

Abstract
Objective. The Visual Assessment of the Spine Bruckel Instrument (VASBI) is a new status tool developed by the Spondylitis Association of America and the University of Toronto to reflect spinal appearance in patients with ankylosing spondylitis (AS). Our objective was to validate the VASBI according to the Outcome Measures in Rheumatoid Arthritis Clinical Trials filter (truth, discrimination, and feasibility).
Methods. Three hundred patients with AS were asked to rate their degree of perceived spinal deformity using the VASBI. To evaluate construct validity, VASBI scores were compared with functional outcome, spinal mobility, and radiographic spinal damage. Test-retest reliability was evaluated using kappa statistic (κ).
Results. Patient VASBI demonstrated strong correlation with spinal mobility (r = 0.543) and moderate correlation with functional impairment (r = 0.490) and structural damage (r = 0.309). Reliability for VASBI was very good (κ = 0.973, p < 0.001).
Conclusion. The VASBI is a novel tool with practical applications in a busy clinical setting as it simplifies assessment of AS spinal deformity. Our study demonstrates that the VASBI has good feasibility, construct validity, and reliability.
One of the earliest features of ankylosing spondylitis (AS) is loss of spinal mobility1. Evaluation of spinal mobility is an important part of patient subgroup stratification. Further, it provides a baseline at the commencement of appropriate therapy and determination of clinical outcomes2,3. To this end, the Assessment in AS (ASAS) Study Group has identified spinal mobility as one of the core domains for the evaluation of disease-controlling therapies and for clinical recordkeeping in AS4. Based on the ASAS Study Group recommendation, spinal assessment should be incorporated into routine clinical and research practice4,5. Spinal deformity is also a common feature of AS, and at present, rheumatologists rely on clinical and radiographic examination to assess the degree of spinal deformity in patients with AS. Measurements of spinal involvement (mobility/deformity) in the clinical setting can be assessed using the Bath Ankylosing Spondylitis Metrology Index (BASMI)6, which consists of 5 clinical measures to assess axial spine status in patients with AS. Radiographic damage is measured using the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS), which is considered superior to the other radiographic scoring systems7,8. However, these measurements can be time-consuming, requiring a metrologist for accuracy and appropriate resources that are often lacking in physicians’ offices. Other spinal measurement tools have been developed9,10, but few have undergone validation according to the Outcome Measures in Rheumatoid Arthritis Clinical Trials (OMERACT) filter, which examines truth, discrimination, and feasibility11.
To date, no quick and easy tool has been developed for defining the status of spinal deformity in patients with AS. Thus the Visual Assessment of the Spine Bruckel Instrument (VASBI) was developed for use in AS by the Spondylitis Association of America (SAA) and the University of Toronto (Figure 1). It is named after Jane Bruckel, a former executive director of the SAA. It is a simple status tool reflecting a patient’s spinal appearance that can be used by anyone regardless of their education background. It is very feasible as it takes less than 10 seconds to complete, is of minimal cost, and is easily scored.
