

Abstract
Objective. By 2026, there will be a 64% shortfall of rheumatologists in Canada. A doubling of current rheumatology trainees is likely needed to match future needs; however, there are currently no evidence-based recommendations for how this can be achieved. The Workforce in Rheumatology Issues Study (WRIST) was designed to determine factors influencing the choice of rheumatology as a career.
Methods. An online survey was created and invitations to participate were sent to University of Western Ontario (UWO) medical students, UWO internal medicine (IM) residents, Canadian rheumatology fellows, and Canadian rheumatologists. Surveys sent to each group of respondents were identical except for questions related to demographics and past training. Participants rated factors that influenced their choice of residency and scored factors related to the attractiveness of rheumatology and to recruitment strategies. Statistical significance was determined using chi-squared and factor analysis.
Results. The survey went out to 1014 individuals, and 491 surveys were completed (48.4%). Responses indicated the importance of exposure through rotations and role models in considering rheumatology. Significant (p < 0.002) differences between groups were evident regarding what makes rheumatology attractive and effective recruitment strategies, most interestingly with rheumatologists and trainees expressing opposite views on the latter.
Conclusion. Recommendations are made in 2 broad categories: greater exposure and greater information. As medical students and IM residents progress through their training, their interest in rheumatology lessens, thus it is important to begin recruitment initiatives as early as possible in the training process.
It has been estimated that by 2026, 6 million Canadians will have arthritis1,2. A 64% shortfall in required rheumatologists is projected by that year1,2,3. Further, as the Canadian population ages, the shortfall in rheumatologists will likely increase4. Low numbers of rheumatologists can substantially increase patients’ wait times, leading to inadequate care4. A majority of Ontario rheumatologists have reported that long wait times were a barrier to providing quality patient care4. The median time from referral to assessment for nonurgent cases was reported to be 8 weeks, and many rheumatologists reported substantial difficulties in accommodating urgent consultations4. The delay in initiating treatment can increase joint damage, thus worsening functional disability and employment disability, and increasing the need for joint replacement5.
Insufficient enrollment in rheumatology subspecialty programs has been identified as a major problem in rheumatology2,3,4. The Canadian Council of Academic Rheumatologists completed a detailed analysis of the status and future trends in enrollment at Canadian academic rheumatology centers in 20012. The council determined that it would be necessary to double the number of candidates entering rheumatology training programs to match projected needs2. While enrollment in rheumatology fellowship programs in Canada has increased since 2001, it is still not near the level needed to meet projected future needs.
From 2004 to 2007, there was a 16% increase in the number of Canadian internal medicine (IM) subspecialty trainees; however, the number of rheumatology fellows increased by only 3%. Over the same time period, only 1% of the 114 new subspecialty trainees in Canada went into rheumatology6. Recently, the discrepancy in recruitment between procedure-based and nonprocedure-based IM subspecialties has been highlighted7. Several studies of nonprocedure-based subspecialties in Canada have been undertaken to find the cause of the discrepancy and to determine effective recruitment strategies7,8,9,10. Despite concerns about a dwindling rheumatology workforce, there has been very little research exploring factors that affect medical student recruitment11,12. Our goal was to investigate this issue through the Workforce in Rheumatology Issues STudy (WRIST). WRIST was designed to determine which factors influence the choice of rheumatology as a career among medical students, IM residents, rheumatology trainees, and practicing rheumatologists by examining the differences between groups. There have been no other in-depth studies of factors influencing rheumatology as a career choice to date.
MATERIALS AND METHODS
The WRIST survey was designed as a cross-sectional prevalence study, with a descriptive, group-comparison design. The WRIST survey used data gathered from medical students, IM residents, rheumatology fellows, and rheumatologists to determine factors that make rheumatology an attractive or unattractive specialty choice and methods to increase recruitment into Canadian rheumatology programs.
