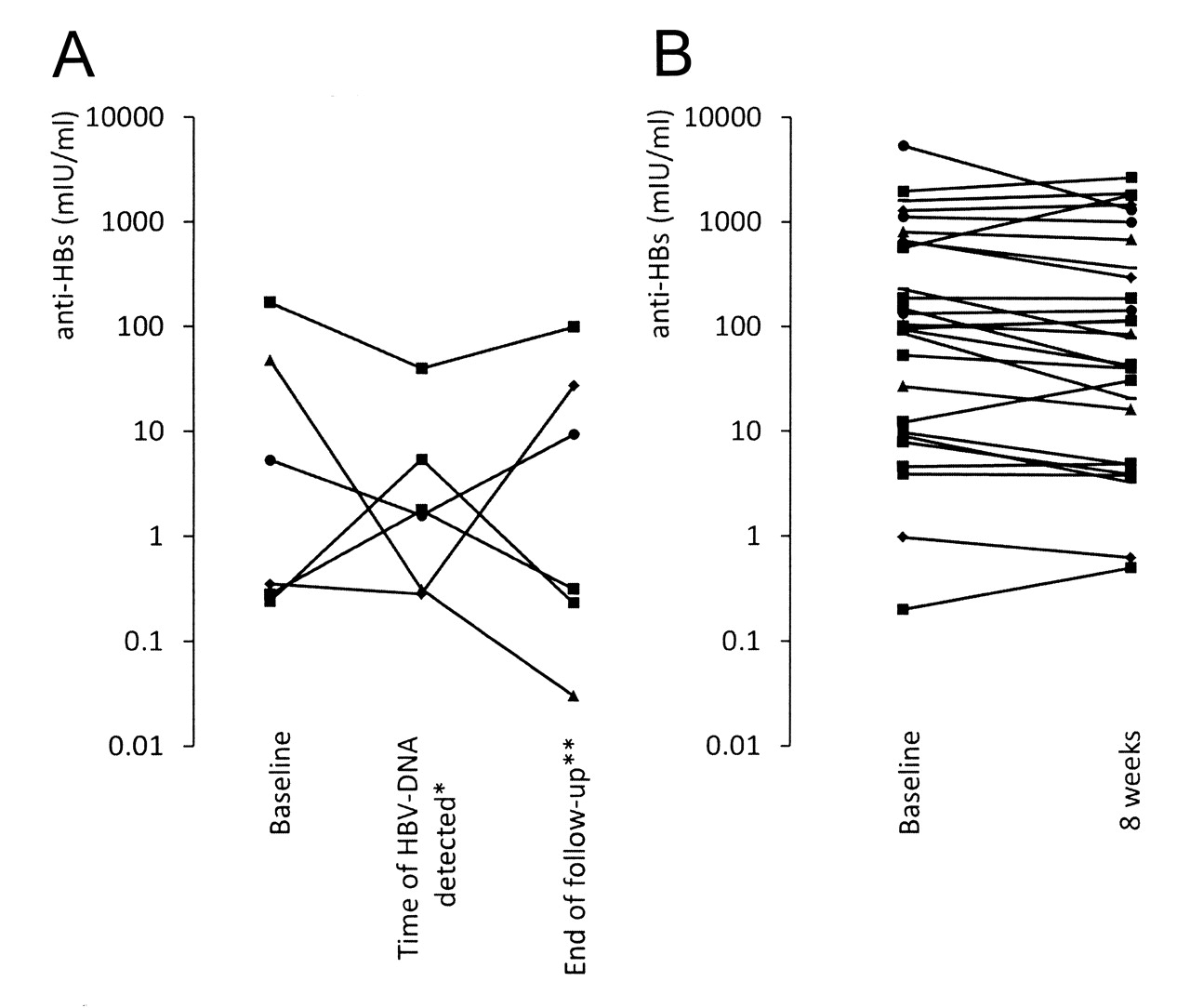
The titer of anti-HBs was monitored in each patient with HBV reactivation at baseline, at the time HBV-DNA was detected, and at the end of followup, but no particular fluctuation pattern was noted (Figure 2A). In patients without HBV reactivation, anti-HBs was measured at baseline and 8 weeks after the initiation of immunosuppressive therapy, showing persistent titers of anti-HBs: 99.4 (range 0.00–5342.98) mIU/ml versus 77.4 (range 0.00–2652.80) mIU/ml (p = 0.66, Mann-Whitney U test; Figure 2B).
