

Abstract
Objective. The LupusQoL-US instrument was recently validated in the US. We studied the benchmarks for a US patient cohort with systemic lupus erythematosus (SLE) and relevant demographic and disease correlates.
Methods. LupusQoL-US was administered to 185 patients with SLE. Demographic data (age, sex, ethnicity, marital status) and disease features (duration, disease activity and damage) were assessed simultaneously. Descriptive statistics were obtained. LupusQoL-US domain scores were calculated, and compared by sex, ethnicity, and marital status using nonparametric tests. Correlation between LupusQoL-US domains and age, disease duration, disease activity, and disease damage were obtained.
Results. Mean age of patients was 42.2 ± 14.5 years; 94% of subjects were women. African American patients comprised 60% of the study cohort. The most affected domains were Fatigue and Physical Health. The least affected was Intimate Relationships. Age correlated with Physical Health, Pain, and Body Image (r = 0.15–0.18). Differences were observed based on sex and marital status, but not by ethnicity; there the LupusQoL-US correlated inversely with disease activity (r = −0.001 to −0.36) and damage (r = −0.003 to −0.40).
Conclusion. All domains of the LupusQoL-US based health related quality of life (HRQOL) were affected adversely. HRQOL varied by age, sex, and marital status in our SLE cohort.
- SYSTEMIC LUPUS ERYTHEMATOSUS
- HEALTH RELATED QUALITY OF LIFE
- SYSTEMIC LUPUS ERYTHEMATOSUS DISEASE ACTIVITY INDEX
- SLICC-ACR DAMAGE INDEX
Systemic lupus erythematosus (SLE) is a multisystemic autoimmune disease that predominantly affects young women. It affects multiple facets of a patient’s health and life, leading to a poor quality of life.
Health outcomes in SLE are traditionally measured using physician or laboratory based assessments. Physician based assessments include physician’s global assessment of disease activity and damage. Use of patient reported outcomes is encouraged since it provides information that is understandable and relevant to the patient and provides unique information that may be known only to the patient.
Health related quality of life (HRQOL) is one such patient reported outcome measure widely used in medical research. In SLE, HRQOL has been reported in several studies to be poor1,2,3. We previously reported that the HRQOL in patients with SLE may indeed be worse than in other common chronic diseases1. A poor correlation between disease activity, damage, and HRQOL has been noted in several studies1,4. Generic measures of HRQOL [e.g., the Medical Outcomes Study Short Form-36 (SF-36)] have been found not to be sensitive to changes in disease activity among SLE patients5. This may be partly due to the poor correlation between disease activity and damage with HRQOL or lack of some domains considered pertinent by SLE patients (e.g., sleep, concentration, effects of visible disfigurement, planning) in generic tools such as the SF-366,7. Disease-specific patient reported outcome measures may not only include pertinent domains, but also be sensitive to changes in the disease status. Further, the US Food and Drug Administration encourages use of patient reported outcome measures for drug development and testing. The LupusQoL-US instrument is the modified version of the LupusQoL8 for US patients and has undergone inter-cultural validation9. We describe the LupusQoL-US benchmarks for our SLE study cohort and its correlation with demographic and disease features.
MATERIALS AND METHODS
Consecutive patients with SLE attending the rheumatology outpatient clinics at Rush University Medical Center and John H. Stroger Hospital, Chicago, were approached to participate in this study. A total of 185 consenting patients were enrolled and self-administered the LupusQoL-US. All patients met the American College of Rheumatology (ACR) classification criteria for SLE10.
LupusQoL-US has 8 domains9: Physical health (PH), Pain (PN), Planning (PL), Intimate Relationships (IR), Burden to others (BU), Emotional health (EH), Body image (BI), and Fatigue (FA). The domain scores range from 0 to 100, where 100 represents best HRQOL.