The WRIST survey was designed after a thorough literature search of recruitment and workforce issues facing the various residency programs; in particular, the Geriatric Recruitment Issues Study (GRIST) survey was used as a model7,8,9,10,13,14,15,16,17,18,19 because that survey had been validated and shown to be reliable8. A written version of our survey was pretested on a small sample of 6 for readability and comprehension. The pretest sample included medical students, medical residents, 1 rheumatology trainee, and 1 rheumatology nurse. Only minor formatting changes were needed. Two different individuals then piloted each online survey for ease of use and errors. No changes were needed after this stage of piloting.
All medical students (n = 566) and IM residents (n = 79) at the University of Western Ontario (UWO) were contacted by e-mail and asked to participate in our study. Program directors of each of the country’s rheumatology fellowship training programs were contacted and asked to share our online survey with their fellowship trainees (n = 41). Rheumatologists (n = 328) were contacted through the Canadian Rheumatology Association (CRA) member database. Two followup e-mails and an incentive draw were used to maximize the response rate. Participants had the option to enter the incentive draw directly through the online survey tool or indirectly through a separate e-mail address, to maintain anonymity.
Surveys sent to each group of respondents were identical except for questions related to demographics and past levels of training. Participants rated 24 (medical students) or 25 (IM residents, rheumatology fellows, rheumatologists) factors that influence their choice of residency (“not at all important” to “extremely important”). Participants also scored 28 factors related to the attractiveness of rheumatology (“very unattractive” to “very attractive”) and 11 recruitment strategies (“very ineffective” to “very effective”). Questions were also asked about previous rheumatology rotations, role models/mentors, and experiences with people with arthritis. Three open-ended questions asked for the greatest strengths of rheumatology, the biggest deterrents to choosing rheumatology, and the single best recruitment strategy. All Likert scales used in the survey had 5 points: 2 positive, 2 negative, and 1 neutral.
Of note, in Canada, rheumatology rotations are considered elective during medical school. Most IM residents will complete some rheumatology training, although many will do so in the final months of their residency, when they have already chosen a specialty.
Data were gathered using the MRInterview online interface (SPSS Inc., Chicago, IL, USA). Quantitative analysis was completed using SPSS 17.0. Positive responses were identified as the 2 most positive options (very important/extremely important, agree/strongly agree, attractive/very attractive, or effective/very effective). Negative responses were identified as the 2 most negative options (not at all important/not very important, strongly disagree/disagree, very unattractive/unattractive, or very ineffective/ineffective). Chi-squared analysis was used to determine significance. A Bonferroni correction was used to adjust levels of significance for multiple testing. Factor analysis was performed on the data using principal components extraction and varimax rotation. The number of factors to extract was determined by their eigen value, scree plot examination, and parallel analysis. Only items with factors loadings > 0.3 were considered for factor inclusion. Factors were then examined for internal consistency using Cronbach’s alpha coefficient. Qualitative responses were coded by the authors using emergent theory.
The Research Ethics Board at UWO approved this study in 2008. Data collection occurred between May 2009 and July 2009.
RESULTS
The survey was completed by 239 medical students, 34 IM residents, 9 fellows, and 209 rheumatologists (response rates of 42.2%, 43.0%, 22.0%, and 63.7%, respectively). The overall response rate was 48.4% (491/1014). Twenty-five rheumatologists were removed from data analysis after indicating that they did not complete a general IM residency prior to their rheumatology training. The group of rheumatology fellows was statistically under-powered because of the low response rate; thus, it was analyzed together with practicing rheumatologists in the group “practitioners.” The demographic data of participants are shown in Table 1.
Sex and age of study participants by training level.
Unfortunately, we were unable to compare the demographic features of survey responders to survey nonresponders. Because of the online, anonymous design of the survey, we were unable to link nonresponders to any demographic information.
