

Abstract
Objective. To describe enhanced magnetic resonance imaging (MRI) features and characteristic entheseal changes in the knees in patients with seronegative spondyloarthropathy (SpA).
Methods. The 56 patients included 30 with psoriatic arthritis, 5 with ankylosing spondylitis, 5 with reactive arthritis, 5 with ulcerative colitis (UC), 5 with Crohn’s disease, and another 6 with skin psoriasis. Controls were 20 healthy subjects without knee complaints. MRI was performed in all participants, emphasizing entheseal sites.
Results. Both knees were studied in 45 (80.3%) patients and one knee in 11 (19.6%). MRI showed evidence of bone marrow edema in 13 (23.2%) patients, cartilaginous erosions in 18 (32.1%), and bone erosions in 9 (16.1%). Enthesitis was found in medial collateral ligaments in 18 (32.1%), lateral collateral ligaments in 8 (14.3%), posterior cruciate ligaments in 3 (5.35%), patellar tendon in 18 (32.1%), biceps femoris insertion in 3 (5.35%), medial patellofemoral ligaments (MPFL) in 5 (8.9%), and lateral patellofemoral ligament in 1 patient (1.8%). In the UC and Crohn’s patients (n = 10), 2 had bone erosions and 5 had enthesitis. In the skin psoriasis group (n = 6), one had bone marrow edema; enthesitis was detected in 5 at the patellar tendon insertion and in one in the MPFL. Entheseal-related changes were absent in the controls.
Conclusion. This is the first study showing entheseal-related changes in the knees in patients with inflammatory bowel disease or skin psoriasis without clinical arthritis. Enthesitis of the knee on MRI may be an early finding in SpA.
- MAGNETIC RESONANCE IMAGING
- KNEE JOINT
- ENTHESITIS
- PSORIASIS
- SERONEGATIVE SPONDYLOARTHROPATHIES
- INFLAMMATORY BOWEL DISEASE
Enthesitis is a common feature of spondyloarthropathy (SpA), but is clinically recognized in only a minority of inflamed joints; this may be explained by factors such as the intraarticular and deep location of entheseal insertions and the proximity of entheseal regions to synovium. If enthesitis is the primary event, it would be expected to precede synovitis and to resolve prior to synovitis1. Prospective studies in patients with early SpA will be necessary to determine whether enthesitis and synovitis coexist at all stages of synovitis or if in fact synovitis eventually becomes autonomous. Barozzi and coworkers2 described the magnetic resonance imaging (MRI) features of enthesitis as being characterized by “swelling of the entheseal region and deviation from the normally uniform low signal intensity of tendons and ligaments, with distension of adjacent bursae by fluid collection, peritendinous soft tissue swelling and inflammation of bone adjacent to the insertion.”
To date, most studies have examined MRI changes in the hand joints of patients with rheumatoid arthritis (RA) and seronegative SpA, most commonly psoriatic arthritis (PsA) and reactive arthritis (ReA)3,4,5,6,7,8. McGonagle and colleagues1 were the first to describe characteristic MRI entheseal changes involving the knee joints in a cohort of 10 patients with SpA (3 of whom had PsA) with knee swelling of recent onset. They observed an increased signal on T2-weighted images, characterizing “focal extracapsular fluid/edema” in entheseal portions of the patellar tendon, the iliotibial band, and adjacent to the posterior capsule of the knee. Perientheseal bone marrow edema (BME) was present in 6 patients with SpA, including one with PsA, in whom it involved bone at the tibial plateau as well as bony attachments of the patellar tendon and posterior cruciate ligament. These findings suggest that knee synovitis in patients with early PsA and SpA-associated monoarthritis/oligoarthritis is often characterized by clinically unrecognized enthesitis near the swollen joint, which suggests that enthesitis may be the primary lesion. This is supported by the observation that enthesopathic inflammation may extend as far as the synovial cavity1.
