

Abstract
Objective. To evaluate the clinical benefits of the endothelin receptor antagonist bosentan on interstitial lung disease (ILD) in patients with systemic sclerosis (SSc) who are ineligible for cyclophosphamide (CYC) therapy.
Methods. In this prospective open-label study, 9 patients with SSc and ILD received bosentan for 24 months. The main reasons for avoiding CYC included severely impaired lung function, long disease duration, and relapse after CYC treatment. Pulmonary function tests and Doppler echocardiograms were evaluated every 6 months, and high-resolution computed tomography (HRCT) was performed every 12 months. For an extended survival analysis, 17 historical controls who met the inclusion criteria at referral and had not used any immunosuppressive or antifibrotic agents thereafter were selected from the SSc database.
Results. Two patients did not finish the study; one developed vasculitis requiring high-dose corticosteroids and another died of bacterial pneumonia. The remaining 7 patients tolerated bosentan and completed the study period. There were trends toward mildly reduced forced vital capacity, total lung capacity, and diffusing capacity for carbon monoxide over time. Two patients developed pulmonary hypertension during the 24-month period. HRCT scores for ground-glass opacity, pulmonary fibrosis, and honeycomb cysts gradually increased. In the extended study, there was no difference in cumulative survival rate between the bosentan-treated and historical control groups.
Conclusion. The gradual worsening of pulmonary function and HRCT findings in patients treated with bosentan was consistent with the natural course of SSc-associated ILD. This study does not support the use of bosentan for SSc-associated ILD even when CYC treatment is inadvisable.
Interstitial lung disease (ILD) is the leading cause of disease-related morbidity and mortality in patients with systemic sclerosis (SSc)1. University of Pittsburgh database records of SSc-related deaths over the past 30 years show that the proportion of patients who died of ILD increased from 6% to 33%, indicating that ILD is the primary cause of SSc-related deaths today2. The current treatment for SSc-associated ILD (SSc-ILD) is limited to immunosuppressive agents. For patients with endstage ILD, lung transplantation may offer a viable alternative therapeutic option. A recent randomized placebo-controlled trial (Scleroderma Lung Study; SLS) reported a modest but significant benefit of oral cyclophosphamide (CYC) on lung function and health-related quality of life in SSc patients with active ILD3, but this small effect was lost at 1 year of followup4. Two independent metaanalyses failed to demonstrate any clinically significant improvement in pulmonary function in patients with SSc who were treated with CYC5,6. In the Markov decision analytic model for evaluating risk-benefit tradeoffs, 1 year of CYC therapy for SSc-ILD actually resulted in a small loss in the quality-adjusted life-years compared with no CYC7. On the other hand, it has been reported that a clinical response to CYC is observed only in a subset of patients with ILD, with the predictors of clinical benefit including a forced vital capacity (FVC) < 70% and moderate pulmonary fibrosis on high-resolution computed tomography (HRCT)8. Therefore, the use of CYC should be decided on a patient-by-patient basis by considering the balance between therapeutic efficacy and potential toxicities, such as carcinogenesis and impaired fertility. Alternative regimens for treating SSc-ILD are clearly needed, especially in patients with advanced or endstage ILD, significant risk for toxicity, or relapse after CYC treatment.
