

Abstract
Objective. To ascertain whether magnetic resonance angiography (MRA) can reliably detect synovial neovascularization in subjects with early inflammatory arthritis.
Methods. Subjects with 6 weeks to 6 months of clinical evidence of inflammatory hand arthritis had a radiograph, power Doppler ultrasound (PDU) scan, magnetic resonance imaging (MRI), and contrast enhanced MRA performed on the more symptomatic hand. Ultrasound examination of the wrist and 2nd–5th metacarpophalangeal (MCP) joints was scored for erosions, synovial thickening, and synovial blood flow. MRI were assessed using the OMERACT Rheumatoid Arthritis MRI Score (RAMRIS). MRA was used to assess the number of abnormal vessels in the 2nd–5th MCP and in the wrist.
Results. Of 30 subjects, 66.7% showed abnormal vasculature on MRA in the MCP and/or wrist; mean number of abnormal vessels was 5.24 (range 0–22). Number of abnormal vessels on MRA was strongly correlated with degree of blood flow seen in the corresponding area on PDU (r = 0.79, p ≤ 0.0001). The number of abnormal vessels was highly correlated with MRI MCP synovitis scores (r = 0.69, p ≤ 0.0001), MRI wrist synovitis scores (r = 0.73, p ≤ 0.0001), and ultrasound synovitis scores (r = 0.68, p ≤ 0.0001).
Conclusion. In this cross-sectional pilot study, MRA identified abnormal vessels in patients with early inflammatory arthritis. This is the first report of MRA visualizing abnormal vessels in this patient population. If the degree of neovascularization in early inflammatory arthritis predicts disease course, MRA evidence of abnormal vessels could be a new imaging biomarker.
- EARLY INFLAMMATORY ARTHRITIS
- IMAGING
- VASCULARITY
- MAGNETIC RESONANCE ANGIOGRAPHY
- POWER DOPPLER ULTRASOUND
Determining which patients with recent onset undifferentiated inflammatory arthritis will develop rheumatoid arthritis (RA) remains a challenge for rheumatologists. Many patients with recent-onset inflammatory arthritis do not have a full spectrum of signs and symptoms and usually have normal radiographic findings1. Given the ability of disease-modifying antirheumatic drugs (DMARD) and biologics to prevent permanent damage2, it is of importance to identify those individuals with early inflammatory arthritis who are at high risk of future erosive disease so that they can be treated aggressively, before the occurrence of irreversible joint damage. A reliable method to stratify patients for risk would allow directed treatment of those who are most likely to progress, while preventing drug-related side effects in those with less aggressive disease.
Synovial angiogenesis has been proposed as one of the earliest markers of inflammatory arthritis3. Angiogenic cytokines, such as platelet-derived growth factor, tumor necrosis factor-α, and vascular endothelial growth factor (VEGF), which also mediates changes in synovial permeability, are present in the synovial fluid and synovium of RA patients with active disease4,5. In the rat model of collagen-induced arthritis (CIA), angiogenesis inhibitors prevent the onset of CIA, suppress established disease, and reduce serum concentrations of VEGF3. Investigators postulate that the degree of synovial vascular proliferation may determine the rate of disease progression in RA, as described in diabetic retinopathy6. It is not known, however, if the presence of synovial vascular proliferation in early undifferentiated inflammatory arthritis predicts development of established RA. This hypothesis would ideally be tested by prospective histologic evaluation of synovium. However, this is not ethically feasible. In place of tissue sampling, a noninvasive “imaging biomarker” that could reliably identify abnormal vessels would allow this to be determined. We evaluated the capability of magnetic resonance angiography (MRA) to identify abnormal vasculature in patients with very early inflammatory arthritis, and correlated the findings on MRA with other measures of disease activity.
MATERIALS AND METHODS
Design
This cross-sectional pilot study was designed to evaluate whether MRA can detect abnormal capsular vessels in the wrists and metacarpophalangeal (MCP) joints of subjects with very early inflammatory arthritis of the hands. The study protocol was approved by the Hospital for Special Surgery, Weill Cornell Medical College, and General Clinical Research Center of Weill Cornell Medical College institutional review boards. All patients provided written informed consent.
