

Abstract
Objective. There are a number of different approaches to the initial treatment of juvenile dermatomyositis (JDM). We assessed the therapeutic approaches of North American pediatric rheumatologists to inform future studies of therapy in JDM.
Methods. A survey describing clinical cases of JDM was sent to pediatric rheumatologists. The cases described children with varying severity of typical disease, disease with atypical features, or refractory disease. Three open-ended questions were asked following each case: (1) What additional investigations would you order; (2) What medicine(s) would you start (dose, route, frequency, adjustment over time); and (3) What nonmedication treatment(s) would you start.
Results. The response rate was 84% (141/167). For typical cases of JDM, regardless of severity, almost all respondents used corticosteroids and another medication, methotrexate (MTX) being the most commonly used. The route and pattern of corticosteroid administration was variable. Intravenous immunoglobulin (IVIG) was used more frequently for more severe disease, for refractory disease, and for prominent cutaneous disease. Hydroxychloroquine was often used in milder cases and cases principally characterized by rash. Cyclophosphamide was reserved for ulcerative disease and JDM complicated by lung disease.
Conclusion. For the majority of North American pediatric rheumatologists, corticosteroids and MTX appear to be the standard of care for typical cases of JDM. There is variability, however, in the route of administration of corticosteroids and use of IVIG and hydroxychloroquine.
Juvenile dermatomyositis (JDM) is a rare chronic inflammatory disease of childhood affecting approximately 3.2 children per million per year1. The characteristic clinical features of proximal muscle weakness and rash are secondary to a systemic immune-mediated vasculopathy. The outlook for children with JDM has greatly improved compared to 50 years ago, when one-third of affected children died and another third had disabling complications of the disease2. The prognosis of JDM is now more favorable. Mortality is rare and less than 10% of children have significant disability in longterm followup3. Despite this, recent studies show that over half of patients have persistent disease activity and/or continued need for medications 3 years after initiation of therapy3,4,5.
There are no randomized controlled trials of therapy for JDM. Observational studies have suggested that the use of high-dose corticosteroids early in the disease course has improved prognosis. Outcome studies of children treated in the 1970s demonstrated that children who were treated with low-dose or short courses of corticosteroids, or had a delay in initiation of treatment, had poorer functional outcomes and more dystrophic calcium deposition6,7. These findings led to the adoption of treatment regimens using high-dose oral corticosteroids (up to 2 mg/kg/day prednisone) with a slow tapering regimen, often over a minimum of 2 years8,9,10,11. Concern about the side effects of prolonged corticosteroid use — in both uncomplicated and corticosteroid resistant/dependent cases — has led to a number of new treatment approaches. Early aggressive therapy with high-dose intravenous methylprednisolone (IVMP)12,13 and the early introduction of methotrexate (MTX)8 and/or intravenous immunoglobulin (IVIG)14,15,16 have often been used with the goal of controlling disease and minimizing treatment related toxicity. Additional immunosuppressive drugs have been used as adjunctive therapies in the treatment of JDM, including hydroxychloroquine17, cyclosporin A18,19, azathioprine6, mycophenolate mofetil20, systemic tacrolimus21, cyclophosphamide22, and rituximab23.
One goal for studying therapy in JDM is to better define efficacy and safety of current approaches. A proposed strategy is to develop specific well defined treatment protocols from which rheumatologists could choose when treating children. Carefully collected, standardized outcomes would allow for a comparison of competing combinations of therapies to assess efficacy and safety. In order to best define such treatment protocols, it is necessary to understand the current treatment approaches of pediatric rheumatologists treating JDM. We therefore undertook a survey that presented written clinical cases to participants. The primary aim of the study was to describe therapeutic approaches taken by North American pediatric rheumatologists. A secondary aim was to describe the investigative approach to these cases.
MATERIALS AND METHODS
The survey was administered using methods as described24. The study was approved by the Research Ethics Board at Hospital for Sick Children (Toronto, Canada). Members of the Childhood Arthritis and Rheumatology Research Alliance (CARRA) were asked to complete an on-line or paper survey in November 2006. CARRA members surveyed were board certified or board eligible pediatric rheumatologists (≥ 50% professional effort in pediatric rheumatology), pediatric rheumatology trainees (licensed physician participating in an approved Pediatric Rheumatology Fellowship program), or emeritus members (member no longer active in clinical research). At the time of this survey, 76 American and Canadian centers were represented. Survey participants were asked to provide practice details, including their subspecialty and number of new cases of JDM seen over a 5-year period.