Endothelin-1 (ET-1), an endogenous vasoconstrictor, is implicated in the pathophysiology of pulmonary arterial hypertension (PAH) through the constriction and proliferation of vascular smooth muscle cells9. Endothelin receptor antagonists (ERA) such as bosentan have been shown to be effective treatments for PAH10,11. ET-1 also exerts profibrotic activity by modulating matrix turnover12 and interacting with transforming growth factor-ß signaling13. In addition, ET-1 has been shown to play an important role in ILD pathogenesis, based on the elevated ET-1 levels in the plasma and bronchoalveolar lavage fluids of patients with ILD14, and reduced collagen deposition in the lung with ERA treatment in a rat model for bleomycin-induced pulmonary fibrosis15. Due to its antifibrotic effects, ET-1 blockade would seem to be a logical approach to treating ILD, and randomized, placebo-controlled trials were conducted to investigate the potential efficacy of the dual ERA bosentan on idiopathic pulmonary fibrosis (BUILD-1)16 and SSc-ILD (BUILD-2)17. Disappointingly, both trials failed to show improvement in the 6-min walk distance and in lung function in patients treated with bosentan, although there was a trend in favor of bosentan delaying the time to death or disease progression in patients with biopsy-proven usual interstitial pneumonia16. Since the BUILD-2 trial used strict criteria to select SSc patients with active and progressive ILD but without clinically apparent pulmonary hypertension (PH)17, it is still possible that bosentan is effective for certain subsets of SSc-ILD, such as endstage ILD with severely impaired pulmonary function and complicating PH.
We conducted a 24-month open-label study to evaluate the clinical benefits of bosentan in patients with SSc-ILD ineligible for CYC treatment. The majority of patients enrolled did not satisfy the inclusion criteria of the BUILD-2 trial.
MATERIALS AND METHODS
Study design
This open-label prospective study was conducted at Keio University Hospital, Tokyo, Japan. The protocol was initiated in February 2006, and all the enrolled patients completed the study by February 2010. After assessing a patient’s suitability for the study, bosentan was initiated at 62.5 mg twice daily. The dosage was increased to 125 mg twice daily at 4 weeks, and continued for 24 months. Patients were allowed other medications, with the exception of corticosteroids at a dose > 10 mg/day of prednisone or equivalent, or immunosuppressive agents. After completing the 24-month study period, patients were allowed to continue bosentan and were followed to assess the longterm survival and safety profiles. A complete medical history, physical examination, and laboratory analysis were performed for each patient at pretreatment, with more limited evaluations during monthly followup visits. Pulmonary function tests (PFT) and transthoracic echocardiography were done at the 0 (pretreatment), 6, 12, 18, and 24-month visits, and HRCT was performed at 0, 12, and 24 months. Safety profiles, including liver toxicity, were monitored at monthly intervals. The study protocol conformed to the ethical guidelines of the Declaration of Helsinki, as reflected in prior approval from the institutional review boards, and each patient gave informed written consent.
Subjects
Patients were considered for inclusion if they satisfied all the following criteria: they (1) were over 18 years of age; (2) met the American College of Rheumatology preliminary classification criteria for SSc18; (3) had both exertional dyspnea and ILD as determined by chest radiographs; and (4) were considered ineligible for CYC treatment because of severely impaired lung function [defined as having FVC < 45%, diffusing capacity for carbon monoxide (DLCO) < 30%, oxygen saturation measured by pulse oximetry < 85% during exercise], SSc duration > 7 years after the first non-Raynaud’s phenomenon, a relapse after CYC treatment, a recent malignancy, or the patient’s refusal3. Patients currently treated with corticosteroids > 10 mg/day prednisone or equivalent and/or immunosuppressive agents were excluded. For the extended survival analysis, we selected 17 historical controls from our SSc database, which contains information on 415 patients diagnosed since 1985, based on the following criteria: they (1) met the inclusion and exclusion criteria of this study at time of referral (first visit) to our hospital; and (2) had never been treated with immunosuppressive agents, corticosteroids > 10 mg/day (prednisone), or D-penicillamine since referral to our hospital. Patients with SSc were classified as having diffuse or limited cutaneous disease19. Diffuse cutaneous SSc (dcSSc) was considered present if, at any time during the course, skin thickening proximal to the elbows or knees was present, e.g., upper arms, thighs, anterior chest, or abdomen.