Participants
Thirty patients with signs and symptoms of hand inflammatory arthritis for at least 6 weeks but less than 6 months were recruited between August 2005 and October 2006 from the private offices of rheumatologists affiliated with Hospital for Special Surgery, New York. Subjects were between ages 18 and 75 years, and had at least 3/7 criteria for RA of the 1987 American College of Rheumatology (ACR) revised criteria7. Exclusion criteria included another systemic rheumatic disease or crystalline arthritis, pregnancy or nursing, unable to give informed consent, current use of glucocorticoids, methotrexate or other DMARD except plaquenil, active malignancy (except non-melanomatous skin cancer), active cellulitis or osteomyelitis, contraindication to magnetic resonance imaging (MRI), known claustrophobia, gadolinium allergy, Raynaud’s phenomenon, and lack of fluency in English.
Clinical assessment
Clinical evaluation was performed for all patients by the same rheumatologist before the imaging studies were performed. Patients answered questionnaires about their demographic information, current medication use, and comorbid conditions, and completed the Multidisciplinary Health Assessment Questionnaire (MDHAQ).
Laboratory assessment
C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and serum antibodies for rheumatoid factor (RF) IgM and anti-cyclic citrullinated protein antibodies (anti-CCP) were determined at baseline. IgM RF was measured using nephelometry; RF > 20 was considered positive. Anti-CCP were detected using ELISA; anti-CCP antibody > 20 was considered positive.
Disease activity assessment
Disease activity was assessed by calculating the 28-joint Disease Activity Score (DAS28) for each patient8.
Ultrasound assessment
Ultrasound examinations of the wrist and second through fifth MCP joints of the more symptomatic hand were performed by an experienced musculoskeletal ultrasound radiologist, blinded to the clinical, laboratory, radiographic, and MRI findings. The ultrasound was performed utilizing an IU22 system (Phillips Medical, Bothell, WA, USA) with a 12 or 17 MHz transducer linear phased array. Power Doppler measurements were obtained using the scanner’s low-flow sensitivity settings according to the criteria given by Newman, et al9 with scans obtained in sagittal plane at 3 points through each MCP joint and at 3 standardized points along the carpus. Each ultrasound scan was scored for erosions and synovitis of the carpus and 2nd–5th MCP. Scores for erosions and synovitis were based on the scale for those measures used by Szkudlarek, et al10 in their study of ultrasonography of the finger and toe joints in RA. Erosions were scored 0–2 (0 = no erosions, 1 = single erosion, and 2 = multiple erosions) for the 2nd–5th MCP, base of the metacarpals 1–5, and carpus as divided into 3 areas (carpus, distal ulna, and distal radius) for a total erosion score ranging from 0 to 24. Synovial thickening was scored 0–3 (0 = no synovial thickening, 1 = minimal synovial thickening, 2 = synovial thickening bulging over the line linking tops of the periarticular bones but without extension along the bone diaphysis, 3 = synovial thickening bulging over linking tops of the periarticular bones and with extension to at least one of the bone diaphyses) for the dorsal and volar sides of the 2nd–5th MCP and the dorsal and volar sides of the wrist as divided into proximal radial, proximal ulnar, distal radial, and distal ulnar for a total synovial thickening score ranging from 0 to 48. Power Doppler ultrasound (PDU) was used to assess vascularity. Vascularity scores were designed to parallel the vascularity scoring for the MRA. Vascularity was scored 0–3 (0 = no appreciable synovial flow, 1 = mild synovial flow, 2 = moderate synovial flow, 3 = marked synovial flow) for the dorsal and volar sides of the 2nd–5th MCP and the dorsal and volar carpus divided into radial, mid, and ulnar zones, for a total vascularity score ranging from 0 to 21.
MRI/MRA assessment
All patients underwent noncontrast MR imaging as well as MRA following intravenous injection of 0.2 ml/kg gadolinium (Omniscan, General Electric Health Care, Milwaukee, WI, USA) of the more clinically active hand on the same day as their clinical evaluation. One patient was unable to complete the MRI due to severe shoulder pain. Twenty-six studies were performed on a 1.5 Tesla unit and 3 studies were performed on a 3.0 Tesla unit (General Electric Health Care). All studies were completed with a standard 8 channel phased array extremity coil placed at isocenter. Coronal and sagittal moderate echo time (34 ms) fast spin-echo images were obtained using a validated cartilage-sensitive technique11. Additional coronal fast inversion recovery techniques were performed to provide an extended dynamic range and allow visualization of subtle marrow edema, which has been shown to precede the presence of erosion12. All patients received a single intravenous Gd-DTPA injection for their time-resolved MRA as part of the standard study protocol, following the noncontrast enhanced MRI in 3 planes, inclusive of a coronal fat-suppressed sequence. A 3-dimensional, digitally subtracted, contrast-enhanced MRA was performed using a time-resolved sequence, typically between 8 and 10 s following intravenous administration of a contrast bolus at a rate of 2 cc/s [time-resolved imaging of contrast kinetics (TRICKS); General Electric Health Care]. Following the MRA, a T1-weighted fat-suppressed sequence was performed. The total time for a morphological MRI of the hand is roughly 40 min. The time-resolved MRA added an additional 5 min.