Factor analysis and reliability testing
Five factors were extracted from the items related to specialty choice. Five factors were also identified from the items making rheumatology attractive/unattractive. Analysis of recruitment strategies revealed 2 relevant factors (Table 2). High factor loadings and Cronbach’s alpha coefficient confirmed the integrity of the factor analysis.
Principal component analysis, factor extraction, and internal reliability testing.
Interest in rheumatology
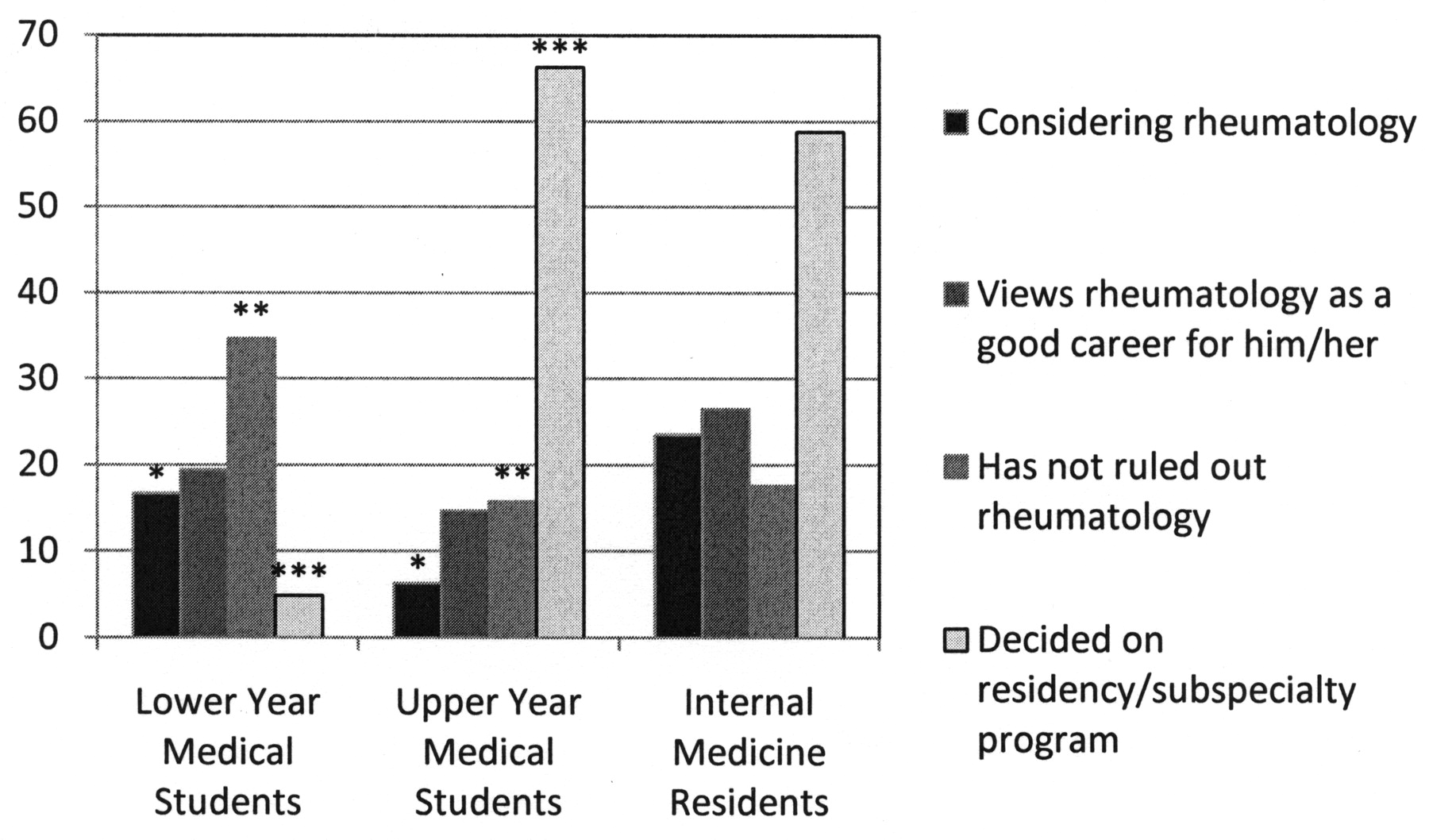
A total of 12.6% of medical students reported considering rheumatology, 17.6% reported that rheumatology would be a good career for them, and 27.2% claimed that they have not yet considered rheumatology but may do so in the future. Not surprisingly, IM residents were more likely to consider rheumatology: 23.5% agreed or strongly agreed that they were considering rheumatology, 26.5% reported that rheumatology would be a good career for them, and 17.6% claimed that they have not yet considered rheumatology but may do so in the future. There is no difference in rheumatology interest between the sexes at either level of training. Among medical students, 29.3% indicated that they have already chosen a residency program. A majority of first-year residents (73.3%; 11/15) and 42.9% (3/7) of second-year residents had not yet decided on a subspecialty (Figure 1).
