

Abstract
Since the first report of serum IgG4 elevation in sclerosing pancreatitis in 2001, various systemic disorders have been reported to elevate IgG4, and many names have been proposed from the perspective of the systemic condition. Despite similarities in the organs damaged in IgG4-related Mikulicz’s disease and Sjögren’s syndrome, there are marked clinical and pathological differences between the 2 entities. The majority of cases diagnosed with autoimmune pancreatitis in Japan are IgG4-related sclerosing pancreatitis, and it should be recognized that this is distinct from the Western type. Diagnosis of IgG4-related disease is defined by both elevated serum IgG4 (> 1.35 g/l) and histopathological features, including lymphocyte and IgG4+ plasma cell infiltration (IgG4+ plasma cells/IgG+ plasma cells > 50% on a highly magnified slide checked at 5 points). Differential diagnosis from other distinct disorders is necessary: these include sarcoidosis, Castleman’s disease, Wegener’s granulomatosis, lymphoma, cancer, and other existing conditions. The Japanese IgG4 research group has begun multicenter prospective studies to improve diagnostic criteria and treatment strategies.
Mikulicz’s disease (MD) was first described in 1892 in a man with symmetrical swelling of the lacrimal, submandibular, and parotid glands1. Morgan, et al reported 18 cases of MD and concluded that it was not a distinct clinical and pathological disease entity but merely one manifestation of a more generalized symptom complex known as Sjögren’s syndrome (SS)2. With the wide acceptance of the conclusions of Morgan, et al there have been few reports of MD in Western countries. However, many cases of MD have been reported in Japan, and there has been considerable discussion regarding the differences between MD and SS3–7. Patients with MD have been reported to have a point mutation in the FasL gene, which may account for their mild sicca symptoms despite massive lymphocytic infiltration3. Further, high IgG4 concentrations have been reported in the sera of patients with MD4, suggesting that MD is an IgG4-related disease.
We describe the differences between MD (especially IgG4-related MD) and SS, and refer to other systemic complications of IgG4-related diseases.
Differences between IgG4+ MOLPS and SS
As so-called MD may include various conditions3–6 and consist of IgG4-related or unrelated subtypes, the IgG4+ multiorgan lymphoproliferative syndrome (MOLPS)/MD research group has established tentative criteria for IgG4+ MD (Table 1).
Diagnostic criteria of IgG4+ Mikulicz’s disease (Japanese Sjögren’s Syndrome Society, 2008). Differential diagnosis is necessary from other distinct disorders, including sarcoidosis, Castleman’s disease, Wegener’s granulomatosis, lymphoma, and cancer. The diagnostic criteria for Sjögren’s syndrome (SS) may also include some patients with IgG4+ Mikulicz’s disease; however, the clinicopathological conditions of patients with typical SS and IgG4+ Mikulicz’s disease are different.
MATERIALS AND METHODS
We collected data on 64 patients with IgG4+ MOLPS including MD and performed retrospective analysis to clarify the differences between IgG4+ MOLPS and definite SS (Table 2)7. Despite similarities in the involved organs, there are marked differences between IgG4+ MOLPS and SS. For example, their sex distributions were quite different. Men with SS were very rare (2 of 31), while almost half (31 of 64) the patients with IgG4+ MOLPS were men.
Comparison of symptoms, complaints, and laboratory findings in IgG4+ MOLPS and typical SS. Data are percentage (number) unless stated otherwise. Incidence rates (numbers of positive patients) are shown for xerophthalmia, xerostomia, arthralgia, allergic rhinitis, bronchial asthma, sclerosing pancreatitis, interstitial nephritis, interstitial pneumonitis, RF, ANA, A-SSA, A-SSB, and low CH50. Masaki Y, et al7. Ann Rheum Dis 2009; 68:1310–5. Adapted with permission.
RESULTS
Significantly fewer patients with IgG4+ MOLPS than with SS showed symptoms of xerostomia, xerophthalmia, and arthralgia. Patients with IgG4+ MOLPS showed significantly lower incidences of rheumatoid factor (RF), antinuclear antibody (ANA), anti-SSA/Ro antibody, and anti-SSB/La antibody than patients with SS. We found that not only IgG4 but also total IgG, IgG2, and IgE concentrations were significantly higher in patients with IgG4+ MOLPS than in patients with SS7. Almost half of patients with IgG4+ MOLPS demonstrated low CH50, which apparently correlated with hyper-IgG (especially IgG1 and IgG2).
