

Abstract
Objective. Hepatitis C virus (HCV)-associated mixed cryoglobulinemia (MC) vasculitis is an autoimmune disorder with significant morbidity and mortality. Renal involvement was associated with an increased mortality, and was the most common cause of death; these data were obtained before effective antiviral treatment was available. We studied causes of death and predictive factors in patients with HCV-associated MC vasculitis treated with antivirals.
Methods. Case histories of 85 patients with HCV-associated MC vasculitis treated in a single center between 1990 and 2006 were retrospectively reviewed. Prognostic factors affecting mortality were studied by comparing 23 patients who died with 62 survivors, using the Cox model regression analysis.
Results. The most common cause of death was infection, accounting for 34.7%, followed by endstage liver disease in 30.4% (including 4 patients with hepatocellular carcinoma), and cardiovascular disease in 17.4% of patients. Endstage renal disease accounted for only 8.7% of deaths, as did central nervous system vasculitis and nonhepatic malignancy. Increased mortality was strongly associated with immunosuppressive treatment [hazard ratio (HR) 6.51, 95% CI 2.75–15.37], cutaneous ulcers (HR 5.37, 95% CI 1.79–16.14), and renal insufficiency (HR 3.25, 95% CI 1.37–7.72). A 2 log10 decrease in HCV viral load at month 3 after starting antiviral treatment was associated with decreased mortality (HR 0.39, 95% CI 0.16–0.95).
Conclusion. While renal involvement is still associated with poorer prognosis, infectious processes are now the most common cause of death in HCV cryoglobulinemia vasculitis. Immunosuppressive treatment is associated with an increased risk of death, independently from disease severity. Response to antiviral treatment is associated with significantly reduced mortality risk.
Mixed cryoglobulinemia (MC) vasculitis is a life-threatening, systemic vasculitis1–3 caused by a B cell proliferative disorder4. MC may lead to clinical manifestations ranging from MC syndrome (purpura, arthralgia, asthenia) to severe vasculitis with nervous system and renal involvement2,3,5.
The identification of a causative role for hepatitis C virus (HCV) in MC vasculitis, together with improving antiviral therapeutic options, dramatically changed the prognosis of MC vasculitis. It has been demonstrated that antiviral treatment can lead to clinical remission and can induce an immunological response, i.e., a significant decrease in plasma cryoglobulin levels6. Further, the clinical response is closely related to effective viral elimination5,6, supporting the causal link between chronic HCV infection and the autoimmune process. The clinical response to the vasculitis progressively increased while antiviral efficacy increased from initial use of standard thrice-weekly interferon (IFN) to combination therapy with IFN and ribavirin (RBV)7–9, and to a more recent combination with polyethylene glycol-IFN (PEG-IFN) plus RBV6.
HCV-induced MC vasculitis can still cause significant morbidity and mortality. Traditionally, the worse prognostic factors were age (older than 60 years at diagnosis) and renal involvement10, with 5-year survival ranging from 50% to 90% with renal involvement11. In studies by Meltzer, et al12 and Gorevic, et al1, renal involvement was the main cause of death. Even in the absence of significant renal failure, increased mortality from liver involvement, cardiovascular disease, infection, and lymphoma has been reported10. In a retrospective Italian study of 231 patients, 46% of deaths were linked to vasculitis (over one-third were due to renal disease), lymphoma, and hepatocellular carcinoma (23%), or liver disease (13%)10. In another study, life-threatening MC complications were observed in up to 14% of the patients, with a 66% mortality rate13. Intestinal ischemia, pulmonary hemorrhage, high cryocrit levels, and type II MC were associated with poor prognosis13.
However, most of the results of these studies were derived from older data (for example, the Italian series included patients as early as in 1972), and therefore may not reflect recent changes in therapeutic practices. We have reconsidered this question in order to assess whether advancements in treatment options (in particular antiviral treatment and improved therapeutic options for renal failure) have changed the causes as well as the prognostic factors in mortality in HCV-induced MC vasculitis.