MRI and MRA were analyzed and scored independently by 2 experienced musculoskeletal MR radiologists without knowledge of the patients’ clinical, laboratory, or radiographic findings (radiographs or ultrasound). MRI were scored according to the OMERACT RAMRIS13,14 scoring system. The MR radiologists used the EULAR-OMERACT RA MRI Reference Image Atlases as a guide for scoring15,16.
Blood vessels on MRA are defined as tubular anatomical structures in the expected distribution of the known vascular anatomy, as well as its normal variants, which demonstrate vascular enhancement following administration of contrast. In the hand, the radial and ulnar arteries give rise to the deep and superficial palmar arches, which give rise to the digital vessels. In a normal hand, there are no discernible smaller arterial branches. New periarticular vessels are identified if there is enhancement of additional arterial supply derived from the normal arteries of the hand17. In our study, new periarticular vessels were identified both temporally and anatomically. The arteries are enhanced prior to venous contamination of the angiogram17. Rapid, successive imaging of the vessels starting 8 s after intravenous injection allowed clear delineation between arterial and venous structures. 3-dimensional assessment of the maximum intensity projection of the temporally subtracted angiogram also helped confirm the arterial origin of the new or recruited vessels.
The MRA were scored for discernible number of abnormal new vessels in the 2nd–5th MCP and carpus. The carpus was divided into 3 compartments: radiocarpal, distal radioulnar, and midcarpal. The MRA score was the sum of all discernible vessels in each area.
Radiographic assessment
Posteroanterior radiographs of patients’ hands were taken at the study visit unless the patient had hand radiographs performed at our hospital within the 6 weeks prior to the US/MRI/MRA evaluation. In those cases, the previous radiographs were used. The radiographs were read by an experienced musculoskeletal radiologist blinded to the patients’ clinical, laboratory, ultrasound, and MRI findings. Radiographic evidence of erosions and joint space narrowing was determined according to the Sharp-van der Heijde method18.
Statistical analysis
Statistical analysis was performed using SAS v. 9.1.3 (SAS, Cary, NC, USA). Correlations among clinical, laboratory, and imaging data were analyzed by Spearman’s rank correlation test. Rater agreement was assessed using the interclass correlation coefficient per Shrout and Fleiss19. The first set of results used the raw scores. A square-root transformation was used to obtain the second set of results. The purpose of the square-root transformation is variance stabilization.
RESULTS
Thirty patients were enrolled in the study. One ultrasound study could not be analyzed as the file was corrupted. One patient was unable to complete the MRI due to severe shoulder pain. One patient did not have analysis for RF, and one patient did not have anti-CCP antibodies drawn. One patient had a radiograph of only 1 hand. Available data from the 5 patients with incomplete data were analyzed.
The patients’ demographic and clinical details are shown in Table 1. The median duration of symptoms at entry into the study was 15.4 weeks. Sixty percent of patients met ACR criteria for RA, 38% were RF-positive, and 21% had anti-CCP antibodies. The median DAS28 was 3.6 [interquartile range (IQR) 1.67].
Demographic and clinical characteristics (n = 30).
Patients’ imaging characteristics are shown in Table 2. Forty-seven percent of subjects had erosions on radiographs. The median number of erosions on radiographs was 3.5; 55.1% of subjects had erosions by ultrasound, with a median number of 1 erosion. The median synovial thickening score was 6. The possible total synovial thickening score for the wrist and MCP ranged from 0 to 48. The median ultrasound vascularity score was 1. The possible total ultrasound vascularity score for the wrists and MCP ranged from 0 to 21. 66.7% of patients had erosions on MRI. The median RAMRIS score was 3 (IQR 5) for the MCP and 3 (IQR 6) for the wrist. The median RAMRIS bone edema score was 0 (IQR 0) for the MCP and 0 (IQR 1) for the wrist. On MRA, 66.7% showed abnormal vessels in the MCP and/or carpal compartments; the median number of new vessels was 4 (IQR 9).