Outcome measures
PFT were performed to evaluate FVC, total lung capacity (TLC), and DLCO. Clinically significant worsening and improvement of PFT scores were defined as described17. Echocardiography using the Doppler technique was used to evaluate the degree of PH. The tricuspid regurgitation pressure gradient (TRPG) estimated by the tricuspid regurgitation peak velocity was recorded, with tricuspid regurgitation peak velocity > 3.4 m/s or TRPG > 46 mm Hg indicating the presence of PH20. The degree of ILD was semiquantitatively assessed by the HRCT scoring system proposed by Goldin, et al21. Scores (scale 0–24) for ground-glass opacity, pulmonary fibrosis, and honeycomb cysts were recorded individually. The ILD stage, extensive or limited disease, was determined according to the combined evaluation of PFT and HRCT22. The modified Rodnan skin thickness score (MRSS; scale 0–51), oral aperture, fingertip-to-palm distance (FTP), Raynaud’s condition score (scale 0–10)23, number of digital ulcers, and the Scleroderma Health Assessment Questionnaire (SHAQ) including the disability index (DI; scale 0–3) and visual analog scale (VAS; scale 0–3)24,25 were also used to evaluate skin thickening, peripheral vascular disease, and functional status.
Identification of SSc-related antinuclear antibodies (ANA)
Serum samples obtained from patients entering the study were analyzed for SSc-related ANA using indirect immunofluorescence and immunoprecipitation assays26.
Statistical analysis
All continuous values were shown as the mean ± SD, and were compared using the Mann-Whitney U test. The frequencies between 2 groups were tested for statistical significance using the chi-square test or Fisher’s 2-tailed exact test, when applicable. Changes in values at different timepoints from the baseline were compared by repeated measures analysis of variance. Cumulative survival rates were calculated according to the Kaplan-Meier method, and comparisons were made using the Cox-Mantel log-rank test.
RESULTS
Patient characteristics at baseline
Nine patients, with the baseline characteristics shown in Table 1, were enrolled. The ratio of men to women was 4:5, and age at entry ranged from 29 to 79 years (55 ± 19). Five were classified as having dcSSc. Evaluation of ANA profiles revealed that all patients with dcSSc were positive for antitopoisomerase I antibodies, and patients with limited cutaneous SSc had either anti-Th/To or anti-U1RNP antibodies. Based on the ILD staging system proposed by Goh, et al22, all except 1 patient had extensive disease, and 4 patients were already receiving supplemental oxygen. Disease duration from the first non-Raynaud’s symptom ranged from 10 to 338 months (141 ± 134). Patient 5 showed elevated TRPG (53 mmHg), suggesting the coexistence of PH. CYC was not used due to severely impaired lung function in 4 patients, long disease duration in 2, relapse after CYC treatment in 1, the patient’s refusal in 1, and recent malignancy in 1.
Baseline characteristics of the 9 patients with SSc enrolled.
Safety profiles
During the 24-month study, none of the patients experienced elevated aminotransferase levels (> 3-fold the upper limit of normal) or other adverse events potentially associated with bosentan. Two patients were dropped from the study; 1 because of antineutrophil cytoplasmic antibody-associated vasculitis requiring high-dose corticosteroid therapy at 7 months (Patient 3) and another died of bacterial pneumonia at 17 months (Patient 6). The remaining 7 patients tolerated bosentan and completed the entire study period.
Serial evaluations of outcome measures
Serial measurements of FVC, TLC, DLCO, and TRPG in the 9 patients enrolled are shown in Figure 1. In the 7 patients who completed the 24-month study period, there were trends toward mildly reduced FVC (62.1% ± 24.0% at baseline to 58.7% ± 22.8% at 24 months), %TLC (61.4% ± 12.4% at baseline to 56.0% ± 10.9% at 24 months), and %DLCO (33.4% ± 13.0% at baseline to 27.6% ± 16.4% at 24 months), but only the reduction of TLC was statistically significant (p = 0.04). The PFT scores remained stable for all but 1 patient (Patient 9), who experienced clinically significant worsening at 12 and 24 months. None of the patients showed improved PFT scores. TRPG changes were not statistically significant (34.9 ± 9.0 at baseline to 35.4 ± 18.2 at 24 months), but in 2 patients who experienced increased TRPG (Patients 2 and 5), PH was confirmed by right-heart catheterization.