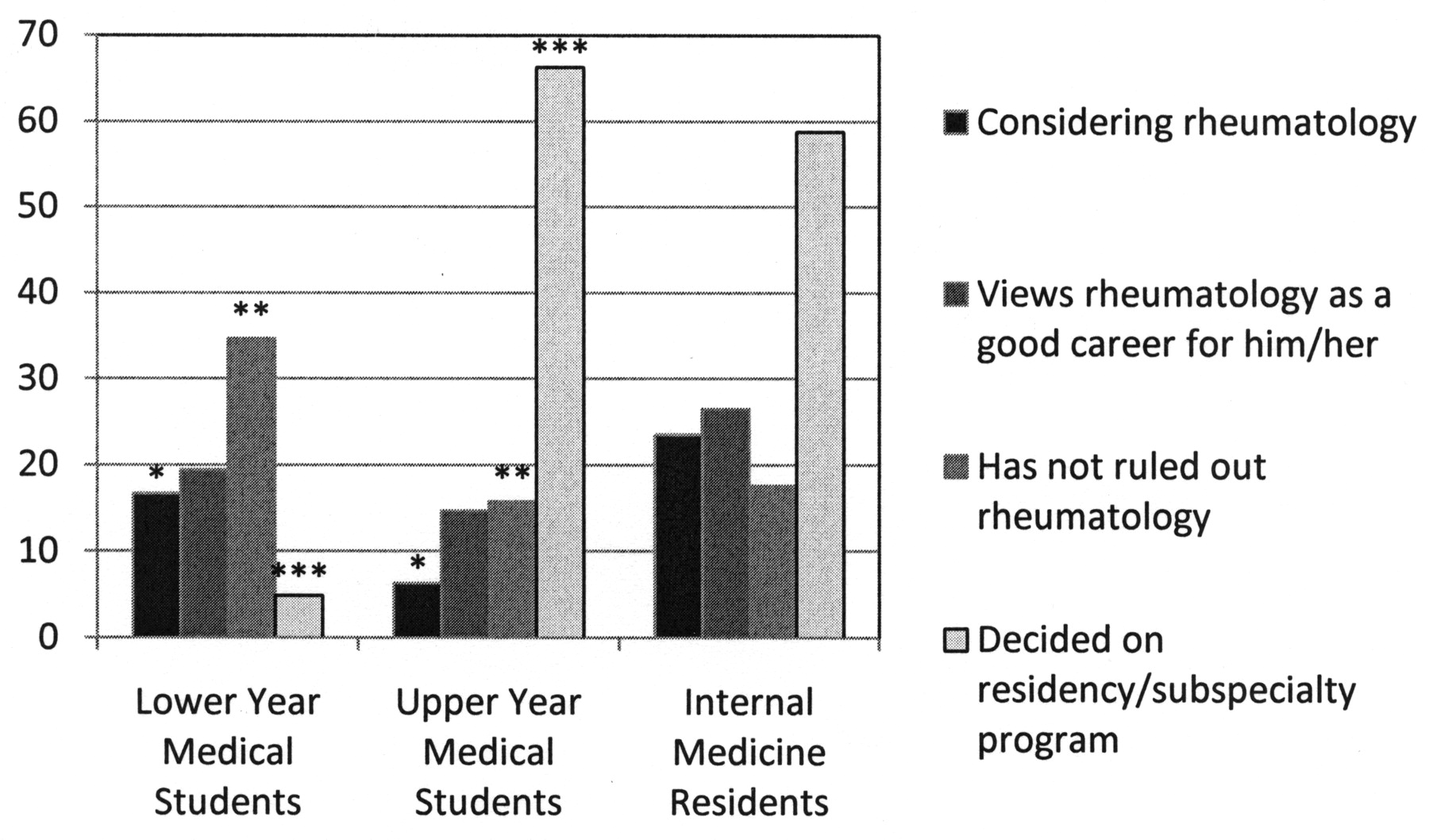
Interest in rheumatology, by percentage, stratified by year of medical training. Lower-year medical students include first-year and second-year students. Upper-year medical students include third-year and fourth-year students. *p = 0.03; **p = 0.001; ***p < 0.001.
Upper-year medical students and residents who have had a rotation in rheumatology were significantly more likely to report that they were considering rheumatology (p < 0.001) and that rheumatology would be a good career for them (p < 0.001), compared to those who have not had a rotation in rheumatology. A majority (70%) reported that the rotation increased their interest in rheumatology.
Of medical students reporting a physician mentor, 81.3% agreed that their mentor influenced their choice of specialty. Residents were less likely to acknowledge the influence of their mentor, at 65.5%. A mentor influenced the choice of subspecialty for 58.7% of residents. Medical students and residents reporting a rheumatologist mentor were significantly more likely to consider rheumatology (p = 0.002) and believe that rheumatology would be a good career for them in comparison to those without such a role model (p < 0.001).
Interest in rheumatology did not differ significantly between students and residents who have had previous positive experiences with arthritis, both in their personal lives and in their medical school training, and those who had not. However, residents who reported positive experiences with arthritis in their residency training had a significantly higher interest in rheumatology than those who did not (p = 0.005).
Factors affecting specialty choice
The most important factors affecting specialty choice are shown in Table 3. Residents were more likely than medical students (p < 0.002) to rate prestige, opportunity for academic practice, and perception as very important or extremely important influences on specialty choice. Practitioners were more likely than medical students (p < 0.002) to rate prestige, the opportunity for academic practice, call schedule, role model/mentor, income, use of new or advanced technology, the opportunity for clinical research, perception, and the opportunity for administration as very important or extremely important influences on specialty choice. Medical students rated exposure in medical school (p < 0.001) as very important or extremely important, significantly more than rheumatologists. Practitioners were no more likely than residents to significantly rate an item as very important or extremely important, and vice versa. Male students and residents rated the use of new/advanced technology as more important than their female counterparts did (p < 0.001).
Reported factors affecting the choice of a career in rheumatology, according to level of medical training. Numbers represent the percentage of total survey respondents who considered that factor either very important or extremely important.
Factors making rheumatology attractive
The most attractive factors of rheumatology are listed in Table 3. The ratings of factors that make rheumatology an attractive career by medical students and residents were shown to have consistent similarities using chi-squared analysis. Medical students and residents were analyzed as 1 group for the purpose of comparison with rheumatologists.