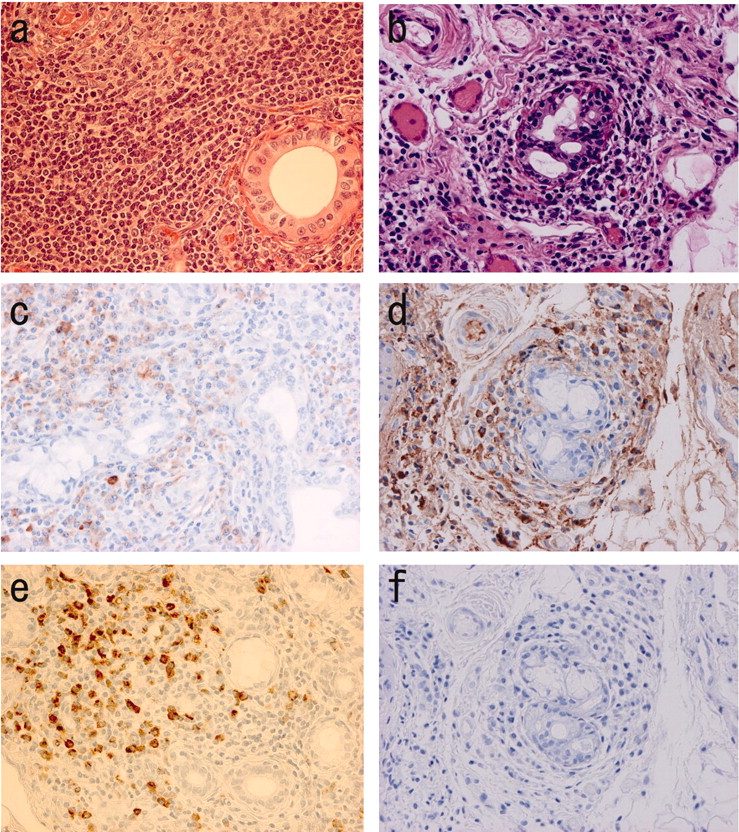
Histological specimens from patients with IgG4+MOLPS showed marked IgG4+ plasma cell infiltration with occasional lymphocyte follicular formation, but without lymphoepithelial lesions (Figure 1)7. This may explain the marked glandular swelling without severe dryness in patients with IgG4+ MOLPS. Importantly, treatment with glucocorticoids resulted in marked clinical improvements in almost all patients with IgG4+ MOLPS, while the effects of glucocorticoids on SS were not so dramatic10.

Histopathological findings of labial minor salivary gland biopsy in patients with IgG4+ MOLPS/Mikulicz’s disease (a, c, e) and Sjögren’s syndrome (b, d, f). (a, b) Hematoxylin and eosin staining; (c, d) IgG immunostaining; (e, f) IgG4 immunostaining. (a) Massive lymphocyte and plasmacyte infiltration and lymphoid follicle formation were seen in IgG4+ MOLPS. The ducts remained clear without lymphocytic infiltration. Both IgG+ and IgG4+ plasma cells were scattered in the periphery of the follicles (c, e). In contrast, there were few or no IgG4+ cells in typical SS (d, f), not even in patients with severe lymphocytic infiltration (b).
Autoimmune pancreatitis and IgG4
Autoimmune pancreatitis (AIP) is a unique form of chronic pancreatitis, first described by Sarles, et al in 196111 and characterized by infrequent attacks of abdominal pain, jaundice, irregular narrowing of the pancreatic duct, and swelling of the pancreatic parenchyma11–22. Kawaguchi, et al described cases complicated with similar pathological features in the common bile duct, gall bladder, and minor salivary glands, suggesting a systemic disorder12. Yoshida, et al described the typical features of AIP as hyper-γ-globulinemia, the presence of autoantibodies (RF and ANA), lymphocytic infiltration of pancreas tissue, coexistence of other manifestations such as sicca complex, and good responsiveness to glucocorticoids13. AIP is now known to be associated with types of sialadenitis and cholangitis distinct from SS and primary sclerosing cholangitis.
In 2001, Hamano, et al first reported high serum IgG4 concentrations in patients with sclerosing pancreatitis14. Further, massive IgG4+ plasmacytic infiltration in the pancreatic tissue was reported15. There have been many recent reports of AIP in Asia12–19 and in Western countries20,21.
Various diagnostic criteria for AIP have been proposed in Japan23, Korea17, and the United States (Mayo Clinic)21. In 2008, the Japan-Korea Symposium on AIP proposed Asian diagnostic criteria19. Further international criteria are currently under discussion.