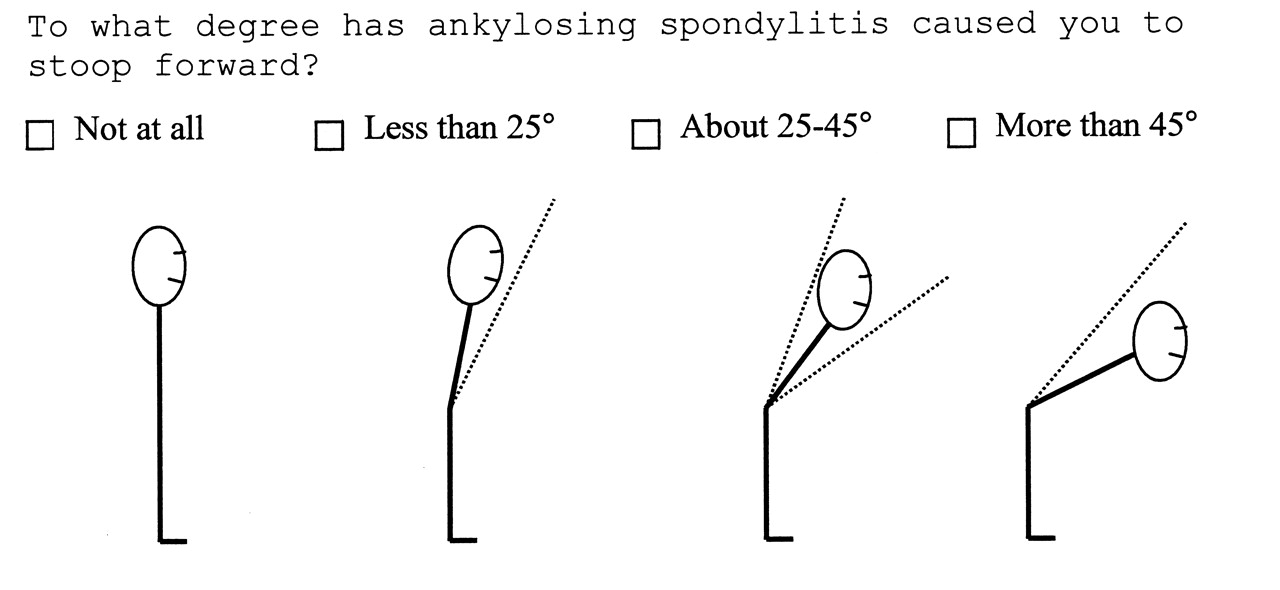
Patient version of the Visual Assessment of the Spine Bruckel Instrument (VASBI).
In this report, we aim to demonstrate construct validity and reliability of this tool that simplifies assessment of spinal deformity in patients with AS. Using a large and representative sample of patients with AS from the United Kingdom, we illustrate VASBI’s validity according to components of the OMERACT filter.
MATERIALS AND METHODS
Development of the VASBI
An illustration for assessment of spinal deformity was developed by Jane Bruckel and a group at the SAA consisting of health professionals, patients with AS, a methodologist, and a graphic designer. It was originally developed for patient use for self-assessment of the degree of perceived spinal deformity. The individual using the tool is asked to choose 1 of 4 diagrams depicting the forward stoop and representative of spinal curvature of the patient with AS. The score range is 1 (no stoop forward) to 4 (> 45° stoop forward). The authors were not involved in designing the illustration.
Patients
Three hundred individuals enrolled in the Spondyloarthropathy Methodology and Research Therapeutics (SMART) Study at the Royal National Hospital for Rheumatic Diseases (RNHRD) in Bath, England, were recruited after giving informed consent. This cohort was a combination of inpatients and outpatients followed prospectively by the attending rheumatologist. To identify the spectrum of disease in AS, the European Spondylarthropathy Study Group guidelines were used as the inclusion criteria12.
Methods
As part of the SMART clinic at RNHRD, patients are asked to complete a set of questionnaires that included the VASBI and demographic, socioeconomic, and clinical data. Patients were asked to rate the degree of perceived spinal deformity by scoring the VASBI (Figure 1).
The following clinical variables were collected: age, disease duration, gender, validated measures for axial spinal status using BASMI6, radiographic spinal damage using mSASSS7 (which is recommended by ASAS13), functional outcome using BASFI14, and the Ankylosing Spondylitis Quality of Life Questionnaire (ASQOL)15. Not all patients had complete assessment of each outcome measure because of the logistical time constraints of conducting the study in an ambulatory outpatient clinic.
Data from these tests were used to assess construct validity of the VASBI. The respective contribution to spinal mobility was determined according to individual items of the BASMI, the entire BASFI score, and items 1, 2, and 8 of the BASFI. We investigated independent questions from the BASFI because they represented activities (i.e., putting on socks, bending forward, looking over shoulder) in which spinal mobility was necessary. All the BASMI were scored by one AS physiotherapist and a member of the group that developed the BASMI instrument. All radiographs were scored by one observer who is a trained expert in mSASSS. Test-retest reliability of the VASBI was assessed by asking participants to repeat the assessment 1 day and 1 week after their hospital visit.