Imaging characteristics (n = 30).
Spearman correlations are shown in Table 3. The number of abnormal vessels on MRA was strongly and significantly correlated with degree of blood flow seen on PDU (r = 0.79, p ≤ 0.0001) as well as RAMRIS synovitis scores of the MCP (r = 0.69, p ≤ 0.0001) and RAMRIS synovitis scores of the wrist (r = 0.73, p ≤ 0.0001), RAMRIS bone erosion score of the wrist (r = 0.78, p < 0.0001), RAMRIS bone edema score of the wrist (r = 0.43, p = 0.02), ultrasound synovitis scores (r = 0.68, p ≤ 0.0001), RF titer (r = 0.43, p = 0.02), and anti-CCP antibody titer (r = 0.43, p = 0.02). The number of abnormal vessels seen on MRA did not correlate with MHAQ, DAS28, or RAMRIS bone edema or bone erosion score of the MCP, or the ultrasound erosion score.
Spearman correlations.
There was a high degree of agreement between readers for the scoring of number of vessels seen on the MRA (Shrout-Fleiss ICC 0.91).
MRI and MRA in Figure 1⇔ show synovitis, tenosynovitis, and abnormal capsular vessels, and PDU shows increased vascularity in the wrist of a patient with clinical synovitis, positive serologies, and a DAS of 5.32. MRI and MRA in Figure 2 show no evidence of synovitis, tenosynovitis, or abnormal capsular vessels in the hand and wrist of a patient with minimal clinical synovitis, negative serologies, and a DAS of 2.61.
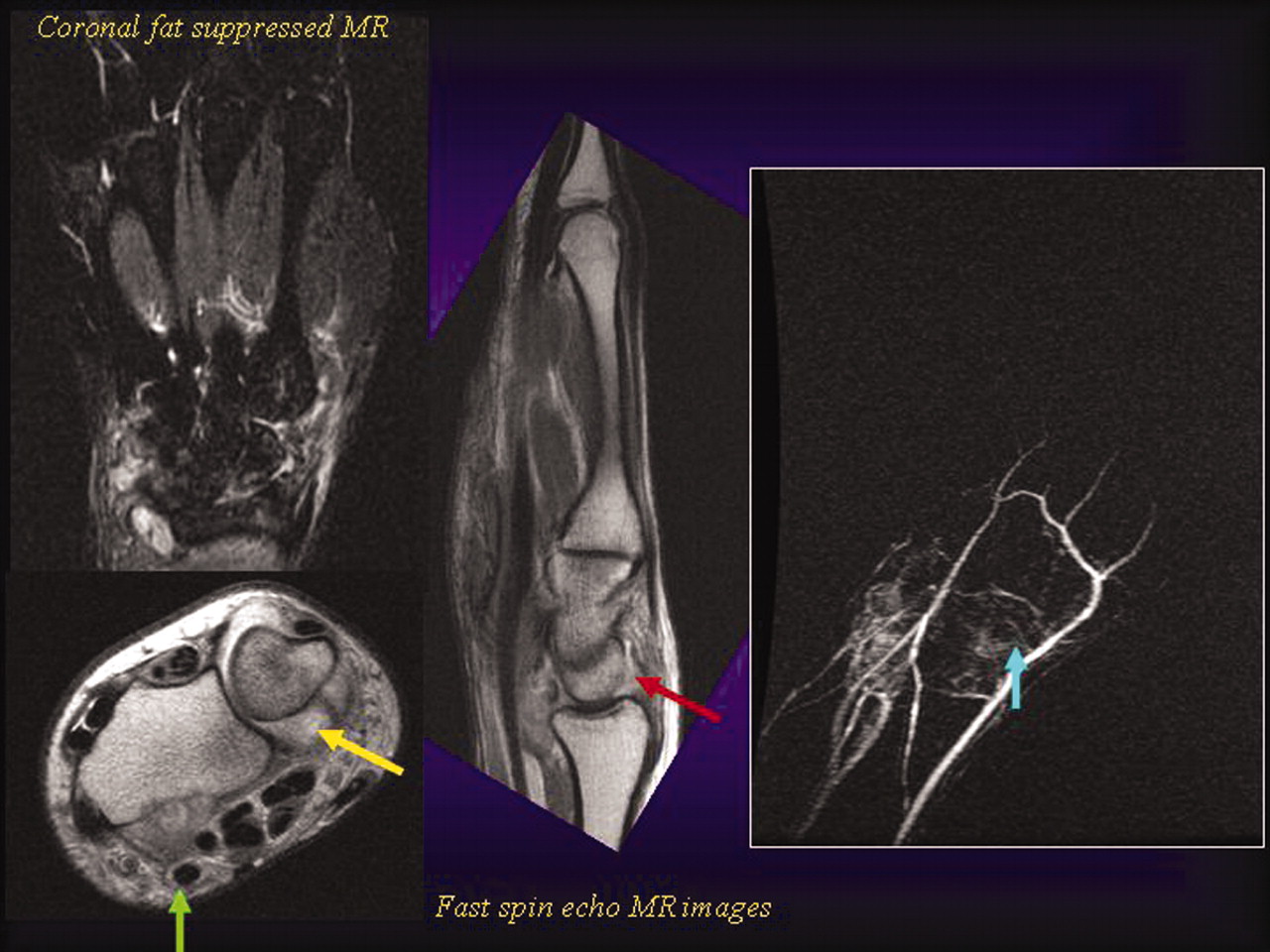
A patient with clinical synovitis, positive serologies, and DAS = 5.32. Fat-suppressed coronal MRI shows reactive bone marrow edema pattern affecting all joint compartments of the wrist. Axial and sagittal fast spin-echo MR images show synovial debris within the distended distal radioulnar joints (yellow arrow) and radiocarpal joints (red arrow). Note also the presence of tenosynovitis of the flexor carpi radialis (green arrow). MR angiography shows the presence of new vessels (blue arrow) at the level of the midcarpal joint.