Demographics and disease duration and activity were assessed. The latter was done using the Safety of Estrogens in Lupus Erythematosus National Assessment–Systemic Lupus Erythematosus Disease Activity Index (SELENA-SLEDAI) tool11. This includes a physician global assessment, along with clinical features present during the past 10 days. Flare assessment for mild and moderate/severe flare is available. Higher scores represent greater disease activity. Disease damage was measured using the Systemic Lupus International Collaborating Clinics/ACR Damage Index (SLICC-ACR SDI), where organ damage for the past 6 months is assessed12. Higher scores represent greater damage. Medical chart reviews were done to determine the serological and clinical disease manifestations to describe the study group and SDI.
The study was approved by the local Institutional Review Board.
Statistical analysis
Summary scores were calculated for each domain of the LupusQoL-US. Descriptive statistics were obtained for age, disease duration, disease activity, and damage. Correlations of LupusQoL-US domains with age, disease activity, and damage were obtained (Spearman’s correlation coefficients r). Mann-Whitney test was used to compare the LupusQoL-US domain scores by sex, marital status, and ethnicity.
Significance of correlations between 2 variables was defined by Cohen’s guideline: none (0.09 < r > 0.0), small (0.3 < r > 0.1), medium (0.5 < r > 0.3), and large (1.0 < r > 0.5). A p value ≤ 0.05 was considered significant.
RESULTS
The description of the study cohort is shown in Table 1. Twenty-three percent of the subjects had fibromyalgia along with SLE. The mean LupusQoL-US scores are shown in Table 2. Of all the LupusQoL domains, Fatigue and Physical health domains were the most affected in our study cohort, followed by Pain, Planning, and Burden to others. The domain Intimate relationships was the least affected. Figure 1 compares HRQOL findings in our study cohort with the referent UK cohort8.
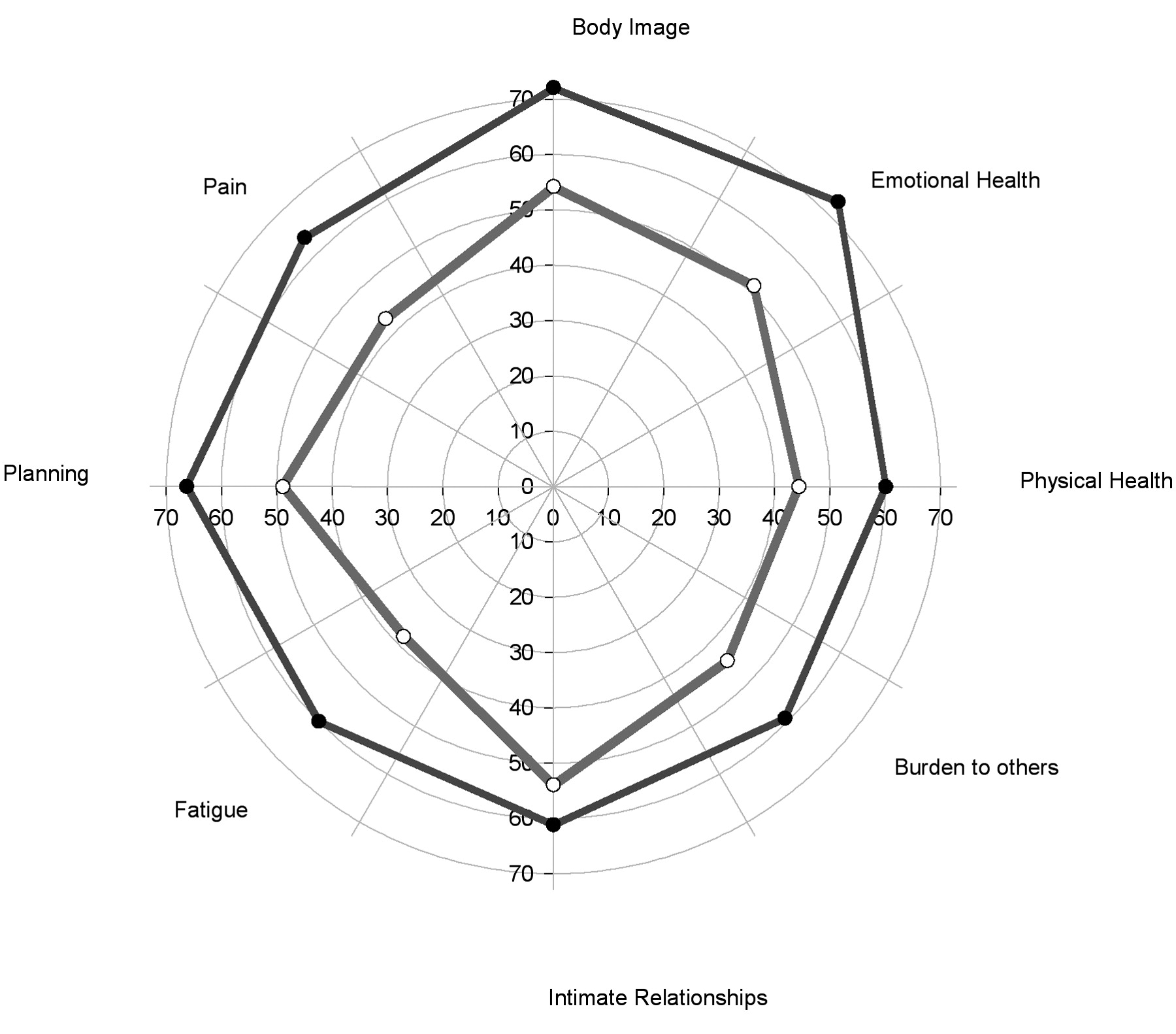
HRQOL domain findings in the US study cohort (inner ring) compared with the referent UK cohort (outer ring).
Description of the study cohort.
