

Abstract
Objective. Adjusted mean Systemic Lupus Erythematosus Disease Activity Index (SLEDAI; AMS) measures lupus disease activity over time. Our aim was to determine optimal visit frequency for calculating AMS.
Methods. Patients followed monthly for 12 consecutive visits were included. AMS was calculated using all of the SLEDAI 2000 (AMSGOLD using all 12 visits), only quarterly visits (AMS3, using visits 3 months apart), semiannual visits (AMS6, using first, middle, and last visits only), and annual visits (AMS12, using only the first and last visits). Comparisons of AMS3, AMS6, and AMS12 with AMSGOLD are made using descriptive statistics.
Results. Seventy-eight patients were included (92% women, mean age at SLE diagnosis 30.1 yrs and at study start 46.2 yrs). The mean (SD) AMSGOLD for the entire year was 2.05 (1.66), for AMS3 1.99 (1.65), for AMS6 2.12 (1.87), and for AMS12 2.08 (1.83). Mean (SD) of the absolute differences with AMSGOLD: for AMS3 0.29 (0.33), for AMS6 0.45 (0.59), and for AMS12 0.61 (0.58). Differences that were < 0.5 were considered minimal while those ≥ 1 were deemed important. Comparing AMSGOLD to AMS3, 82% of the differences were minimal and 3% were important. When comparing to AMS6, 68% were minimal and 10% were important, while comparing to AMS12, 50% were minimal and 21% were important.
Conclusion. Usual clinic visits occurring quarterly offer a good estimation of disease activity over a 1-year period and are preferred over semiannual and annual visits.
Systemic lupus erythematosus (SLE) is an autoimmune disease of unknown cause. It affects primarily women in their childbearing years and has a variable course and prognosis. The disease may affect any organ system in the body, and because of the protean manifestations it has been difficult to assess disease activity. Several instruments to measure disease activity have been developed. Among the most commonly used are the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI), first developed in 19851, and last modified in 2000 (SLEDAI-2K)2; the British Isles Lupus Activity Group (BILAG), first developed in 19883 and last modified in 20044; and the Systemic Lupus Activity Measure (SLAM)5 and its modification SLAM-R6. These measures have been proven comparable in individual visits, and have demonstrated sensitivity to change over time.
SLEDAI has been validated as a tool to assess disease activity in SLE. It has demonstrated reproducibility when both experienced lupologists and novices assess patients7,8. It has also shown sensitivity to change9. High SLEDAI scores predict outcomes in SLE including death and damage accumulation. SLEDAI-2K is identical to the original SLEDAI expect for the definition of 4 items: alopecia, mucous membrane ulcers, rash, and proteinuria, which are recorded if there is persistent inflammation, while in the original SLEDAI would be recorded only if they were new. Its validity has been shown against the original SLEDAI2. While the SLEDAI was initially developed to measure disease activity in the preceding 10 days, it has now been shown to be valid to measure disease activity in the preceding 30 days10.
SLEDAI-2K assesses disease activity at a particular visit. To describe disease activity over time, the adjusted mean SLEDAI-2K (AMS) was developed. The AMS calculates the area under the curve of SLEDAI-2K divided by the length of the time interval11. The AMS has been shown to reflect burden of disease and is an important prognostic marker12.
In drug trials, patients are usually followed at monthly intervals. Consecutive monthly assessments measure the entire disease activity in the time interval. However, in clinical practice and longitudinal observational cohort studies, patients are seen at 3-monthly intervals, and at times miss their appointments and are then followed at irregular intervals. It is therefore important to know whether the assessment of disease activity over time as measured by the AMS can be applied to patients followed at intermittent intervals. Our aims were (1) to compare AMS obtained over a 1-year period when visits are done monthly to AMS obtained using quarterly, semiannual, or annual visits; and (2) to determine the optimal frequency of visits to measure disease activity. Both aims are assessed in individual patients and in patient cohorts.
MATERIALS AND METHODS
Patient selection
Patients registered at the University of Toronto Lupus Clinic who were seen monthly by the same experienced physician for a 12-month period were included. Clinical and laboratory information was collected according to a standard protocol, which includes a detailed clinical history, physical examination, and laboratory evaluation.
Assessment of disease activity
The SLEDAI-2K was calculated at each monthly visit. Several calculations of the AMS were performed. AMSGOLD was considered the “gold standard” for our study and was based on the AMS calculated using all of the monthly visits. AMS3 was defined as the AMS calculated using visits that are 3 months apart (quarterly visits). AMS6 was defined based on the AMS calculated using visits that are 6 months apart (semiannual visits). AMS12 was defined as the AMS calculated using the first and last visits (annual visits). Flare was defined as an increase in SLEDAI-2K of 4 or more between 2 consecutive monthly visits2.