We compared MRI findings of the knee joints in 3 groups of patients, undifferentiated arthritis (UA; n = 25), established RA (n = 15), and SpA (n = 15). In our study special emphasis was given to the following entheseal sites, which were carefully evaluated for abnormalities: the quadriceps tendon insertion, the proximal and distal patellar tendon, the iliotibial band insertion, the lateral collateral ligament (LCL) origin and insertion, the lateral capsular insertions, the cruciate ligaments’ origins and insertions, the biceps femoris insertion, the semimembranosus insertion, and the medial collateral ligament (MCL) origin and insertion. We observed that enthesitis was a common feature on MRI in the SpA group, which was totally absent in the group of patients with RA, and was observed in 3 patients in the UA group. This latter finding may have clinical implications for classification purposes, and can help to determine the developing pattern of patients presenting with UA of the knee joint9.
These lines of evidence inspired us to look for entheseal changes with enhanced MRI in the knee joints in a series of patients with SpA, including PsA, ankylosing spondylitis (AS), and ReA, as well as in cases of ulcerative colitis (UC) and Crohn’s disease; we also examined patients with skin psoriasis without clinically evident synovitis and compared these with healthy controls.
MATERIALS AND METHODS
Study population
A total of 56 patients were studied, including 30 consecutive patients with PsA, 5 patients with AS, 5 with ReA, 5 with UC, 5 with Crohn’s disease, and a random sample of 6 patients with skin psoriasis only and with no clinical evidence of synovitis upon clinical examination. All patients were diagnosed according to the European Spondylarthropathy Study Group preliminary classification criteria10. Endoscopic and histopathologic diagnosis was obtained in all patients with inflammatory bowel disease (UC and Crohn’s disease).
Twenty age and sex matched healthy subjects with no knee complaints served as controls.
Clinical evaluation and assessment
At baseline, a full history was taken, and a complete clinical examination was performed. Detailed rheumatological examinations were assessed with the following measures: peripheral and axial joint assessment (sacroiliac joints, axial mobility tests, and chest expansion), evaluation of extraarticular features such as nail lesions (pits and onycholysis), dactylitis, enthesitis, distal interphalangeal joint involvement, tenosynovitis, and psoriatic skin lesions. We determined swollen joint counts (SJC), tender joint counts (TJC), and duration of morning stiffness in minutes.
MRI protocol and data acquisition
MRI/gadolinium-enhanced MRI was done for all patients with unilateral or bilateral knee involvement. The results are given as per patient, to increase sensitivity. A General Electric echo speed 1.5-Tesla MR unit equipped with a dedicated cylindrical knee coil was used. Sagittal, coronal, and axial T1-weighted spin-echo MR images were obtained; detailed MR sequences and imaging characteristics are illustrated in Table 2. Immediately after the acquisition of baseline images, 0.05 mmol per kg/body weight intravenous bolus of Gd-DTPA (Schering, Berlin, Germany) was given including fat saturation.
Interpretation of MRI findings
MR images were evaluated for the following radiological signs before and after intravenous contrast injection: BME, bone erosions, cartilaginous erosions, synovial cyst, Baker’s cyst, periarticular soft tissue edema, knee effusion, and synovial thickness and distribution.
Joint effusion size was subjectively graded within the suprapatellar bursa, intercondylar region, and tibiofibular joint as follows: (1) mild, (2) moderate, and (3) large. Articular cartilage was assessed for contour (smooth vs irregular) and focal destruction (intact, superficial loss and/or thinning, or deep erosions to subchondral bone). Bone was assessed for marrow signal intensity abnormalities and focal erosions. Maximal synovium thickness was measured in the suprapatellar pouch on sagittal T1-weighted gadolinium-enhanced images, as in our earlier study9.
Special emphasis was given to the following entheseal sites and carefully evaluated for abnormalities: the quadriceps tendon insertion and the proximal and distal patellar tendon. The iliotibial band insertion, the MCL origin and insertion, the LCL origin and insertion, the lateral capsular insertions, the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL) origins and insertions, the biceps femoris insertion, the semimembranosus insertion, medial patellofemoral ligament (MPFL), and lateral patellofemoral ligament (LPFL). Focal areas of abnormal signal adjacent to the superior and inferior attachments of the posterior capsule and related calf muscle origins were also considered as enthesitis. Two observers, blinded to the patient’s diagnosis and status as patients or controls, interpreted all MRI scans. In cases of differing interpretations the findings were discussed until agreement was reached. This method was chosen to prevent interreader differences11.