Summary scores for LupusQoL-US domains, correlation with age and disease duration.
HRQOL and demographics
Associations were observed between age and the LupusQoL-US domains of Physical health, Pain, and Body image (Table 2). There was no correlation between disease duration and LupusQoL-US scores (Table 2). Significant differences were observed in the LupusQoL-US domain scores by gender (Table 3). Women had lower scores than men in the domains of Physical health, Intimate relationships, Emotional health, and Fatigue. Differences in LupusQoL-US domain scores were also observed by marital status (Table 3). Married participants scored better in Physical health and Planning domains, whereas unmarried participants scored better in the Intimate relationship domain. A trend was noted towards less pain among married subjects. There were no significant differences in the HRQOL based on ethnicity.
Summary scores for LupusQoL-US by sex and marital status. Data are mean ± SD (interquartile range).
HRQOL and disease activity
Detailed results are shown in Table 4. The Planning domain correlated with the physician global assessment. Only results with p ≤ 0.01 are summarized below. Total SLEDAI score correlated with all domains except Intimate relationships and Body image. The correlation of total SLEDAI score was highest for the Planning (r = −0.26) and Burden to others (r = −0.21) domains.
Correlation of LupusQoL-US with disease activity.
Physical health correlated most with arthritis (r = −0.35) and fever (r = −0.31), although significant but weaker relationships were observed with alopecia and SLEDAI score. Pain correlated most with arthritis (r = −0.34) and alopecia (r = −0.33), while Planning correlated with arthritis (r = −0.29), total SLEDAI (r = −0.26), and fever (r = −0.24). Intimate relationships correlated with alopecia (r = −0.34); Burden to others with alopecia (r = −0.36), low complements (r = −0.25) and fever (r = −0.24). Emotional health was most correlated with leukopenia (r = 0.25), alopecia (r = −0.24), fever (r = −0.23), and headache (r = −0.23). Body image was associated with alopecia (r = −0.32) and leukopenia (r = 0.29), while Fatigue was most associated with alopecia (r = −0.30).