Pulmonary function test results and tricuspid regurgitation pressure gradient (TRPG) changes in 9 patients with SSc-ILD during treatment with bosentan. Statistical analysis was performed for the 7 patients who completed the 24-month study period. *Results from dropout patients. FVC: forced vital capacity; TLC: total lung capacity; DLCO: diffusing capacity for carbon monoxide; NS: not significant.
Serial HRCT evaluations revealed stable but slightly increased scores for ground-glass opacity and pulmonary fibrosis (Table 2). The scores for honeycomb cysts gradually increased, and had doubled at 24 months compared with the pretreatment scores (p = 0.02). As shown in Table 2, the MRSS and oral aperture were stable, but flexion contractures of the digits as measured by FTP appeared to worsen during the study period. The Raynaud’s condition scores tended to increase, but 3 patients experienced a decrease in the number of digital ulcers at 12 and 24 months compared to those observed at pretreatment. There was no treatment effect for the SHAQ-DI or VAS during the study period.
Serial measurements of high resolution computed tomography (HRCT) scores, and measurements of skin thickening, peripheral vascular disease, and functional status in 7 patients who completed the entire study period. Results are shown as the mean ± SD.
Extended survival analysis
Seven patients continued to take bosentan for an additional 2–24 months after the 24-month study period. None of the patients stopped bosentan due to a potential adverse event during the extension period. Sildenafil was added in 2 patients with PH; one of these died of respiratory failure at 27 months. Therefore, 2 patients (22%) died of ILD-related causes (respiratory tract infection at 17 months and respiratory failure at 27 months) while taking bosentan. The cumulative survival rate in patients treated with bosentan at 2 and 3 years was 86% and 71%, respectively (Figure 2).
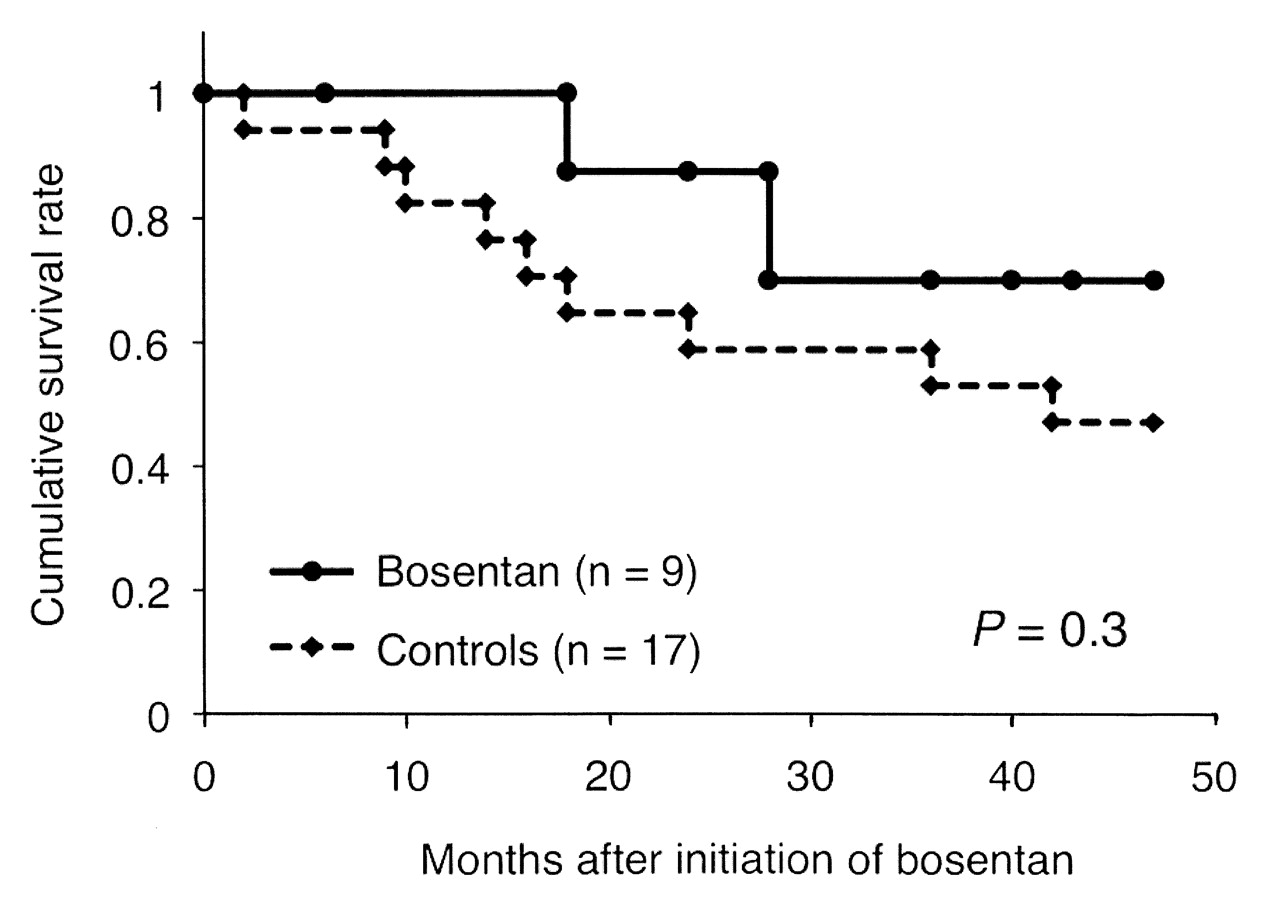
Cumulative survival rates in 9 patients treated with bosentan and 17 historical controls. Comparison between the 2 groups by Cox-Mantel log-rank test.