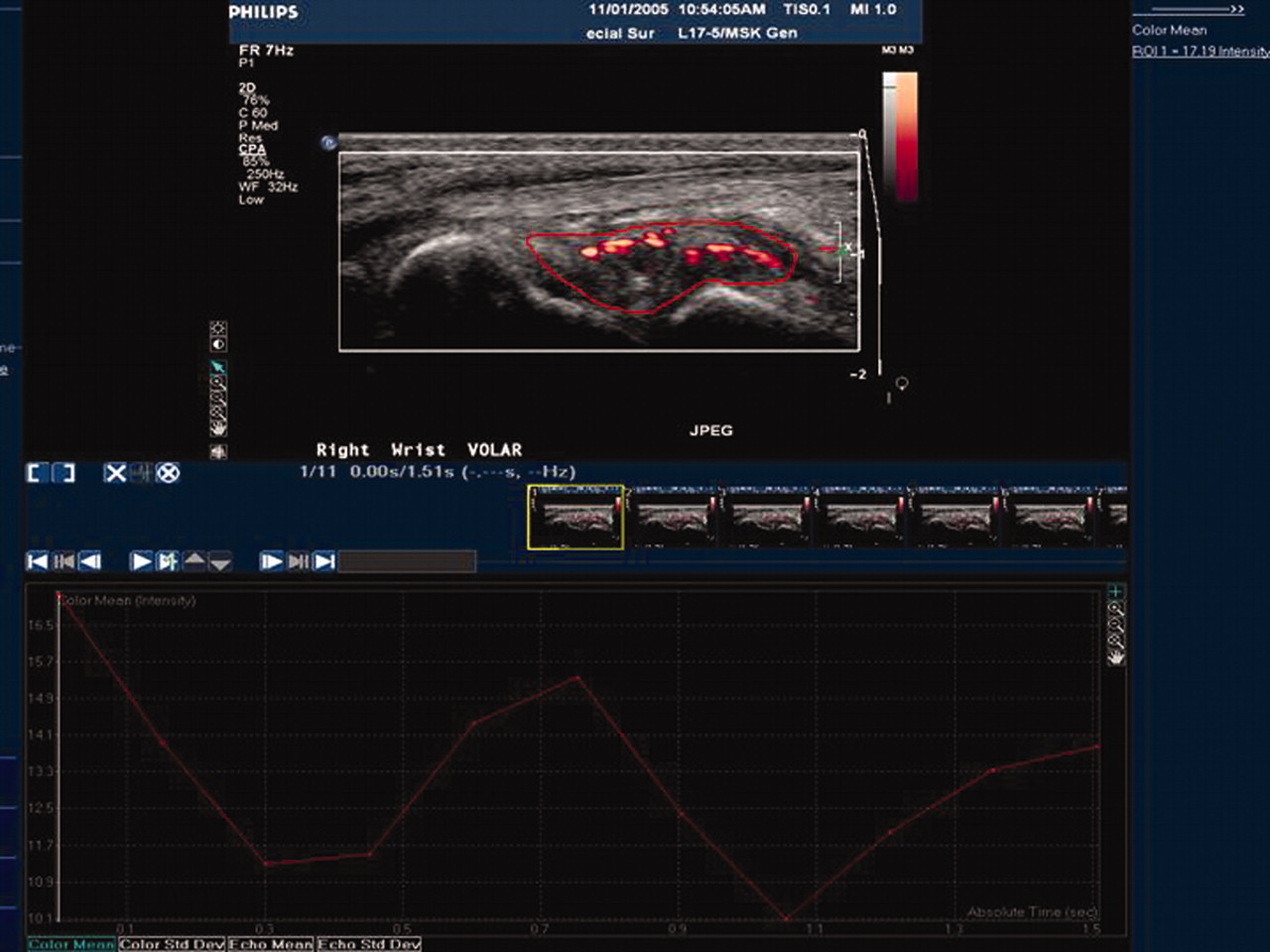
Power Doppler ultrasound of the same patient shows the volar aspect of the wrist along the radioscaphoid joint. A region of interest encompasses hypoechoic soft tissue with increased vascularity. The graph plots the mean power Doppler signal intensity (dB/mm2) versus time. The pulsatility reflects the arterial component of the visualized vascularity.

The hand and wrist of a patient with minimal clinical synovitis, negative serologies, and DAS = 2.61. Fat-suppressed and fast spin-echo MR images show no evidence of synovitis affecting the wrist joints. MRA reveals no evidence of neovascularity. Coronal T1 fat-suppressed MR images after injection of contrast also show no abnormal areas of synovial enhancement.
DISCUSSION
Angiogenesis of the synovium is a critical, early stage in the progression of synovitis and joint destruction. The new vascular network provides inflammatory cells access to the synovium and promotes the synovial hyperplasia that leads to bone and cartilage destruction20. Case reports using contrast-enhanced MRA have shown a proliferative network of small vessels in the periarticular distribution of patients with longstanding RA21, but MRA has not been systematically used to evaluate abnormal vascular recruitment in patients with early inflammatory arthritis.
Our study was designed to evaluate the validity of MRA as a method to detect abnormal vessels in patients with very early inflammatory arthritis of the hand. MRA was not previously used to image the small vessels of the wrist and hand, areas commonly involved in early inflammatory arthritis, because high resolution is needed to view the small-caliber vessels (often < 1 mm in diameter) and the acquisition time must be short to avoid venous contamination21. To address the previous limitations of MRA, we used a 1.5 or 3 Tesla MR scanner with a high quality receiver coil and time-intensity sensitive