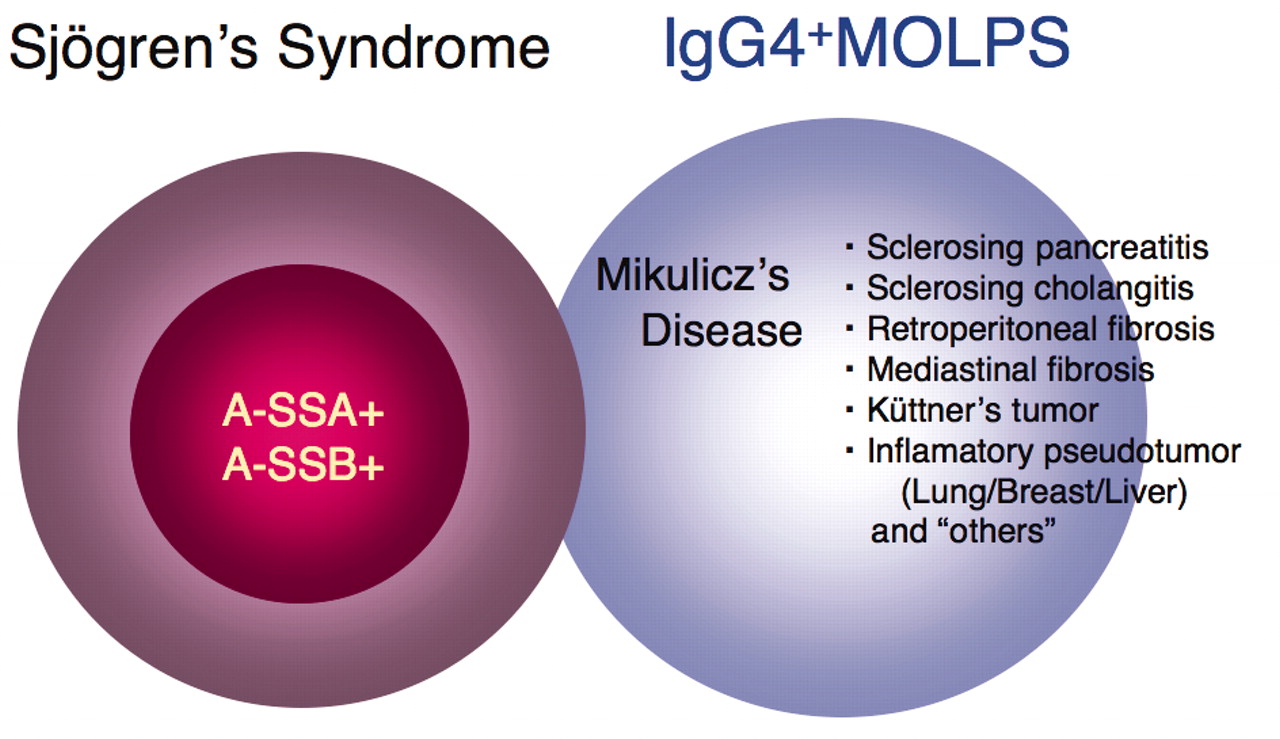
IgG4 and other clinical conditions (Figure 2)

IgG4+ MOLPS should be defined as a distinct clinicopathological entity that includes Mikulicz’s disease (MD), autoimmune pancreatitis (AIP), sclerosing cholangitis, and other clinical conditions with good response to glucocorticoids. Although the diagnostic criteria of SS may include some patients with IgG4+ MOLPS/MD, typical SS and IgG4+ MOLPS/MD are different clinical conditions.
Hyper-IgG4-γ-globulinemia and IgG4+ plasma cell infiltration with sclerotic lesions, although first reported in patients with sclerosing pancreatitis, have also been reported in patients with many other disorders, including sclerosing cholangitis15,16; inflammatory pseudotumors of the lung24, liver16, and breast16,25; retroperitoneal or mediastinal fibrosis26; interstitial nephritis27; hypophysitis5; sclerosing dacryoadenitis28; sialadenitis (MD and Küttner’s tumor)4,5,29; inflammatory aortic aneurysm30,31; tumorous lesions of the coronary artery31; lymphadenopathy32; and many other inflammatory conditions in multiple organs.
In addition, various systemic involvements have been reported in each disorder. Kawaguchi, et al12 noted the same etiology between autoimmune pancreatitis and multifocal idiopathic fibrosclerosis (MIF) reported by Comings, et al33 because both conditions include occlusive phlebitis and sclerotic lesions.
DISCUSSION
Proposal of a new clinical entity, IgG4+ MOLPS, as a more generalized disorder
In addition to the term “IgG4+ MOLPS,” there are many synonyms, such as MIF, IgG4-related autoimmune disease15, IgG4-related plasmacytic disease6, and IgG4-related sclerosing disease18, all of which may refer to the same conditions.