HRQOL and disease damage
Total SDI scores were most associated with the Physical health (r = −0.22) and Planning (r = −0.20) domains. Physical health (r = −0.35), Pain (r = −0.33), Planning (r = −0.40), Emotional health (r = −0. 38), and Fatigue (r = −0.35) domains correlated most with neuropsychiatric damage (Table 5). Burden to others correlated with musculoskeletal damage (r = −0.27), while skin damage was associated most with the Body image (r = −0.25) and Fatigue (r = −0.27) domains.
Correlation with SDI (SLICC-ACR).
DISCUSSION
Generic tools for measuring patient reported health outcomes are limited in their inclusion of domains specifically affected in patients with SLE. Also, the tool may not be sensitive to changes in the disease. Disease-specific tools for SLE include SLEQOL13, LupusQoL8, LUP-QOL14, L-QOL15, and LupusPRO16. Each tool has its strengths and weaknesses. Currently, none of these disease-specific tool have been tested in clinical trials. LupusQoL was developed from feedback from women with SLE who were predominantly of Caucasian ethnicity.
We present the benchmarks for LupusQoL-US from our lupus study cohort. The most affected domain was Fatigue, a common complaint in patients with SLE17,18,19,20. The least affected was intimate relationships. However, the latter observation may be confounded by the sensitive nature of the question. Patients may not feel comfortable sharing this information, and missing and incorrect data are frequently found in studies focused on intimacy. Comparison with referent UK LupusQoL cohort data is not ideal, since the study cohorts differ significantly in demographic and clinical characteristics. Within those limitations, the following observations were made: HRQOL in a US cohort was worse than in the UK patients in all domains; and the pattern of domain scores was nearly the same in the 2 samples, except for the Fatigue, Emotional health, and Pain domains, which were disproportionately lower among the US patients.
We found an inverse association between age and physical health and pain. This is plausible, since physical health and functioning decline with aging. Similarly, pain may be associated with age related degenerative joint disease and other coexistent comorbidities. Others have reported similar findings2,21,22 regarding HRQOL and age in SLE. Increasing pain with age has been previously noted23. We found no association of HRQOL with disease duration in our study. Gladman, et al also reported a lack of association between HRQOL and disease duration24.
We found significant differences in the HRQOL by sex and marital status. These results are not consistent with those of other studies in SLE25,26. However, men have been found to have better HRQOL as compared to women27,28. Moreover, studies report that the frequency of SLE relapses is lower among men29, and that men may have less severe forms of SLE30. Cervera, et al found less arthritis in male patients with SLE31. The number of men in our study was small, thus limiting our confidence in this observation. However, SLE does predominantly affect women and thus is a uniform feature of this disease. Unless a study is designed specifically to address the differences in HRQOL by sex, this limitation will be present in most SLE studies. More studies are needed to confirm these findings.
In our study, married participants with SLE had a better HRQOL, in comparison to worse HRQOL in the study by Alarcon, et al21. However, other reports show that unmarried SLE subjects are more likely to be noncompliant with care32,33. Marital status is known to be associated with better health outcomes in general34,35. In our study, married participants scored worse on the Intimate relationship domain. Possible reasons for this may include the stress of care-giving, household chores, parenting, and on the quality of the relationship. These issues may need further research.
Significant albeit weak to moderate associations between HRQOL, disease activity, and damage were noted. These findings are consistent with those of others1,4,24. The associations were plausible, e.g., arthritis with Physical health and Pain domains, and alopecia with Body image. Neuropsychiatric damage was associated with Physical health, Pain, Planning, Emotional health, and Fatigue domains, skin damage with the Body image domain. Surprisingly, presence of diabetes was associated with the Planning and Burden to others domains, although weakly.
Some limitations of our study include the generalizability of the results, as the patient population was not representative of community patients with SLE, since patients were recruited from 2 tertiary care hospitals. Also, the ethnic makeup of the study cohort was more representative of the patients seen in our inner city hospitals in Chicago. However, this is the first study to our knowledge reporting benchmarks for our study cohort. Also, this is the first study to note an association between gender, marital status, and HRQOL using the LupusQoL-US.
- Accepted for publication April 7, 2010.








{kind=link}