A subgroup of investigators developed 11 clinical cases based on real cases from their practices. The themes of the cases were chosen to reflect a variety of presentations of JDM. Each written case consisted of structured components providing details on the clinical presentation, unique features differentiating each case from the others, results of investigations, and functional measures. A summary of the pertinent features from each case can be found in Table 1. Four of the cases represented varying degrees of severity of “typical” JDM, 5 represented “atypical” presentations, and 2 were cases of “refractory” disease. Three open-ended questions were posed following each case: (1) What additional investigations would you order? (2) What medicine(s) would you start (dose, route, frequency, adjustment over time)? and (3) What non-medication treatment(s) would you start? Subjects were not limited with respect to the number of responses they could provide.
Summary of the pertinent features of the clinical cases of JDM.
In the pilot phase of the survey, we determined that completion of all 11 cases was not feasible due to the duration of time required to complete the survey. Participants were therefore asked to complete 4 cases each. Each participant completed the case that represented a moderately severe case of “typical” JDM (the second case in Table 1) and the remainder of cases was randomly distributed prior to sending out the survey using a table of random numbers so that each participant completed 3 additional cases. Each participant was assigned to one of 4 groups of cases (Groups A-D), with each group comprising the moderately severe case and 3 other cases. Due to the number of cases, 2 of the 4 groups contained a repeat case (see Table 2).
Response rate by individual case.
Analysis
Survey responses were summarized using descriptive analysis. The survey was sent to all members of CARRA. Calculations for precision in a descriptive study are as follows: 18 usable questionnaires would give a 95% CI around a clear majority opinion (we defined it as 75%) of ± 0.2. Seventy-two usable questionnaires would give a 95% CI around 0.75 of ± 0.1. And 147 usable questionnaires would give us 0.75 ± 0.07. All treatments were characterized by medication type, dose, route of administration, and frequency of administration. For the purposes of reporting, we grouped responses into defined categories. For the typical cases, dosages for oral corticosteroids and MTX were broken down into low, medium, and high. An oral corticosteroid dose < 1 mg/kg/day (prednisone or equivalent) was considered low-dose, ≥ 1.0 mg/kg/day and < 1.5 mg/kg/day was considered medium-dose, and ≥ 1.5 mg/kg/day was considered high-dose. A MTX dose ≤ 10 mg/m2/week was considered low-dose, > 10 mg/m2/week and < 20 mg/m2/week medium-dose, and ≥ 20 mg/m2/week high-dose. Intravenous “pulse” methylprednisolone (30 mg/kg/dose) was broken down into 2 categories: the first in which it would be given at “initiation of treatment for 3–5 days” and the second in which it would be used as “ongoing intermittent” therapy (this varied from weekly to monthly). After determining the frequency of use of each treatment individually, we characterized the most common treatment combinations by case. The responses to question 1 and 3 were counted and ranked by frequency of response. The proportion of respondents who indicated they would use corticosteroids, MTX, IVIG, and hydroxychloroquine in the moderately severe case of “typical” JDM were compared between respondent groups stratified by the estimated number of new patients seen per 5-year period using a chi-square test.
RESULTS
The response rate of the survey was 84% (141/167), of which 124 provided meaningful data. The number of respondents per case can be seen in Table 2. Ninety-five percent of respondents work in an academic center. Further characteristics of the respondents are given in Table 3.
Respondent characteristics.
Treatment approaches. Typical cases — combinations of medication
The treatment combinations for each case can be seen in Figure 1. Almost all respondents indicated they would use corticosteroids for each of the 4 typical cases. It was quite uncommon, however, for respondents to indicate that they would use corticosteroids as a single agent (≤ 11% for all cases). The most common combination of treatment regardless of presentation was corticosteroids and MTX, with 38%, 43%, 44%, and 30% of respondents indicating that they would use these medications together in the mild, moderate, severe, and ulcerative cases, respectively. MTX was the most commonly used second-line agent (either with corticosteroid only or with other medications) with 76%, 84%, 79%, and 67% indicating they would use it for the mild, moderate, severe, and ulcerative cases. No respondents indicated that they would use IVIG for the mild case. Eighteen percent of respondents would use IVIG for the moderate case, most commonly in combination with corticosteroids and MTX. Intravenous immunoglobulin would be used relatively more frequently by respondents for the severe and ulcerative cases at 39% and 45%, respectively. Forty-four percent of respondents would use hydroxychloroquine in the mild case, most commonly in combination with corticosteroids and MTX. However, hydroxychloroquine would be used less frequently as the disease presentation became more severe. Cyclophosphamide would be used most commonly in the ulcerative case.