We further compared the cumulative survival rate in bosentan-treated patients and historical controls. Table 3 shows baseline characteristics in the 9 bosentan-treated patients and 17 historical controls. There was no statistically significant difference in age at entry, disease duration, or lung function such as FVC and DLCO, but historical controls appeared to be more homogeneous than bosentan-treated patients: historical controls had shorter disease duration, lower %FVC, and higher prevalence of antitopoisomerase I antibody. When an outlier (Patient 9) with very long disease duration (338 months) and preserved %FVC (107%) was excluded from the bosentan-treated groups, disease duration and %FVC were 117 ± 134 and 52.0 ± 17.4, respectively, which were compatible to those in the historical controls. The reasons we did not treat ILD in 17 historical controls included severely impaired lung function in 11, long disease duration in 3, relapse after CYC treatment in 2, and recent malignancy in 1. Nine (53%) of the historical controls died within 48 months, and causes of death were all ILD-related, such as respiratory failure and respiratory tract infection. Although there was a trend toward better cumulative survival rates in the patients treated with bosentan, the difference did not reach statistical significance (p = 0.3). When an outlier (Patient 9) was excluded from the bosentan-treated group, cumulative survival rates at 3 years were almost concordant between bosentan-treated and control groups (67% vs 58%, respectively; p = 0.6).
Baseline characteristics of bosentan-treated patients and historical controls.
DISCUSSION
Since the BUILD-2 trial had shown that bosentan does not reduce the frequency of clinically important worsening in SSc patients with active and progressive ILD17, this prospective open-label study targeted the treatment of CYC-ineligible SSc-ILD. We found that 2-year treatment with bosentan did not have any beneficial effects on lung function or HRCT findings in the target population. Although bosentan was safe and well tolerated, all the outcome variables related to the extent and degree of ILD tended to worsen in spite of bosentan treatment. The relatively slow rate of progression in lung function changes and the HRCT findings in patients treated with bosentan were similar to the natural course of SSc-ILD27. Therefore, our data together with the BUILD-2 trial results do not support the use of bosentan as therapy for any forms of established ILD in patients with SSc, including the early disease with exertional dyspnea (SSc duration < 3 years), late active disease (SSc duration ≥ 3 years), or advanced or endstage disease.