Although various other disorders have been associated with hyper-IgG4-γ-globulinemia, including multicentric Castleman’s disease34, Wegener’s granulomatosis35, lymphoma36,37, and cancer38, IgG4+ MOLPS should be defined as a distinct clinicopathological entity, characterized by sclerosing sialadenitis and dacryoadenitis, AIP, sclerosing cholangitis, and other clinical conditions with good response to glucocorticoids.
Hypothetical mechanism of IgG4+ MOLPS
At present, the pathogenesis of IgG4+ MOLPS is not clear. Although some patients are positive for RF and ANA, these incidences are significantly lower than in SS, suggesting that RF and ANA positivity may be due to nonspecific immunoglobulin binding. Although IgG4+ MOLPS is accompanied by various immunological disorders, including AIP, there is little evidence that IgG4+ MOLPS is an autoimmune disorder because of the lack of disease-specific autoantibodies.
The role of IgG4 in IgG4+ MOLPS is still unknown. IgG4 represents the smallest population among IgG subclasses in the sera of normal subjects (3%–6% of total IgG), and is unique among the IgG subclasses in its inability to bind with the C1q complement39. IgG4 is associated with the pathogenicity of a small number of disorders, such as atopic dermatitis, parasitic disease, pemphigus vulgaris, and pemphigus foliaceus.
In clonality analysis, most tissue-infiltrating and circulating IgG4-positive cells are polyclonal40. These findings have suggested that IgG4 does not play a major pathological role in IgG4+ MOLPS, and that there may be other upstream regulators in its pathogenesis.
Zen, et al reported that the pathogenesis of IgG4-related AIP was characterized by the infiltration of T helper 2 and regulatory T cells (Treg), which secrete various cytokines such as interleukin 10 (IL-10) and tumor growth factor-ß (TGF-ß)41. Moreover, the level of Foxp3 messenger RNA expression was significantly increased in patients with AIP, and immunohistochemical staining revealed increases in the numbers of CD4+ CD25+ Foxp3+ cells. Treg may be involved in the in situ production of IL-10 and TGF-ß, which could be followed by IgG4 class switching and fibroplasia41.
The concentrations of IgG2, IgG4, and IgE have been shown to be significantly higher in patients with IgG4+ MOLPS than in those with typical SS, while the concentrations of IgG1, IgG3, IgA, and IgM were significantly higher in patients with typical SS than in those with IgG4+ MOLPS7. The immunoglobulin gene fragments Cμ, Cδ, Cγ3, Cγ1, Cα1, Cγ2, Cγ4, Cɛ, and Cα2, which encode IgM, IgD, IgG3, IgG1, IgA1, IgG2, IgG4, IgE, and IgA2, respectively, are arranged linearly in this order from upstream to downstream. Gene linkage and different class-switch mechanisms may cause the hyperproduction of the different immunoglobulin subclasses observed in these 2 diseases, which may contribute to the pathophysiology of IgG4+ MOLPS.
Future perspectives
Although IgG4+ MOLPS may be distributed worldwide, this disease entity has not been well recognized to date. Most reports on IgG4-related diseases have been from Japan, while many reports on AIP have come from Western countries, especially the Mayo Clinic21 in the United States. Therefore, we believe that an international consensus regarding IgG4-related diseases as new clinical entities is required.
In this regard, the Japanese IgG4 research group (Research Committee of Intractable Diseases, Health and Labor Sciences Research Grants, Ministry of Health, Labor and Welfare, Japan) has begun multicenter prospective clinical studies (UMIN: R000002820, R000002823) to formulate better diagnostic criteria, to identify novel diagnostic and prognostic factors, and to design better treatment strategies.
Acknowledgments
We thank all participants in the IgG4+ MOLPS/Mikulicz’s Disease Research Group and the researchers of the Autoimmune Pancreatitis Group for critical discussion.
Footnotes
-
Supported by grants from Intractable Diseases, the Health and Labor Sciences Research Grants from the Ministry of Health, Labor, and Welfare, and the Japanese Ministry of Education, Culture, Sports, Science, and Technology (13557160, 15024236, 15390313, and 13877075 to H. Umehara and 17591060 to Y. Masaki), Umehara Memorial Foundation (to H. Umehara), The Vehicle Racing Commemorative Foundation, and the Kanazawa Medical University Research Foundation (C2009-4 to H. Umehara and S2004-16 and S2007-5 to Y. Masaki).
- Accepted for publication February 8, 2010.








{kind=link}
{kind=link}