Combinations of medications for treatment of “typical cases.” Steroid: oral or intravenous corticosteroid; MTX: methotrexate; HCQ: hydroxychloroquine; IVIG: intravenous immunoglobulin; CYCLO: cyclophosphamide.
Atypical cases — combinations of medication
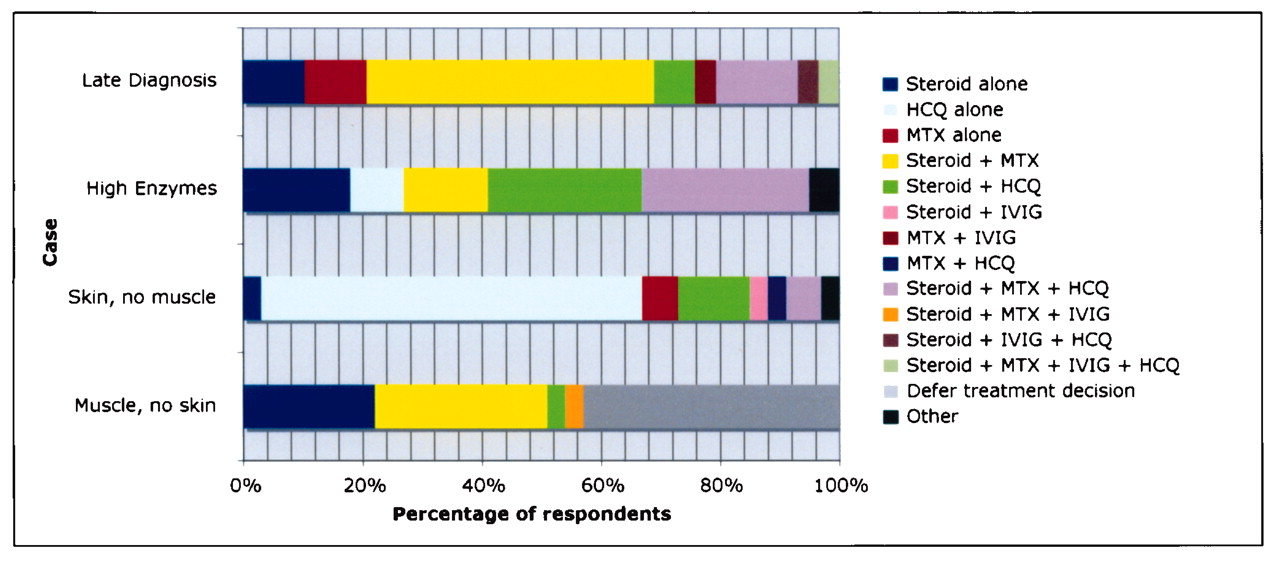
The treatment combinations for the 5 atypical cases were more varied in comparison to typical cases (Figure 2). Almost half of respondents indicated that they would use corticosteroids and MTX for the case of “late diagnosis” in which the patient presented 3 years after the development of symptoms. Twenty-one percent of respondents indicated that they would use a single agent — corticosteroid alone or MTX alone. For the “high enzyme” case characterized by mild clinical disease but persistent elevation of levels of muscle enzymes, the most common combinations were corticosteroids with MTX and hydroxychloroquine, or corticosteroids with hydroxychloroquine, each combination used by approximately one-quarter of respondents. Overall, 71% of respondents indicated that they would use hydroxychloroquine in combination or alone. For the case in which the child had rash but no evidence of muscle involvement, the majority of respondents would use hydroxychloroquine alone. In the case where there was no rash, but features consistent with myositis, almost half of respondents indicated that they would defer treatment decisions until a biopsy was performed. The most common responses, when treatment was described, were corticosteroids alone or in combination with MTX. The responses received for the “lung disease” case were the most variable of the atypical cases. Twenty-five percent of respondents held treatment decisions until further investigations were available, and of the remaining respondents, there were 14 different combinations of treatment (and therefore not shown in Figure 2). Cyclophosphamide, with corticosteroids or alone, was the most commonly suggested treatment.