software, which permits tracking of the contrast into the affected joints as a function of time. MRA is a relatively noninvasive technique by which direct angiographic views of the affected joints can be obtained without the attendant risks of arterial puncture and ionizing radiation that exist with conventional contrast angiography. The MRA requires about 5 additional minutes in the MR unit and may be performed at the same session as the MRI.
Gadolinium-enhanced MRI is able to demonstrate increased contrast distribution in areas where there is increased local tissue perfusion, and the inflamed rheumatoid synovium produces cytokines, causing increased vascular permeability3,6. MRI evidence of synovial gadolinium enhancement correlates with histological evidence of an elevation in numerical density of blood vessels (number of vessels per square millimeter) in RA patients with knee synovitis3. Conversely, in RA patients without clinical knee synovitis, biopsies of the knee synovium show no vascular proliferation, even though perivascular mononuclear cell proliferation and synovial lining-layer thickening were evident3,6. MRI evidence of synovitis and bony abnormalities has also been shown to correlate with histological evidence of synovitis and vascularity in the MCP of patients with RA22. MRI does not, however, offer a direct method to quantify synovial vascular proliferation.
PDU has also been used to examine synovial blood flow in patients with synovitis. PDU can be used to distinguish active synovitis from inactive synovial thickening23. PDU measures of blood flow are strongly associated with clinical and laboratory assessment of disease activity24 and synovitis on post-contrast MRI25. Although PDU measurements are highly associated with histologic evidence of synovial vascularity in patients with RA, it is a measure of dynamic blood flow without direct correlation to neovascularization26.