Ophthalmological examination in all patients included (1) unaided and best-corrected visual acuity; (2) intraocular pressure assessment; (3) anterior segment evaluation with slit lamp; and (4) fundus examination with indirect ophthalmoscopy and biomicroscopy and (5) Schirmer’s tear test to exclude dry eyes.
The study was approved by the local ethical committee of the Dr. Erfan and Bagedo General Hospital and performed following the principles of the Declaration of Helsinki; all patients gave informed written consent before participation.
Statistical analysis
Quantitative variables were described using mean ± standard deviation (SD) and categorical data by frequency and percentage. Pearson chi-square test was used to test differences among categorical variables among the groups of patients and nonparametric Kruskal-Wallis test was used to compare quantitative variables among the groups. Fisher’s exact test was used to calculate an exact probability value for the relationship between 2 dichotomous variables between positive and negative patients with respect to enthesitis, and Student’s t test was used to compare quantitative variables between groups of patients with respect to enthesitis. In all tests, p value < 0.05 was considered to be statistically significant.
RESULTS
Detailed demographic and clinical characteristics of the study groups, slit lamp examination findings, and current treatment at inclusion in the study are illustrated in Table 1. The control group comprised 20 healthy subjects with no knee complaints and matched for age and sex with the patient group. They were 12 (60%) men and 8 (40%) women, mean age 34.30 ± SD 6.22 years.
Clinical and demographic characteristics of the studied groups of patients. Data are the mean ± SD unless otherwise indicated.
Laboratory results and characteristic MRI findings of patients are summarized in Table 2. Unilateral MRI studies were performed in a total of 11 patients and bilateral in the other 45 patients. Soft tissue edema was observed in 70% in the PsA group, 20% in the AS group, 40% in those with ReA, 20% with UC, 20% with Crohn’s disease, and in 20% with skin psoriasis (Table 2).
Laboratory investigations and detailed MRI findings among the studied groups of patients. Data are the mean ± SD unless otherwise indicated.
Comparison of quantitative variables among the groups of patients by nonparametric Kruskal-Wallis test showed no significant difference regarding sex (p = 0.8) and age at disease onset (p = 0.5). A higher significant difference was observed in the PsA group compared to other groups regarding disease duration (p = 0.02), ESR (p < 0.001), C-reactive protein (CRP) levels (p = 0.001), SJC (p < 0.001), TJC (p < 0.001), and degree of synovial thickness (p < 0.001).
Bone erosions were observed in 23.3% of the PsA group, 20% of the AS group, and 40% with ReA; and no erosions were observed in patients with UC, Crohn’s disease, or skin psoriasis.
Cartilaginous erosions were found in 40% with PsA, 20% with AS, 60% with ReA, and in 40% with UC, and none were observed among patients with Crohn’s disease and skin psoriasis.
BME was observed in 26.7% with PsA, 40% with AS, 40% with ReA, and 16.7% with skin psoriasis, while BME was totally absent in patients with UC or Crohn’s disease.