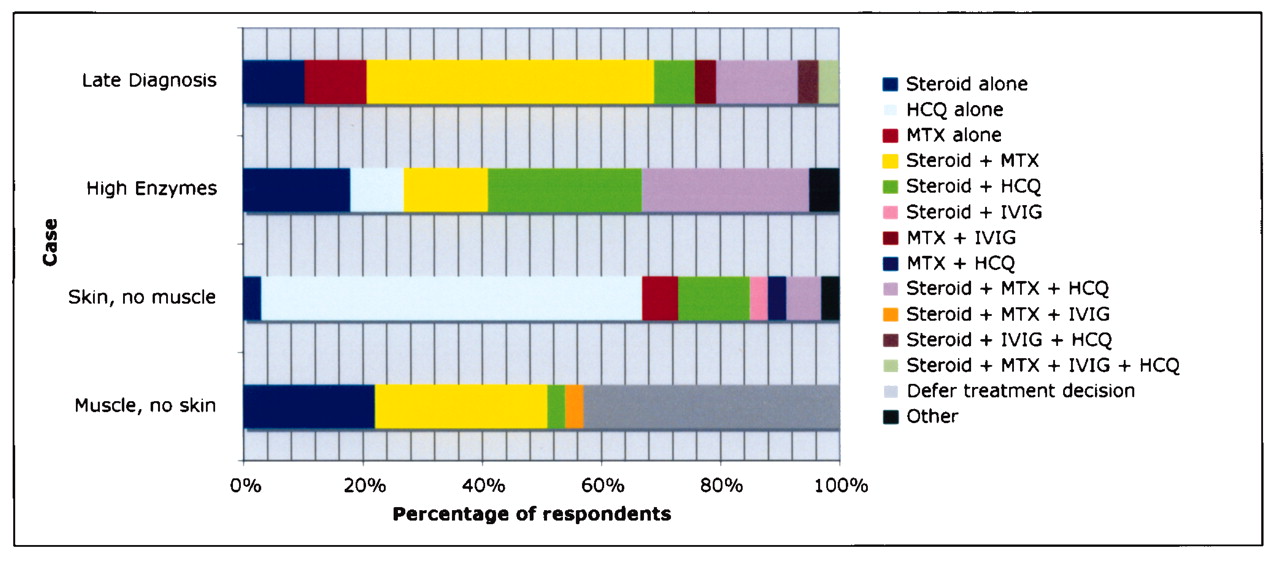
Combinations of medications for treatment of “atypical cases.” See Figure 1 for abbreviations.
Refractory cases
Of all the cases, the 2 refractory cases had the most variable responses, with 25 combinations of medications for the refractory skin case, and 22 for the partial response case. In the “refractory rash” case, hydroxychloroquine was suggested by approximately two-thirds of respondents (30% of respondents as a single agent) and IVIG by just over one-quarter (8% of respondents as a single agent). While medications for the “partial response” case were suggested in many different combinations, the most commonly suggested individual medications were pulse methylprednisolone (44%), increased MTX (44%), IVIG (44%), reduced prednisone (36%), and hydroxychloroquine (35%).
Typical cases — dose, route, and pattern of corticosteroid administration
Almost all respondents indicated that they would use corticosteroids in the mild, medium, and severe cases; however, the manner in which it was given varied (Figure 3). In the mild case, over half of respondents indicated that they would use high-dose oral corticosteroids (this corresponded to a dose of 2 mg/kg/day in all cases). Just fewer than 10% indicated they would use high-dose corticosteroids and daily pulses of IVMP (30 mg/kg per dose) at diagnosis. Nineteen percent would use medium-dose oral corticosteroids alone. Those that use low-dose oral corticosteroids would also use intermittent pulses of methylprednisolone. In the moderate case, 88% of respondents would use pulse methylprednisolone. The most commonly reported regimen was 3–5 doses of daily pulses followed by high-dose oral corticosteroids. Twenty-two percent of respondents did not indicate whether oral corticosteroids would be used in addition to pulses. In the severe case, high-dose oral corticosteroids and IVMP at initiation of treatment was the most common corticosteroid regimen. A higher percentage of respondents would use intermittent pulses in addition to high-dose oral corticosteroids for the severe case (25%) compared with the moderate case (8%). In the ulcerative case, the child in this scenario had already been started on “aggressive therapy.” Many respondents indicated that they assumed the child was on corticosteroids already, and thus details of corticosteroid use could not be analyzed.