Members of the SAA and physicians from the University of Toronto performed a pilot study to evaluate construct validity of the VASBI in 200316. Self-perceived spinal deformity, using this instrument, was compared to functional outcome, as measured by the BASFI, in 2720 patients with AS who participated in the Life Impact Study, a nationwide survey conducted by the SAA in 2003. Based on these data, our study was planned and conducted, in which the instrument could be tested more rigorously in the clinical setting according to components of the OMERACT filter.
Face validity
Members of the SAA, patients with AS, and physicians from the University of Toronto with international reputations as experts in the management of AS (M.A. Stone and R.D. Inman), determined that VASBI had good face and content validity, according to OMERACT filter definition11. Based on the consultative process, it was felt that the VASBI had face validity because it appeared to an expert in the field to measure at least one aspect of AS (spinal appearance). Moreover, the VASBI achieved content validity because experts in the field felt that it determined the dimensionality of the manifestations of AS (spinal structure and mobility).
Truth: construct validity
Construct validity was gauged by analyzing correlations (using Spearman’s rho for nonparametric data) between the patient-scored VASBI and other indices of spinal deformity. These included spinal mobility using BASMI, radiographic spinal damage using mSASSS, and functional outcome using BASFI. A positive and moderate correlation of these indices and the VASBI was expected. The VASBI score was also compared with individual items on the BASMI and BASFI as described in the Methods section. The correlation coefficients were interpreted according to Cohen’s categories for strength of association, which are strong (r between 0.5 and 1.0), moderate (r between 0.3 and 0.5), small (r between 0.1 and 0.3), and insignificant (r < 0.1)17.
Discrimination: reliability
The agreement between test and retest was calculated using Kappa statistic, where a value of 0.2–0.4 was fair agreement beyond chance, 0.4–0.6 moderate agreement beyond chance, 0.6–0.8 substantial agreement beyond chance, and 0.8–1.0 almost perfect agreement beyond chance18.
Discrimination: responsiveness
Because of the small number of potential scores for the VASBI (1–4), it was not appropriate to evaluate common indicators of responsiveness such as the effect size or standardized response mean. Because the VASBI is a status tool, the authors did not assess its responsiveness.
The statistical package used was SPSS for Windows (version 12.0). A p value < 0.05 was considered significant in all analyses.
RESULTS
Patient characteristics
Of the 300 individuals enrolled in the study, 57% were experiencing extraarticular features and 80% were diagnosed with AS according to the modified New York criteria1. Of the 236 who were tested for HLA-B27, 89.4% were positive (Table 1). Most of the patients were male (75%) and the mean (± SD) duration of symptoms since onset was 27.1 (12.57) years. The mean ± SD for BASFI, BASMI, and mSASSS were 4.6 (2.54), 3.6 (1.91), and 14.2 (19.92), respectively (Table 1).
Characteristics of patients with SpA in VASBI study.
Patient VASBI (Table 2) demonstrated moderate correlation with functional impairment (BASFI: r = 0.490), and structural damage (mSASSS: r = 0.309), and a strong correlation with spinal mobility (BASMI: r = 0.543). The patient-scored VASBI scores demonstrated moderate correlation with the 3 BASFI questions.
Assessment of construct validity of the VASBI: Correlation between measures (BASFI, BASMI, mSASSS) and patient VASBI score.
Of the individual BASMI components, tragus-to-wall measurement showed a strong correlation with patient-scored VASBI; lumbar flexion, lumbar side flexion, and cervical rotation showed moderate correlations with patient-scored VASBI and weak correlation with intermalleolar distance. Correlations with individual mSASSS component scores were weak.
The VASBI was assessed in patients for reliability. The VASBI scores at baseline (clinic response) were found to have substantial agreement with VASBI results in the same patient 1 day and 1 week later [1 day: n = 67, Kappa = 0.739 (SE = 0.080); 1 week: n = 63, Kappa = 0.786 (SE = 0.076)]. One-day and 1-week responses were in near-perfect agreement [n = 75, Kappa = 0.973 (SE = 0.027)].