Statistical analysis
Descriptive statistics included t tests and plots to represent distribution of AMSGOLD, AMS3, AMS6, and AMS12 in the group as a whole and in individual patients.
The difference in estimating AMS was calculated based on the absolute difference between AMSGOLD and AMS3, AMS6, and AMS12. This is called the “error” associated with visit frequency.
Presence of flare was determined in each patient using monthly visits. AMSGOLD was compared among patients with and without flares. The magnitude of this difference was labeled an “important error.”
RESULTS
Patient characteristics
Seventy-eight patients with SLE were seen monthly for 12 consecutive visits. Seventy-two (92%) were women and 6 (8%) were men, with a mean (± SD) age at SLE diagnosis of 30.7 ± 11.4 years; mean age at start of study of 46.2 ± 12.0 years; and mean disease duration of 15.5 ± 9.7 years. The mean SLEDAI-2K at each of the monthly visits is provided in Table 1. In total, 25 (32%) of the patients had at least 1 visit with a SLEDAI-2K score > 4.
Mean Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) at each of the monthly visits.
Assessment of disease activity
Table 2 and Figure 1 depict the distribution of AMS using monthly, quarterly, semiannual, and annual visits for the whole group. For the whole group there is no statistically significant difference in the estimation of AMS regardless of the time interval used for its calculation. For the group as a whole, mean AMS obtained through quarterly, semiannual, or annual visits all perform quite well, all within 0.07 from mean AMSGOLD.

Distribution of adjusted mean Systemic Lupus Erythematosus Disease Activity Index using monthly, quarterly, semiannual, and annual visits, for the whole group.
Distribution of adjusted mean Systemic Lupus Erythematosus Disease Activity Index (AMS) using monthly, quarterly, semiannual, and annual visits for the whole group.
Determination of error
Table 3 provides the distribution of errors between AMSGOLD and AMS3, AMS6, and AMS12 for individual patients, and indicates a dose-response relationship. The more frequent the visits, the better the estimate of the AMSGOLD. Figure 2 provides the distribution per patient in addition to the magnitude of the error.
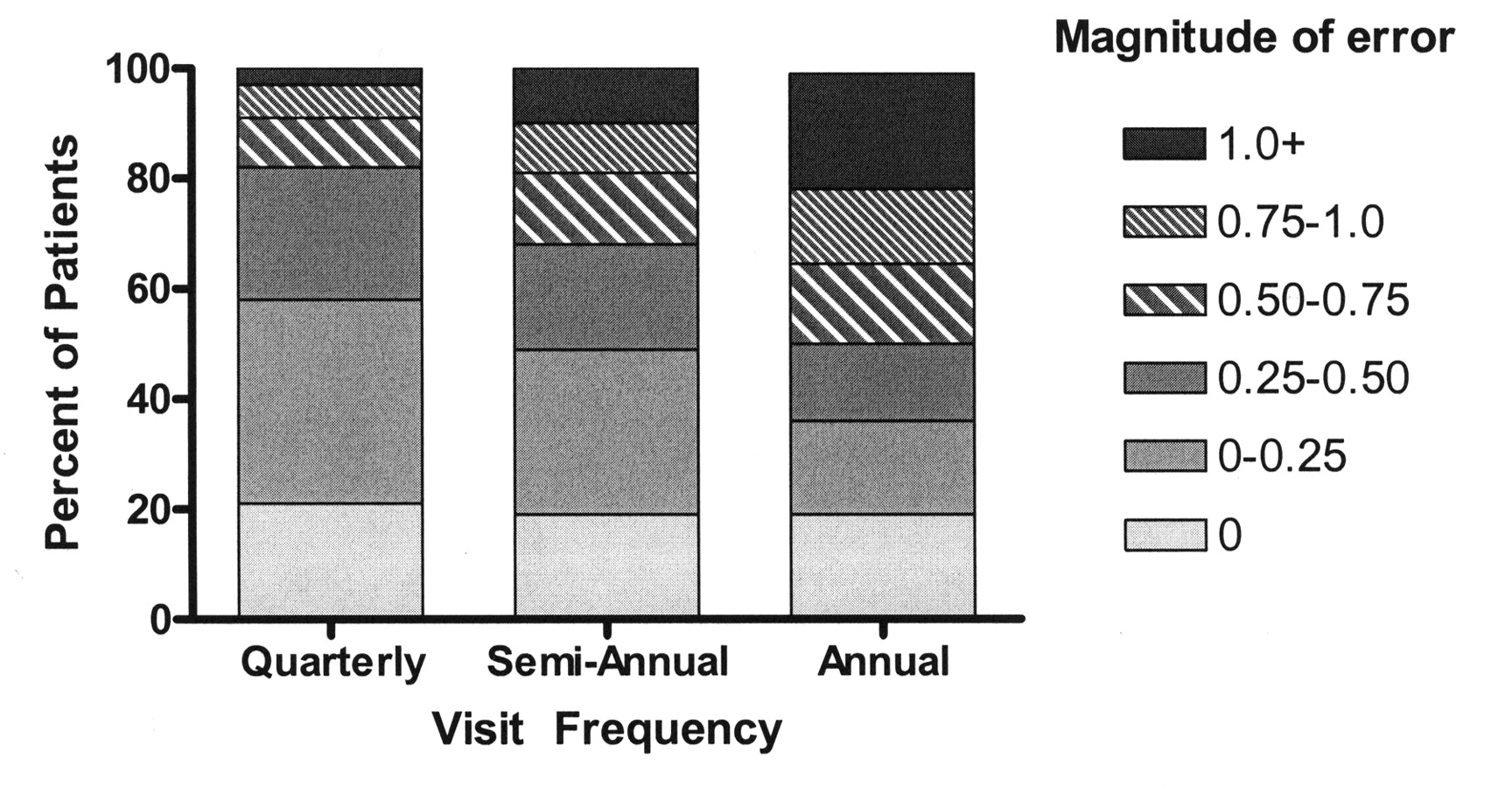
Distribution of errors by visit frequency.