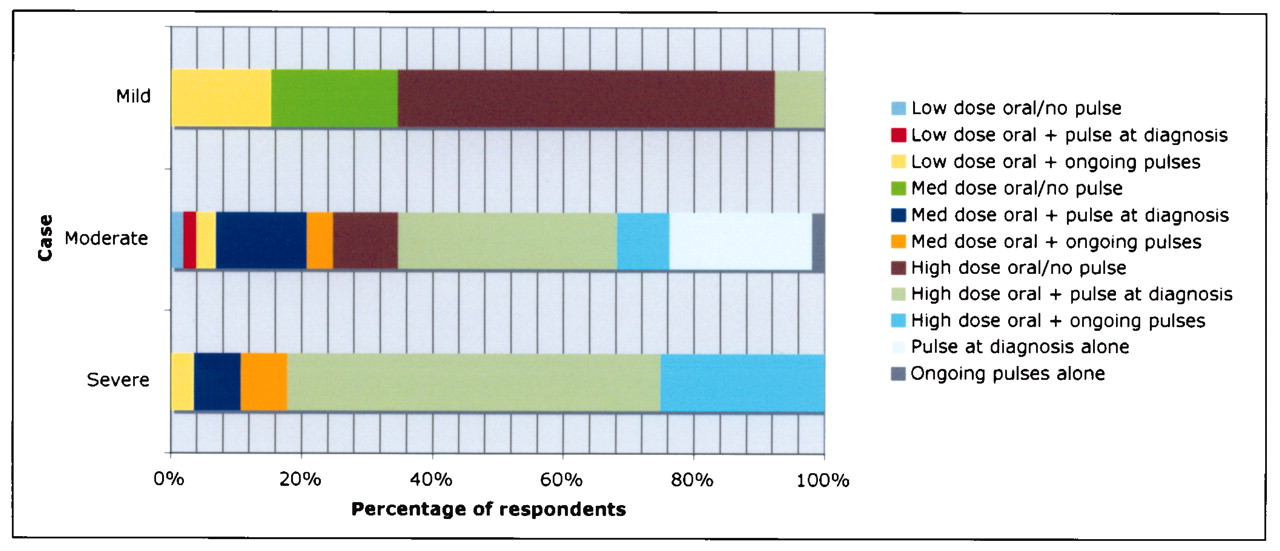
Dose and route of corticosteroids in mild, moderate, and severe cases. Low-dose oral: < 1.0 mg/kg/day; pulse at diagnosis: pulse methylprednisolone (30 mg/kg/dose/day) for 3–5 consecutive days; ongoing pulses: ongoing intermittent pulses; medium-dose oral: ≥ 1.0 mg/kg/day < 1.5 mg/kg/day; high-dose oral: ≥ 1.5 mg/kg/day.
Typical cases — dose and route of MTX administration (Table 4)
Methotrexate (MTX) use in “typical” cases.
The majority of respondents would initiate MTX therapy in medium to high doses regardless of the degree of disease severity of the case. The percentage of respondents who would use medium versus high-dose MTX was essentially divided equally for each case, except in the ulcerative case, in which twice as many respondents would use high-dose over medium-dose. There was a trend toward using oral MTX less commonly as the severity of presentation increased. Overall, the majority of respondents indicated that they would use the subcutaneous route regardless of disease severity (55%–68%).
Investigations
The number of investigations provided to respondents in each case varied, therefore direct comparison from one case to another was not possible. A selection of results from the cases is presented. Most often magnetic resonance imaging (MRI) was the preferred diagnostic test to determine the presence of myositis. Electromyography (EMG) and/or muscle biopsy were requested by less than half of the respondents in cases in which the results of such investigations were not given. For the moderate case, the majority of respondents would investigate swallowing function, with the next most commonly requested tests being a chest radiograph (38%) and von Willebrand factor antigen (31%). Other requested investigations were quite specific to the case, such as a muscle biopsy for the case without characteristic JDM rash, and bronchoalveolar lavage and cardiac evaluation for the case complicated by lung disease.
Nonpharmacologic treatments
The most commonly suggested nonpharmacologic treatments were physiotherapy and occupational therapy, application of sunscreen, and calcium and vitamin D supplementation.
Volume of new patients seen by respondent and treatment preferences
There were no significant differences noted between the use of corticosteroid, MTX, IVIG, and hydroxychloroquine by respondents when stratified by estimated number of new patients seen per 5-year period. We compared respondents seeing > 20 patients (n = 22) with those seeing ≤ 20 patients (n = 86), as well as the former to respondents seeing ≤ 10 patients (n = 50). There were no statistical differences (data not shown).