Enthesopathy
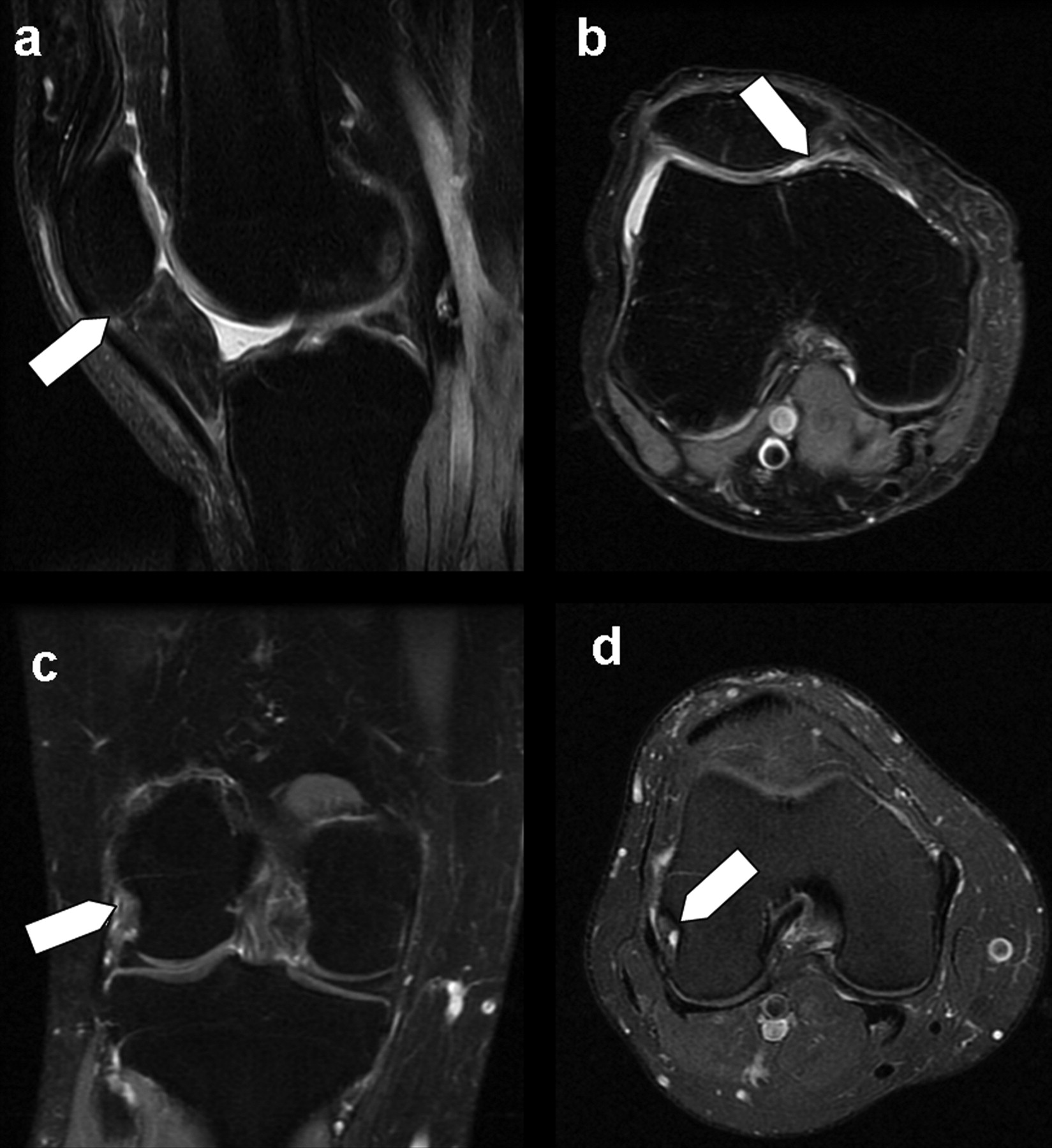
Enthesopathy of MCL was observed in 40% of PsA patients (Figure 1D), LCL in 16.7%, patellar tendon insertion in 23.3% (Figure 1A), PCL in 6.7% (Figure 1B), biceps femoris insertion in 10% (Figure 1C), MPFL in 6.7%, and LPFL in 3.3%, and none showed enthesopathy of the ACL.

Psoriatic arthritis: A (sagittal) and B (coronal) STIR sequence images show enhancement close to the tibial insertion of posterior cruciate ligament (PCL), with periligamentous high signal intensity compatible with fluid, moderate knee effusion, and focal bone marrow edema at the tibial insertion of the PCL (black arrow). C (sagittal) and D (axial) postcontrast T1 fat saturated images show enhancement at entheseal sites close to PCL and MCL and femoral insertions of biceps femoris tendon.