DISCUSSION
We have demonstrated that the VASBI, a new status tool to assess the appearance of the spine in AS, is very feasible and shows good construct and face validity, and reliability. It is a simple tool that relies on the visual assessment of the spine in patients with AS and can be used in a busy clinical setting to quickly assess the appearance of the spine, which in turn is a reflection of spinal damage and mobility.
Patient-assessed health instruments have become an important tool in determining different aspects of a patient’s health, particularly in rheumatology19–21. Currently in AS, the plain radiograph is the “gold standard” for assessing structural damage and the BASMI serves as a clinical measure of spinal mobility. However, plain radiographs are not always readily available and along with the BASMI require training to score appropriately. The present study was prompted by the lack of a quick and easy tool that can reflect spinal degeneration in patients with spondyloarthropathy (SpA). There is a need for a simple tool to measure spine involvement, especially in small communities with restricted resources.
The majority of self-assessment measures in SpA reveal the functional status of patients and some, like the BASDAI, describe disease activity22,23. Other self-report instruments like the Patient Acceptable Symptom State24 are used, but the VASBI is unique because it is an illustration meant to mirror a patient’s spinal appearance. When we compared this novel instrument to other indices of spinal function and structure (i.e., BASFI, BASMI, mSASSS), we achieved significant correlation, demonstrating good construct validity25. Reliability of the instrument was also highly significant on test-retest comparisons.
The VASBI’s categorical quality prevented the assessment of responsiveness using common statistical methods such as effect size or standardized response means. Further, since AS is a slowly progressive disease in terms of spinal damage and loss of mobility, transition between the relatively broad categories of the VASBI would be expected to occur over a number of years in most cases26–29. Therefore we would expect that the majority of patients show no change over the 2-week intensive rehabilitation course because major changes in spinal deformity resulting in transition from one VASBI score to another would be unlikely. Further refinement of the instrument for precision is required before this instrument can be used to detect a change in therapy.
Patient VASBI scores achieved high correlation with BASFI items, indicating that a patient’s view of disease status tends to be influenced by their experience of the illness, again consistent with an earlier study30. Previous work by our group demonstrated a strong correlation between BASFI and VASBI16. Personality traits and a patient’s point of view influence self-reported health status31,32. However, the VASBI contains only 4 items, which makes it unlikely for personality type to influence the score unless the person’s spinal deformity is on the border between 2 items of the instrument. The precision of the instrument may also play a role if it is used to monitor response to treatment.
A study in Canada by Bellamy, et al found that rheumatologists are more likely to longitudinally follow patients with rheumatoid arthritis (100%) and AS (96%) than osteoarthritis (58%–74%) or fibromyalgia (51%)33. It was also pointed out that physicians agree on certain qualities of assessment techniques such as brevity, simplicity, and validity. The VASBI may be employed in the absence of spinal measuring tools such as the inclinometer or goniometer, which are not routinely available or used in clinical practice. It may also serve as a status tool to follow patients longitudinally and with modification to improve precision, for the detection of changes with treatment. Further, VASBI might be a cost-effective visual assessment tool that can be scored by both patients and physicians. Because of its availability and simplicity, VASBI is an ideal tool for use outside large urban centers to give us a better understanding of the spectrum of disease in the population.
VASBI is a feasible and reliable tool with good construct and face validity that may be used for assessing the spine in large cohorts and for tracking disease progression. This measure can provide physicians with a quick and easy tool to follow patients with spinal deformities such as AS.
Footnotes
-
Supported by a joint award from the Spondylitis Association of America and the National Ankylosing Spondylitis Society of the UK; and by the donated funds award from the Royal National Hospital for Rheumatic Diseases, Bath. Dr. Podbielski is the recipient of a Canadian Arthritis Network Summer Research Program Studentship, the Spondylitis Association of America (SAA) Studentship, and the St. Michael’s Hospital Summer Research Student Scholarship. Dr. Stone is the recipient of the Cumming Visiting Professor Award and SAA award.
- Accepted for publication October 9, 2009.








{kind=link}