DISCUSSION
This survey provides a description of treatment approaches taken by a large sample of North American pediatric rheumatologists in response to written clinical case scenarios describing children with JDM. The response rate of the survey was excellent, 84% of those surveyed responding.
Our results demonstrate that corticosteroids are the first line of therapy for children presenting with mild, moderate, and severe JDM. Monotherapy with corticosteroids is rare. MTX is often considered a concomitant first-line agent independent of the disease severity at presentation in the typical cases, whereas IVIG is typically reserved for more severe presentations and for patients with a partial response to standard treatment. Respondents use hydroxychloroquine in cases where children are less severely affected and where rash is prominent or refractory. Cyclophosphamide is reserved for more severely affected cases and when lung disease is present. There are differences in the route of corticosteroid administration, highlighted by the typical cases, where children with more severe disease are more often treated with pulse methylprednisolone. When MTX is given, it is most often used at a dose of 11 mg/m2 per week or higher, with a trend toward doses > 20 mg/m2 for severe ulcerative presentations. Subcutaneous MTX is the preferred route. The investigational approach of respondents to some of the cases shows that MRI is most often used for confirmation of myositis (often in lieu of EMG and muscle biopsy). Respondents use a number of nonpharmacologic treatments, most frequently physiotherapy and occupational therapy.
Corticosteroids continue to be the mainstay of therapy for children with JDM. While randomized controlled trials are lacking, early studies of JDM demonstrated the importance of promptly initiating corticosteroids in reducing complications and poor functional outcomes6,7. It appears, however, that the use of corticosteroids as monotherapy is now quite rare, and most pediatric rheumatologists add MTX as a second agent at the onset of treatment. Subcutaneous administration is preferred, possibly due to concerns of enteral absorption in the context of possible gastrointestinal vasculopathy.
Most respondents indicated that they would not give over 25 mg of MTX in a single dose. MTX has been used in the treatment of JDM for many years, and initially was typically reserved for recalcitrant cases25. A more recent study8 compared 2 groups within a cohort of children with JDM; one group received only corticosteroids as initial therapy, while the second group received corticosteroids and MTX as initial therapy. In the latter group, corticosteroids were tapered more quickly, children experienced less corticosteroid toxicity, and disease control was equivalent8. It appears that in North America, most pediatric rheumatologists are taking this approach regardless of disease severity at presentation.
We found that intravenous methylprednisolone pulses at initiation of therapy is the preferred method of corticosteroid administration for almost 9 out of 10 rheumatologists when treating moderately severe JDM. There are a number of reasons why the use of high-dose IVMP (30 mg/kg/day) could offer a treatment advantage over oral corticosteroids. Patients with active JDM may have decreased bioavailability of oral corticosteroids compared with IVMP secondary to proximal intestinal vasculopathy26. One study found that IVMP compared with oral corticosteroids was potentially cost-effective due to reduction in duration of disease13. Improved outcomes, including a reduction in calcinosis, were also suggested in 2 case series27,28. However, a recent comparative study was unable to find a difference in a host of important outcomes when comparing aggressive IVMP therapy to oral corticosteroids in moderately affected patients, leading to continued uncertainty regarding the most effective and safest route of corticosteroid administration12.
IVIG does not appear to be a therapy that most pediatric rheumatologists would use at initiation of therapy, particularly for children presenting with mild or moderately severe disease. IVIG has been shown to be efficacious in a controlled trial of adults with treatment-resistant dermatomyositis29. In children, IVIG may be effective and allow reduction in corticosteroid dose14,15,16. It remains unclear what benefit there may be in using IVIG as initial therapy for JDM. Its benefits must be weighed against the potential side effects (such as infusion reactions), costs, and risks of exposure to a blood product.
The responses from this survey suggest that there are a number of pediatric rheumatologists who use hydroxychloroquine for cutanous disease and less severely affected patients. Perhaps, with more severe disease and more aggressive treatment, it is felt that hydroxychloroquine is unlikely to offer an additional benefit. Hydroxychloroquine is used in a number of rheumatologic conditions including systemic lupus erythematosus (SLE)30 and rheumatoid arthritis31. It appears to be beneficial particularly in the treatment of the cutaneous manifestations of SLE32. Two case series (one in adults and one in children with dermatomyositis) found that hydroxychloroquine appeared to be helpful, particularly for skin disease17,33. In contrast, there has been a report of rash worsening with hydroxychloroquine34 and another report of a high frequency of cutaneous drug reactions to hydroxychloroquine when treating dermatomyositis35.