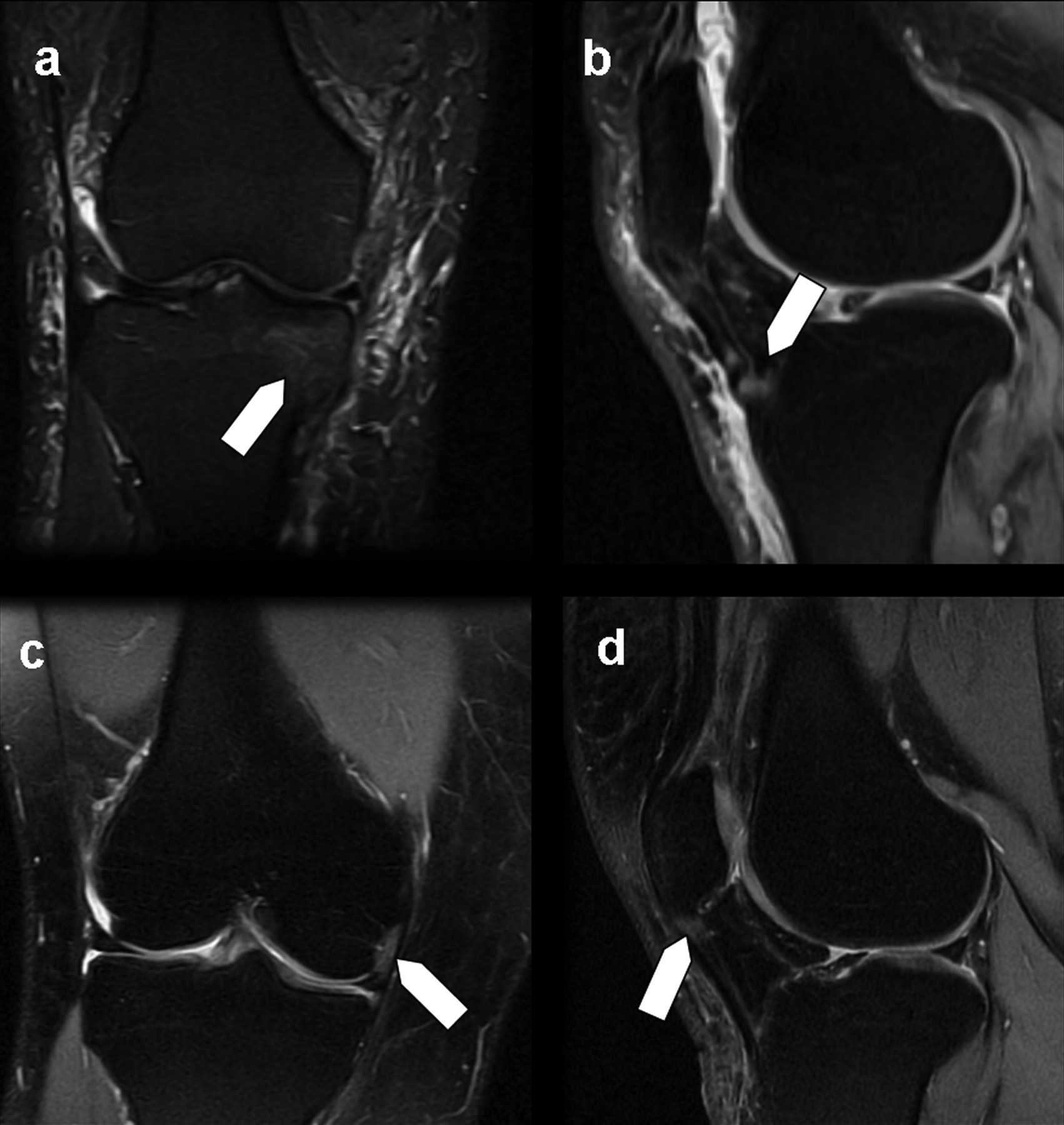
Enthesitis of the MCL was observed in 40% of the AS group, LCL in 40% and MPFL in 20%, and patellar tendon insertion in 20% (Figure 2A), while other entheseal sites were unaffected in this group.

Ankylosing spondylitis: A. Right knee PD fat saturated image shows enthesitis at the patellar tendon insertion (white arrow). Ulcerative colitis: B. Axial PD fat saturated image shows enthesitis at the medial patellar retinaculum (white arrow). Crohn’s disease: C (coronal) and D (axial) PD fat saturated images show enthesitis at the lateral collateral ligament of the right knee in the same patient (white arrows).