MATERIALS AND METHODS
Patients
The files of 85 chronically HCV-infected patients with MC vasculitis at the Department of Internal Medicine of a university hospital between 1990 and 2006 were retrospectively studied. Twenty-three patients who died (mean age at death 66.35 yrs; range 62–75 yrs) were compared to 62 consecutive patients who survived (mean age at end of study 59.21 yrs; range 48.5–72.5 yrs). All had positive anti-HCV antibodies (detected by third-generation enzyme-linked immunosorbent assay, Ortho Diagnostics, Cardiff, UK) and HCV-RNA and were negative for hepatitis B surface antigen and anti-HIV antibodies. The most common genotype was genotype 1 (71.5%), with genotype 1b accounting for 53% and 1a accounting for 26% of the patients. All patients had an MC level in serum > 0.05 g/l, at at least 2 determinations. Symptomatic MC was defined by serum MC associated with the triad of purpura-arthralgia-asthenia, sometimes associated with renal or neurologic involvement. Histological evidence of vasculitis was obtained in 78.2% of the patients, while in 21.8%, the MC vasculitis diagnosis was based on clinical and laboratory features12. Followup included visits at least every 2 months. All patients received IFN-based antiviral therapy with or without immunosuppressive treatments.
Demographic information such as age at diagnosis, gender, and presumed mode of HCV transmission was recorded. Clinical details recorded were manifestations of vasculitis; cause of death (obtained from patients’ files, certificates of death, or autopsy results); evidence of a lymphoproliferative disorder; antiviral treatment type, dose, and duration; immunosuppressive treatment type, dose, and duration; and clinical, immunologic, and virologic response to treatment at 3 and 12 months after beginning antiviral treatment, at 6 months after stopping antiviral treatment, and at the end of the followup (last data before death). The following laboratory data were taken (all at the time of initial diagnosis): creatinine level (μmol per liter); proteinuria (g per day); alanine aminotransferase (ALT) level expressed in multiple of upper level of normal value (ULN) before and after treatment; HCV genotype (second-generation line probe assay, Innogenetics, Brussels, Belgium); viral load before and after treatment (expressed in log10); cryoglobulinemia type and level (g/l); complement C4 (g/l); rheumatoid factor (RF) activity by latex and Waaler-Rose test, before and after treatment; and liver degree of fibrosis and necro-inflammation evaluated on hepatic biopsy and/or fibrotest-actitest14 and expressed by the Metavir score15 before and after treatment.
Antiviral treatment
Patients were treated with PEG-IFN with or without RBV (45 patients, 52.9%) or standard IFN with or without RBV (40 patients, 47.1%), for a minimum of 6 months, according to common clinical practice.
Different types of treatment responses were recorded. Clinical response for patients with MC vasculitis was defined by analyzing the course of the following main clinical signs: skin involvement (absence of purpura), peripheral neuropathy (clinical and electrophysiologic improvement on 2 successive examinations), renal involvement (normalization of serum creatinine level and disappearance of proteinuria), and the absence of arthralgia. A complete clinical response was defined as a full improvement in all baseline clinical manifestations. Complete immunologic response was defined by the absence of serum cryoglobulin (< 0.05 g/dl). Patients had sustained virologic response when they had undetectable viremia 6 months after stopping antiviral treatment. Of note, none of the patients received rituximab.
Statistics
Data were summarized as incidences and percentages for categorical variables. Quantitative variables were described using means and SD. We compared the 23 patients who died with a cohort of 62 patients with HCV MC vasculitis followed at the same department during the same period and still alive in March 2006. The Cox model adapted for survival data was used to test the association between death and potential predictive factors and to quantify the effect size measured by estimated hazard ratio (HR) with 95% confidence interval (CI). This was an inception cohort with baseline data taken at the time of MC vasculitis diagnosis. Considering that no deaths occurred during the first 3 months in our study, response at 3 months was tested as a potential predictive factor.