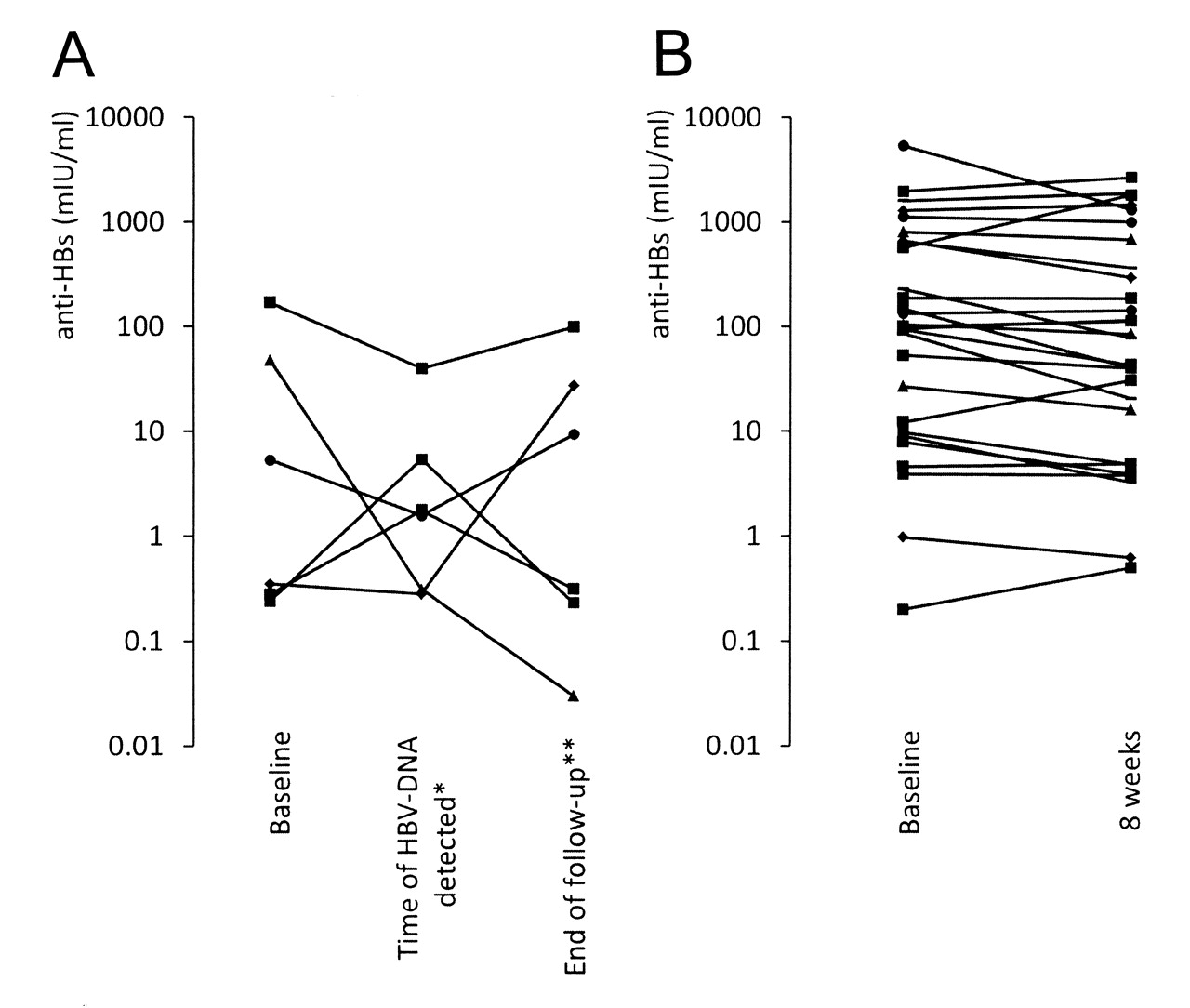
Change of anti-HBs titer in patients with HBV reactivation (A) and in those without reactivation (B). *4 to 8 weeks; **20 to 124 weeks.
DISCUSSION
We demonstrate the potential risk of HBV reactivation during standard immunosuppressive therapy for autoimmune diseases in patients who are HBsAg-negative. There have been 3 case reports of reactivation of resolved HBV during treatments with anti-TNF or MTX: a patient with Crohn’s disease receiving infliximab25, a patient with ankylosing spondylitis receiving etanercept26, and a patient with rheumatoid arthritis receiving low doses of MTX27. In prospective studies, there have been conflicting results regarding the risk of reactivation of resolved HBV by biological agents; Charpin, et al reported the safety of anti-TNF agents in 21 patients with rheumatic diseases29, and Vassilopoulos, et al reported the safety of anti-TNF agents in 19 patients with rheumatic diseases30. In contrast with these small prospective studies, Urata, et al reported that reactivation of resolved HBV occurred in 7 of 135 patients with rheumatoid arthritis and that use of biologic agents represented a risk for reactivation28. Therefore, the safety of immunosuppressive therapy in patients with resolved HBV with autoimmune diseases has not been established.
From our data, anti-HBs, the neutralizing antibody against HBV, may correlate with HBV reactivation. Anti-HBs titer was significantly lower in the patients with HBV reactivation than the others at baseline and tended to rise upon detection of HBV-DNA in some cases (Figure 1). Onozawa, et al31 reported a correlation between progressive decrease of anti-HBs and reactivation of resolved HBV after allogeneic hematopoietic stem cell transplantation. In our study, a progressive decrease of anti-HBs was not seen. Compared with reports of treatments in the field of oncology or transplantation, the current therapy for autoimmune diseases is less aggressive in terms of immunosuppression, thus anti-HBs titers are persistent in patients with autoimmune diseases. In contrast, the low titer of anti-HBs at baseline may represent the risk of HBV reactivation and could be one of the markers for the management of those patients.
All the subjects investigated in our study had active heterogeneous autoimmune diseases requiring aggressive immunosuppressive therapy, thus it was difficult to analyze a correlation between underlying disease activity and HBV reactivation. However, patients receiving cyclophosphamide had relatively higher risk of having HBV reactivation than the other patients [31% (4/13) vs 9% (2/22); p = 0.12, Fisher’s exact test]. It could reflect that patients who received cyclophosphamide because of high disease activity had more risk of HBV reactivation.
The limitations of our study are the small sample size, large confidence intervals, and relatively short followup. In the published reports, reactivation of resolved HBV occurred 1 to 14 months after the initiation of immunosuppressive therapy25,26,28, thus longer observation in large population studies may confirm our findings.
Our study suggests that reactivation of resolved HBV can occur during standard immunosuppressive therapy for autoimmune diseases, and that the low titer of baseline anti-HBs may carry its risk. Further study will be needed to establish the procedure for better management of HBV reactivation in the field of autoimmune diseases.
- Accepted for publication June 10, 2011.








{kind=link}
{kind=link}