Enthesitis of the MCL was observed in 40% of the ReA group, PCL in 20%, and patellar tendon insertion in 60%, while other entheseal sites were unaffected in this group.
Enthesitis at the MCL was detected in 20% of the UC group, MPFL in 20% (Figure 2B), and patellar tendon insertion in another patient (20%), while in the Crohn’s disease group enthesitis was detected in the MCL in 20%, in LCL in 20% (Figure 2C, 2D), and in MPFL in 20%.
In the group with skin psoriasis (Figure 3), 83.3% showed enthesitis at patellar tendon insertion (Figure 3B, 3D) and 16.7% showed enthesitis at MPFL (Figure 3C), while other entheseal sites assessed by MRI were unaffected in this group (Table 2).

Skin psoriasis: A. Right knee coronal PD fat saturated image shows bone marrow edema (white arrow). B. Sagittal PD fat saturated image shows soft tissue edema and enthesitis at the patellar tendon insertion (white arrow) in another patient with skin psoriasis. C. Right knee coronal PD fat saturated image shows enthesitis at the medial patellofemoral ligament (white arrow). D. Right knee sagittal PD fat saturated image shows coexisting enthesitis in the same knee at the patellar tendon.
Pearson’s chi-square test showed no significant sex difference among the studied groups of patients (p = 0.23). For MRI findings, effusion size was significantly higher in the PsA group compared to other groups (p = 0.05). No other significant differences were observed between the groups of patients regarding Baker’s cyst (p = 0.6), soft tissue edema (p = 0.7), BME (p = 0.22), cartilaginous erosions (p = 0.23), bone erosions (p = 0.46), and enthesitis (p = 0.72).
Fisher’s exact test showed no significant association between enthesitis and sex distribution among the groups of patients. No significant association was observed between enthesitis and other MRI findings such as Baker’s cyst (p = 1), effusion size (p = 0.5), soft tissue edema (p = 1.0), BME (p = 0.09), cartilaginous erosions (p = 0.3), bone erosions (p = 0.3), and spinal disease (p = 0.6).
Student t test showed no significant associations between enthesitis and other categorical variables: age (p = 0.3), disease duration (p = 0.2), ESR (p = 0.07), CRP levels (p = 0.41), degree of synovial thickening (p = 0.84), SJC (p = 0.4), and TJC (p = 0.4).
No entheseal changes, bone erosions, or BME were found in the control group.
DISCUSSION
We evaluated enhanced MRI features and characteristic entheseal-related changes of the knee joint in 56 patients with SpA. Our report is the first to describe such changes in different diseases as representative of this domain, and the first to describe enthesitis of the knee joint among patients with inflammatory bowel disease and skin psoriasis by using MRI.
In 6 patients with skin psoriasis only, our study revealed evidence of subclinical arthritis in a large proportion. We also found entheseal-related changes among patients with skin psoriasis, where 5 out of 6 patients (83.3%) had enthesitis: soft tissue edema in 2 patients (33.3%) and BME in one patient (16.7%). These findings suggest that in patients with skin psoriasis a form of subclinical synovitis may exist, and the presence of entheseal-related changes in such a large percentage may suggest that enthesitis may be an early MRI sign (perhaps the earliest) of inflammation. This needs to be evaluated further in prognostic longitudinal studies.
Our patients with skin psoriasis are receiving only topical treatment and none was treated with disease modifying antirheumatic drugs like methotrexate that may delay or ameliorate the appearance of overt arthritis in patients presenting with skin psoriasis.
Our findings of subclinical synovitis in the knee joints are consistent with and extend the findings of Offidani, et al12, who performed MRI of the hands in 25 patients with skin psoriasis with no arthritic symptoms and controls. Signs of arthritis were found in 68% of patients including joint or tendon sheath effusions, bone erosions, and BME. Periarticular edema and synovitis/intraarticular effusion were the 2 most frequent findings (in 36% and 44%, respectively); these findings were in agreement with a scintigraphic study in patients with severe psoriatic skin disease13, with increased periarticular uptake of isotope at a number of joint regions. An early Mayo Clinic study14 noted subclinical PsA occurring in 39% of patients with skin psoriasis.