Practitioners were more likely than medical students and residents to rank the following factors as attractive or very attractive (p < 0.002): job availability, the opportunity for academic practice, patient population, perception, lack of procedures, the opportunity for administration, complexity of patients, management of chronic illness, working with an interdisciplinary team, less competition for residency positions, the opportunity for part-time work, focused/narrow field, new therapies for the treatment of arthritis, treatment of chronic pain, working with ambulatory patients, working with workers’ compensation, and concerns about litigation. Medical students and residents were significantly more likely than rheumatologists (p < 0.002) to rate the opportunity to “make a difference” for individual patients and the intellectual challenge as attractive or very attractive elements of rheumatology.
Female medical students were more likely than males (p < 0.002) to consider the patient population, the opportunity for longterm followup, and working with the whole patient as more attractive.
Effective recruitment strategies
The most and least effective recruitment strategies are shown in Table 4. Again, medical students and residents showed great concordance in their rating of effective recruitment strategies and so were compared to rheumatologists as a single group.
Most and least important reported factors influencing recruitment into rheumatology, according to level of medical training. Numbers represent percentage of survey respondents who considered that factor either very important or extremely important, or very unimportant or extremely unimportant.
Medical students and residents positively rated the effectiveness of increased remuneration and the promotion of positive role models/mentoring significantly more often than rheumatologists did (p < 0.0001). Rheumatologists rated formal outreach programs, invitations to attend national conferences, national awards programs, and formal mentoring as effective or very effective strategies more often than medical students and residents did (p < 0.0001).
DISCUSSION
The WRIST survey has demonstrated that there is considerable interest in rheumatology at both the medical student and IM resident level. However, interest declines significantly from the first and second to the third and fourth years of medical school, perhaps as students gain more exposure to the various specialties and begin to narrow their interests. A similar but not statistically significant trend was seen among IM residents. Another important finding is that very few lower-year medical students have decided on a residency program and two-thirds of R1 and R2 IM residents have yet to choose a subspecialty. These trends suggest that recruitment interventions should be targeted to the early years of both medical school and IM residency, when individuals are least likely to have narrowed their focus.
The importance of early exposure is highlighted again by the fact that rheumatology rotations and rheumatologist role models/mentors both significantly increase interest in the specialty, confirming previous research12. It is difficult to determine whether these experiences increased interest in rheumatology or whether they were sought out by already interested students and residents. The fact that 70% of those who did a rotation said that the rotation increased their interest in rheumatology indicates that rotations are very effective in increasing rheumatology interest regardless of the motivations. Medical students and IM residents further confirmed the importance of rotations and role models by rating their part in recruitment very positively.
Interestingly, practicing rheumatologists rated the promotion of positive role models and mandatory rotations among the least effective recruitment strategies. Also interesting is that while medical students and residents rated national awards programs, invitations to conferences, and formal outreach as some of the least effective strategies, rheumatologists ranked them among the most effective. This discordance merits further investigation, ideally in a controlled fashion, by comparing over time students who have participated in outreach programs and students who have not. The results of such a study would have important implications for current recruitment measures, such as local “Joy of Rheumatology” dinners for UWO medical students and weekend retreats in rheumatology held in Quebec and Ontario.
Differences between the levels of training are also seen in the rating of factors that affect specialty choice. Research has found that medical students and residents report similar answers when asked about factors related to specialty choice8 and it is not clear why our survey revealed a number of differences. As well, responses given by residents and practitioners were extremely concordant. These findings suggest that the importance placed on various factors changes during the training process, possibly most often at the resident level.
Not surprisingly, what is considered attractive about rheumatology also differs between medical students/IM residents and rheumatology practitioners. The former more highly rate nonclinical, lifestyle considerations while the latter indicate clinical and patient population characteristics most favorably. As medical students rank lifestyle considerations most favorably, it makes sense that they view these factors as most attractive. Both medical students and residents rated the perception of the specialty very unfavorably; however, both groups indicated that perception is not an important factor in selecting a specialty. Also given low importance were income and level of debt, supporting research that finds that lower salaries are not a deterrent for specialty selection14,16.