Cyclophosphamide is reserved for severely affected children and those with lung disease. However, even in these cases the majority of respondents would not use it at initiation of therapy. Riley, et al reported improvements after 6 months of therapy with cyclophosphamide in a small group of patients with cutaneous ulcerative disease and/or severe systemic manifestations22. Most of these patients were treated after an initial trial of prolonged corticosteroids and other second-line agents. Given the significant side effect profile, it seems reasonable that cyclophosphamide would be reserved for high-risk patients. It is unclear at what level of severity of disease it should be introduced.
The study of biologic agents is at an early stage in the treatment of JDM. In adult studies, anti-tumor necrosis factor (anti-TNF) therapy has not shown consistent benefit and may be associated with flares and worsening of disease36,37. In contrast, a recently described case series of children with refractory JDM treated with infliximab demonstrated improvement in muscle weakness, contractures, and calcinosis38. Anti-TNF therapy was mentioned only a few times in the survey. Rituximab appears more promising in adult studies, with controlled trials under way in adults and children39. At present, however, it is not indicated in the initial treatment of JDM. This survey suggests that cyclosporine, mycophenolate mofetil, and azathioprine are not agents used widely by North American pediatric rheumatologists in the initial treatment of JDM.
The approach to investigations was highly individualized. The survey reconfirms that there is a shift occurring in the approach to diagnosis of JDM. When results of EMG, biopsy, and MRI were not presented, approximately half of respondents indicated that MRI would suffice to diagnose JDM prior to beginning treatment. This is consistent with another survey that showed that MRI is being used frequently in lieu of EMG and biopsy, the latter 2 being more invasive40. The sensitivity and specificity of MRI in diagnosing JDM is unknown; however, MRI is becoming an important diagnostic tool.
Physical and occupational therapy, sunscreen, and calcium and vitamin D supplementation are the most commonly reported nonpharmacologic therapies in this study. There has been relatively less focus on nonpharmacologic therapy in JDM; however, the role of exercise in the treatment and monitoring of JDM has been receiving more attention recently41,42.
Our results must be considered in the light of potential limitations of our study design. As this was a survey using hypothetical cases, the responses may not reflect the true practice of respondents. However, the cases were drawn from “real-life” presentations of JDM and chosen to represent what is seen in clinical practice. In addition, we were unable to include all 11 cases for each participant due to problems with feasibility (11 cases was felt to be too time-intensive in the pilot phase of the study). The responses to the 10 cases (i.e., excluding the “moderate” case) may be less precise, as fewer respondents completed these cases. However, due to the random sampling from the population, response bias was minimized, increasing the likelihood that the results are generalizable to the population sampled. A second limitation is that this survey focused on initial treatment, and due to the wording of the questions, we were unable to glean information regarding the tapering regimens of medications. Many respondents indicated they would modify treatment based on clinical response.
It is emphasized that this study describes treatment preferences of pediatric rheumatologists in North America and is not necessarily representative of treatment preferences in other parts of the world. For example, The Paediatric Rheumatology International Trials Organization (PRINTO) is presently conducting a multicenter single-blind trial with 3 arms, one of which involves prednisone and cyclosporin A43. Our survey suggests that cyclosporin A would seldom be used in the practice of our respondents in the initial treatment of JDM. With limited evidence to support many of the treatments that are used in JDM, it is not surprising that the approach to treatment may vary around the world.
For the majority of North American pediatric rheumatologists, corticosteroids and MTX are the standard of care for typical cases of JDM, even for children presenting with relatively mild disease. There is variability in the route of administration of corticosteroids and use of IVIG and hydroxychloroquine. The results of our survey suggest that the next step in the study of optimizing treatment of JDM could be a prospective observational treatment study where corticosteroids and MTX are included in the basic treatment regimen, with options allowing evaluation of the route of administration of corticosteroids and the addition of IVIG and hydroxychloroquine.
Footnotes
-
Supported by Friends of CARRA (Childhood Arthritis and Rheumatology Research Alliance).
- Accepted for publication April 6, 2010.








{kind=link}
{kind=link}
{kind=link}