A novel finding in our study was the presence of entheseal-related changes of the knee joint among patients with inflammatory bowel disease — in patients with UC (n = 5) and Crohn’s disease (n = 5). In the UC group we observed cartilaginous erosions in 2 patients (40%) and soft tissue edema in one patient (20%); the latter finding was also observed in one patient with Crohn’s disease, while in the UC group no BME or bone erosions were found. These findings again suggest the presence of a subclinical synovitis among patients with inflammatory bowel disease despite treatment with combinations of mesalamine, corticosteroids, and azathioprine, which are effective in the treatment of arthritis. The coexistence of enthesitis in the patients with UC (MCL, n = 1; MPFL, n = 1; patellar tendon insertion, n = 1) and with Crohn’s disease (MCL, n = 1; LCL, n = 1; MPFL, n = 1) suggests again that enthesitis is a characteristic MRI finding in these patients and may be an early sign of inflammation in patients with inflammatory bowel disease.
Psoriatic arthritis
In our series the PsA patients often, but not always, showed a pattern of joint inflammation that extended beyond the capsule into the extraarticular tissue. In particular, bone edema at the entheseal junction was seen, especially in the knee. MRI allows visualization of soft tissue articular and entheseal lesions, and provides a unique picture of the disease process that cannot be achieved using other imaging modalities. An enthesis-related origin of PsA has been proposed in contrast to the primarily synovial inflammation of RA15.
We observed that in the 30 patients with PsA, there was enthesitis of the MCL (n = 12), LCL (n = 5), patellar tendon insertion (n = 7), PCL (n = 2), biceps femoris insertion (n = 3), MPFL (n = 2), and LPFL (n = 1), and none showed enthesopathy of ACL.
Inflammation at the entheses, the sites of attachment of tendon, ligament, fascia, or joint capsule to bone, is a distinguishing pathological feature of the SpA, including PsA16. Oriente, et al17 found peripheral enthesitis in 20% of patients with PsA, with a peak value of 30% in those with spondylitic pattern, and a subset of psoriatic arthritis may present with isolated enthesitis and/or dactylitis18. In the hand joints, McGonagle and colleagues hypothesized that enthesitis is the primary lesion in SpA and that synovitis of the various structures (joint, tendon, and bursa) represents a secondary phenomenon due to the release of proinflammatory cytokines from the inflamed entheses19,20. In their opinion, the flexor tenosynovitis of dactylitis is due to enthesitis as a consequence of the diffusion of cytokines along the tenosynovial sheaths20. In contrast, Olivieri, et al21 demonstrated that in SpA dactylitis there is no evidence of enthesitis of the insertion of the flexor digitorum tendons or of the attachment of the capsule of the digit joints. In another study, McGonagle, et al22 suggested that dactylitis-enthesitis complex could occur at the numerous “functional entheses” that the digit flexor tendons form with retinacula or pulleys. These functional entheses are frequently associated with the presence of fibrocartilage that reduces compression and shear. Considering these together, enthesitis could be the common thread that confirms PsA as a distinct entity from RA and also unifies the clinical subsets of PsA.
McGonagle, et al introduced the concept of the “synovio-entheseal complex”23,24,25,26. This opens previously unexplored avenues of research in PsA, focusing attention away from the synovial cavity, and could advance our understanding of the disease pathogenesis27. Peripheral PsA synovitis appears similar to RA synovitis on static and dynamic MRI; however, bone erosions in PsA do not have disease-specific MRI features and little is known of how they progress over time. With enthesitis, dactylitis, and spondylitis, the MRI features of PsA depart from those of RA and conform to the SpA group of disorders28. Further, on the histopathological level the inflamed synovial membrane of PsA differs in subtle ways from rheumatoid synovium, with less lining-layer hyperplasia, more subsynovial edema, and a greater number of synovial vessels per square millimeter29.