Distribution of errors between AMSGOLD and AMS3, AMS6, and AMS12 for individual patients.
Determination of important error
Based on the SLEDAI-2K definition of flare of an increase of 4 or more, and using the monthly visits, 25 patients had at least 1 flare during the study period, while 53 patients did not have a flare. A comparison of AMSGOLD among patients with flares (2.74 ± 1.44) or without flare (1.72 ± 1.67) revealed a statistically significant difference of magnitude 1.0 (p = 0.01). Based on this difference, an important error was defined as a difference of 1. Evaluating the percentage of patients with an important error when using the different visit frequencies, we see that for AMS3 it occurred in 3% of patients, for AMS6 in 10%, and for AMS12, 21%.
DISCUSSION
The assessment of disease activity is important in evaluating patients with SLE. This is relevant in clinical practice and in longitudinal observational cohort studies, as well as in clinical trials of new medications. In randomized clinical trials, patients are typically assessed at monthly intervals. The American College of Rheumatology Ad Hoc Committee on SLE Guidelines for referral and management of SLE in adults recommended that the frequency of visits in patients with SLE be at least every 3 months13. However, in clinical practice and longitudinal observational cohort studies, patients often miss visits and may be seen semiannually or even annually instead.
We have previously described a method for calculating disease activity over time for patients seen on a regular basis11. The frequency of visits, however, may have an effect on the accurate determination of disease activity over time. Therefore, we sought to determine whether the frequency of visits would affect the accuracy of estimating the AMS in patients with SLE. We demonstrate that when groups of patients are analyzed, the frequency of visits within 1 year does not have a significant effect on the mean AMS. The difference between the AMSGOLD and the AMS3, AMS6, and AMS12 was within 0.07, a difference that is neither clinically nor statistically significant. Thus, when comparing groups of patients, yearly visits may suffice to describe disease activity over time.
At the patient level, there are errors in the estimation of AMS depending on the visit frequency. Indeed, there is an increasingly larger error with less frequent visits, such that when a patient is seen at 12-month intervals, the average error increases to 0.61 when compared to the monthly interval visits.
Patients who flared during the year of followup had an AMSGOLD with a magnitude of 1 greater than patients who did not flare. This is defined as an important error. Based on this definition, there was an increasing percentage of important error based on the frequency of visits, with low occurrence of ≤ 10% noted for visits of ≤ 6 months and 21% for yearly visits. Thus in therapeutic trials, when disease activity over time is used as an outcome, landmark analyses at the end of the trial, usually at 1 year, may not accurately describe total disease activity during the followup. This study shows that visits up to 3 months apart provide a good estimation of disease activity over time. Visits beyond 3 months compromise this measure.
A strength of our study is that all patients were evaluated by the same experienced physician, with data gathered in a uniform way and described with the same activity index.
The study patients selected were not different from the rest of the patients seen in the clinic in terms of sex, age at SLE diagnosis, or disease duration, but had a lower average SLEDAI-2K value [4.21 ± 4.54 for the clinic patients compared to 2.06 ± 2.19 for the study group (p < 0.0001)]. A potential weakness lies in the fact that overall, the disease activity in these patients was low, with only 25 patients with a SLEDAI-2K > 4. Whether the same results would be true for patients with higher SLEDAI-2K scores remains to be determined.
When assessing groups of patients, visit frequency of every 3, 6, or 12 months does not affect the mean AMS. In individual patients, usual clinical visits occurring quarterly offer a good estimation of disease activity over a 1-year period and are preferred over semiannual and annual visits.
- Accepted for publication September 21, 2010.








{kind=link}
{kind=link}