While MRI and PDU offer indirect evidence of disease activity, MRA can provide direct visualization of pathologic synovial neovascularization. Inclusion of time-resolved angiography following injection of Gd-DTPA allows detection of newly recruited vessels in the early phase, prior to diffuse synovial enhancement. To our knowledge, this technique has not previously been used to image small vessels of the hand in patients with early inflammatory arthritis.
While MRA did produce impressive images, it is important to correlate these findings with other validated methods of disease assessment noted above. The number of vessels seen on MRA showed high correlation with PDU assessment of synovial blood flow, suggesting that MRA assessment of synovial vascularity is an accurate measurement tool. MRI has additionally been validated as an indirect measure of synovial vascularity22,27. Therefore, we also correlated the number of vessels seen on MRA with OMERACT MRI bone edema, bone erosion, and synovitis scores. The number of vessels on MRA also showed a strong and statistically significant correlation with OMERACT RAMRIS scores of synovitis at the wrist and MCP, and OMERACT RAMRIS bone edema and bone erosion scores at the wrist.
Tender and swollen joint counts, elevated CRP, and presence of RF and anti-CCP antibodies have predictive value for progression to RA in patients with undifferentiated arthritis28. Number of vessels seen on MRA showed a moderate and statistically significant correlation with the presence of RF, anti-CCP antibodies, and ESR, although not with CRP. There was no correlation between the number of vessels seen on MRA and the MDHAQ or DAS28 scores. The lack of correlation with these health status scales underscores the poor discriminatory value of clinical findings in early disease. The significant correlation with RF and anti-CCP antibodies, well known predictors of disease progression, suggests that vessels visualized by MRA may indeed be “imaging biomarkers” of disease severity.
Baseline bone edema measured by MRI has been shown to be a measure of disease severity in patients with early RA29,30. Baseline MRI bone edema at the wrist is predictive of 6-year Sharp score for patients with early RA29. The CIMESTRA group demonstrated that baseline bone edema is a predictor of radiographic progression in the hands, wrists, and forefeet at 2 years30. If MRA can accurately measure neovascularization at the synovial level, before bone involvement, it could potentially be used as an indicator of disease severity and need for treatment in patients with very early, undifferentiated inflammatory arthritis.
Limitations of our study include a small sample size and the use of both a 1.5 and 3 Tesla MRI machine. Although 3 patients were scanned at 3 Tesla and the remaining 26 were scanned at 1.5 Tesla, the signal to noise ratio of the MRA at 1.5 Tesla is quite high and the same in-plane and through-plane resolution was used at both field strengths. No difference in visualization of vascularity was encountered between the different field strengths. While patients reported no more than 6 months of symptoms, it was surprising that 47% of patients had evidence of erosions on plain radiographs. If recall bias led to the inclusion of patients with more established disease, our findings might not be generalizable to patients with very early inflammatory symptoms. Alternatively, the study may have preferentially attracted patients with short-term but more aggressive clinical disease. Further study of a larger, more diverse number of patients is necessary to evaluate the generalizability of our findings.
Our study documents that abnormal synovial vascularization can be visualized by MRA as early as 6 weeks after the start of inflammatory hand symptoms. MRA evidence of new vessels strongly and significantly correlates with PDU evidence of blood flow. While degree of blood flow is an indirect measure of disease activity, abnormal vascular recruitment is direct evidence of synovial pathology. Evidence of early synovial neovascularization may be a putative “biomarker” for aggressive disease. Large prospective studies are needed to determine whether abnormal neovascularization, as measured by MRA, predicts severity of disease course or response to treatment. If neovascularization is predictive of future severe erosive disease, it would allow treatment when disease activity is still at the synovial level, perhaps even before the development of cartilage and bone involvement.
Footnotes
-
Supported in part by the General Clinical Research Center at the Weill Cornell Medical College, NIH/NCRR Grant M01 RR00047, a NIH T32 Training Grant, a NIH CreFF Award, an Arthritis Foundation Postdoctoral Fellowship Award, a Gosden-Robinson Foundation Early Arthritis Research Award, a General Electric Health Care Research Grant, NIH grant K23 AR050607-01, and a Clinical Investigator Award from New York State and the National Arthritis Foundation.
- Accepted for publication January 21, 2010.








{kind=link}
{kind=link}
{kind=link}