McGonagle, et al1 used fat-suppressed MRI to evaluate entheseal-related changes involving the knee joint in patients with RA (n = 10) and SpA (n = 10) to determine if the primary site of abnormality differs. They observed that all 10 SpA patients, but only 4 of 10 RA patients, had focal perientheseal high signal (compatible with fluid or edema) outside the joint (p = 0.01). In their study 6 SpA patients had BME that was maximal at entheseal insertions; in 4 cases this was multifocal and no patient with RA showed such an abnormality (p = 0.01). The authors concluded that prominent entheseal abnormalities on MRI are a consistent feature of new-onset synovitis in SpA, but are a minor feature of RA1. In their study there were 2 significant findings: (1) Focal soft tissue edema outside the joint capsule adjacent to entheseal insertions (perientheseal fluid/edema) was common, and was probably secondary to enthesitis, while the soft tissue abnormalities outside the joint that were seen in a subset of RA patients may have been secondary to severe synovitis, with nonspecific extension of the inflammatory process beyond the joint capsule. (2) BME that was maximal adjacent to entheseal insertions was seen only in SpA and was accompanied by perientheseal fluid or edema. This pattern of bone edema in their study was previously reported in relation to peripheral enthesitis and spondylitis, which suggests a common pathogenic link between spinal disease, peripheral enthesitis, and knee synovitis in SpA. The same group also studied calcaneal enthesopathy in 17 patients with early SpA (including 4 with PsA), and similar findings were described, again often including underlying BME30.
The role of MRI in differentiating undifferentiated arthritis remains debatable and some attempts have incorporated anatomic information. Small studies have shown that MRI signs of inflammation in RA are more frequent in the synovial membrane than at the insertions of ligaments and tendons (enthesitis), while the opposite is true for SpA such as PsA and ReA3. Recently, we compared enhanced MRI features of knee joints in 3 groups of patients: oligoarticular undifferentiated arthritis (UA; n = 25), established RA (n = 15), and SpA (n = 15)9. We observed enthesitis in all SpA groups, significantly more than in the other 2 groups (RA and UA; p < 0.001). Enthesitis with anatomical localization by MRI in the SpA group showed involvement of fibular collateral ligament (n = 1) and fibular insertion of biceps femoris (n = 2), PCL (n = 4), MCL (n = 7), and patellar tendon insertion (n = 5); whereas in the undifferentiated group, enthesitis of MCL was observed in 3 patients and no RA patient showed enthesitis. We suggested that enthesitis on MRI is a common feature in SpA involving the knee joint, but totally absent in the RA group. This latter finding may have clinical implications for classification purposes, and can help to determine the evolving pattern of patients with UA of the knee joint9.
A strength of our study is that we investigated the knees in a large cohort of patients and controls. Moreover we identified more entheseal sites by MRI in the knee joint that can be potentially involved and have not previously been reported in SpA, i.e., the medial and lateral patellofemoral ligaments.
Most studies to date3,4,5,6,7,8 examined and compared characteristic MRI features of the hand joints in RA versus SpA, and only 2 studies1,9 described entheseal-related changes in the knee among patients with RA versus SpA. Our study is the first to describe entheseal-related changes among the whole group of SpA including PsA, AS, and ReA, as well as in those with inflammatory bowel diseases such as UC and Crohn’s disease and even in patients with psoriatic skin lesions without clinical evidence of synovitis.
In summary, entheseal-related changes can be found in patients with inflammatory bowel disease or skin psoriasis with no clinical enthesitis or arthritis. Enthesitis of the knee joint may be an early (perhaps the first) sign on MRI and a characteristic finding in the SpA group of diseases. Entheseal-related changes in SpA can be accompanied by other MRI signs suggestive of ongoing inflammation, such as soft tissue edema, BME, or cartilaginous or bone erosions, that suggest a possible relation to the disease process in this domain (SpA). However, on examination these changes often remain undetected.
Further prospective studies in larger populations of patients are needed to examine the incidence and influence of entheseal-related changes of the knee joint shown by MRI; findings could have important implications for understanding the mechanistic pathways of disease pathogenesis.
- Accepted for publication March 3, 2010.








{kind=link}
{kind=link}
{kind=link}