The majority of the patients enrolled in our study had extensive disease, above 20% on HRCT, and the predicted 4-year survival rate of this population was < 60%22. In addition, severely impaired lung function requiring oxygen supplementation, ILD concomitant with PH, and relapse after CYC treatment, which were observed in the majority of our patients, are associated with poor prognosis28,29,30. Our data showed clearly that bosentan did not improve lung function, but it is still possible that bosentan slowed the lung function deterioration in a patient population highly likely to have poor prognosis. Unfortunately, this issue cannot be evaluated in the setting of a 24-month noncomparative study involving a small number of patients. Our life-table analysis suggests that bosentan may prolong survival in comparison with historical controls, but we have to consider that historical controls might have developed a greater amount of lung deterioration in a shorter period of time in comparison with bosentan-treated patients because of shorter disease duration and lower %FVC. Moreover, historical controls included patients referred to our hospital before 2000, and this may contribute to poor survival rates in historical controls because of outdated equipment and supportive therapies. Larger randomized controlled trials are needed to draw a final conclusion on whether bosentan treatment has some degree of benefit in patients with advanced or endstage ILD.
The potential benefit of ERA to suppress or prevent PH is particularly relevant in patients with SSc-ILD, because these agents have been confirmed to benefit SSc patients with PAH11. In this regard, it has been reported that in spite of ERA use, patients with ILD-associated PH have a 5-fold greater risk of death than those with PAH29, disfavoring the efficacy of ERA in patients with PH owing to ILD. On the other hand, in the subanalysis of the BUILD-2 study assessing bosentan’s preventive effect on PH in patients with SSc-ILD, PH developed in 5 patients (5.8%) in the placebo group, but in only one (1.3%) in the bosentan group during a 1-year study period, although this difference did not reach statistical significance17. However, in our study, 2 patients (22%) developed PH while being treated with bosentan. Thus, bosentan’s efficacy for treating ILD-related PH is apparently inferior to its efficacy for treating PAH.
ET-1 is involved in many pathologic processes, including vasoconstriction, cell proliferation, and promotion of inflammation and fibrosis, and thus blocking ET-1 signaling may result in pleiotropic effects beyond vasodilation. These effects are expected to be beneficial in various aspects of SSc pathogenesis, making ERA attractive potential disease-modifying agents for SSc31. Two randomized, prospective, placebo-controlled studies (RAPIDS-1 and -2) have demonstrated that fewer digital ulcers develop in patients treated with bosentan than in those receiving a placebo, although ulcers did not appear to heal better with bosentan treatment32,33. Recent open-label studies have shown that bosentan is potentially effective for reducing skin thickening in patients with SSc34,35. In contrast, we did not observe any improvement in outcome measures associated with Raynaud’s phenomenon, skin thickening, or functional status during bosentan treatment. These negative findings were also reported in the BUILD-2 trial17. The lack of therapeutic responses to bosentan may argue against a critical role for ET-1 in SSc pathogenesis, but it is also possible that because of the established and advanced stages of disease in our patient population any effective timing of treatment (in terms of the reversibility of the pathogenic process) might already have passed.
Treatment with bosentan did not improve or stabilize lung function in SSc patients with advanced ILD. Currently, there is no evidence to recommend the use of endothelin receptor antagonists for treating SSc-ILD, even when the disease is ineligible for CYC treatment.
Footnotes
-
Dr. Kuwana receives a research grant for intractable diseases from the Japanese Ministry of Health, Labor and Welfare.
- Accepted for publication June 10, 2011.








{kind=link}
{kind=link}