Research has indicated that male and female medical trainees are more greatly influenced by different factors related to specialty choice13. While such a finding was not supported by the WRIST survey, it was revealed that female medical students were significantly more likely to rate characteristics of the rheumatology patient population and doctor-patient interaction more highly than males. This indicates that female medical students may be more interested in the type of chronic, longterm care provided by rheumatologists. It has been suggested that rheumatology as a specialty is becoming feminized20,21, something that is supported by the difference in sex ratio between junior rheumatologists/ rheumatology fellows and more senior practitioners. With more women entering medical school than ever before, more medical students may come to realize that rheumatology provides both the lifestyle and patient interactions that they seek. However, research indicates that the move toward “lifestyle” specialties is not being driven by greater numbers of female physicians22,23. Therefore, we cannot be sure how the increasing number of female medical students will affect rheumatology.
Our study has several limitations. While efforts were made to include multiple institutions, medical students and IM residents were ultimately recruited from a single Canadian medical school. The main reason for this restriction was inability to obtain research ethics board (REB) approval from multiple centers. This may limit the possibility of generalizing our results to other centers. We also did not ask whether the IM residents applied to multiple subspecialty programs, nor did we explore how their final decision of subspecialty was decided. As well, less than one-quarter of rheumatology fellows responded to our survey. This may be due in part to the method of recruiting them, which involved contact through a third party. It is not known what would have been found if sufficient responses to be analyzed separately had been received. Because of the low numbers of responding rheumatology fellows, their responses were sometimes combined with those of practicing rheumatologists. However, one could argue that a rheumatologist who has been practicing for many years may have a significantly different viewpoint compared to that of a new rheumatology trainee.
A third party was also used to recruit practicing rheumatologists, and while the vast majority of Canadian rheumatologists are members of the CRA, it is not known what the effect would be if nonmembers were included. Lastly, although a large number of Quebec rheumatologists participated, only recruitment e-mails and not the survey itself were bilingual, and it is not known how many francophone physicians were subsequently excluded.
We have formulated several recruitment strategies that could be implemented at medical schools and IM residency programs. These recommendations fall under 2 headings: greater exposure and greater information. Recruitment strategies should be implemented in the first years of medical school and IM residency. That is when interest in rheumatology is highest and commitment to a specialty is lowest.
Greater exposure
Increase the number of medical students and IM residents who do rheumatology rotations by either making them mandatory or formally promoting them and providing travel stipends. Encourage students to complete these rotations as early as possible in their training.
Provide funding for lower-year medical students to complete rheumatology studentships. Allow students to book studentships for shorter, more convenient periods of time and encourage the experience of both academic and rural settings. Funding can be taken from formal outreach programs and conference invitations, which medical students and IM residents deemed less effective tools.
Encourage lower-year medical students to participate in short rheumatologist shadowing experiences. Create a database of interested rheumatologists, both academic and rural, who will provide a glimpse into the specialty for a few hours.
Greater information
Create a national rheumatologist mentor database where medical students can be put in contact with a role model who can provide information about rheumatology and dispel any misinformation concerning the specialty.
Create and dedicate online space where students can find information, ask questions, and link to a role model or observership supervisor in their area.
Focus promotional information on the factors deemed most important by medical students and residents. Remember that while rheumatologists are more attracted to the patient population and physician-patient relationship characteristics, students and residents find lifestyle and family considerations more attractive features of the specialty.
The implementation of these recommendations may greatly benefit the field of rheumatology as a whole. Unfortunately, the greatest stumbling block for recruitment may be funding available for training programs. Current government funding of IM subspecialty training programs is often competitive, and can limit the number of trainees to a few per center.
Acknowledgments
Christine Charnock of the Canadian Rheumatology Association and Ana Malbrecht of the UWO Department of Medicine helped contact study participants. The authors also thank everyone who completed the survey.
Footnotes
-
The UWO Summer Research Training Program provided funding to complete this research.
- Accepted for publication March 19, 2010.








{kind=link}