Unadjusted and adjusted HR were computed, with adjustment performed through the use of a multivariable model introducing factors associated with the outcome at the 10% level in univariable analyses. The factor selections were determined using a backward procedure based on the Akaike criteria. All tests were 2-sided with a significance level of 0.05. Analyses were performed using the R statistical package (online at http://www.R-project.org).
RESULTS
Clinical characteristics of mortality cohort
Between 1990 and 2006, 23 patients (14 men, 9 women) died. They were infected with HCV with significant cryoglobulinemia (0.05 g/l) and followed for vasculitis in our department (main clinical characteristics in Table 1). The most common mode of transmission was blood transfusion for 7 patients (30.4%) and intravenous drug use for 3 patients (13.1%), while in 13 patients (56.5%) the mode of transmission was unknown. The mean delay between the diagnosis of HCV infection and death was 15 years (range 1.5–35) and between first vasculitis manifestation and death 65 months (range 16–172).
Main characteristics of patients with HCV cryoglobulinemia vasculitis, including a multivariate analysis of patients who died compared with surviving patients at the end of the study.
Vasculitis involvement of the peripheral nervous system was demonstrated in 19 cases (82.6%), with clinical and electromyographic features of sensory and/or motor polyneuropathy for 13 patients and mononeuropathy multiplex for 6 patients. Cutaneous involvement was reported in 13 patients (56.5%), all with purpura, and 4 patients had both purpura and leg ulcers. Arthralgia was reported in 12 cases (52.1%) and renal involvement in 9 (39.1%). Central nervous system involvement was reported for 3 patients (13%), Raynaud’s phenomenon for 3 (13%), and gastrointestinal involvement (presenting with abdominal pain and melena secondary to bowel ischemia) for 2 patients (8.7%). Lymphoproliferative disorders were reported in 3 patients (splenic lymphoma with villous lymphocytes, Waldenström’s disease, and tonsillar T cell lymphoma). Pretreatment mean creatinine serum level was 159 μmol/l (range 58–630), with creatinine clearance of 55 ml/min (range 2–108), and mean daily proteinuria of 1.08 g (range 0–6.8). At the last point of followup before death, these were, respectively, 200 μmol/l (range 55–729), 48 ml/min (range 2–94), and 1 g (range 0–5.9). Four patients were treated with dialysis, all for rapidly progressive membrano-proliferative glomerulonephritis. Arthritic involvement was not noted in any patient in this cohort.
Mixed cryoglobulinemia, according to Brouet classification16, was type II IgM K (78%) or type III (22%). Pretreatment and last followup cryoglobulinemia mean levels were, respectively, 0.52 g/l (range 0–1.35) and 0.36 g/l (range 0–2.55), C4 levels were 0.086 g/l (range 0.02–0.2) and 0.13 g/l (range 0.01–0.33), and RF levels were 57 IU/l (range 0–301) and 40 IU/l (range 0–301). Pretreatment ALT levels were 1.6 ULN (range 1–4), mean Metavir activity score was 1.3 (range 0–3), and the mean Metavir fibrosis score was 2.3 (range 1–4). At last followup, those levels were, respectively, 1.4 (range 1–3), 1.2 (range 0–3), and 2.7 (range 1–4).
All patients received antiviral treatment. The mean number of treatment courses was 1.87 (range 1–5) with a mean total antiviral treatment duration of 27.4 months (range 6–108). Only 4 out of 23 patients who died had a duration of antiviral treatment < 9 months. Eleven patients (48%) were treated by IFN alone, 2 (8.7%) by PEG-IFN alone, 5 (21.8%) by a combination of IFN plus RBV, and 5 (21.8%) by PEG-IFN plus RBV. Mean dose of RBV was 875 mg/day (range 600–1200 mg) and 1.2 μg/kg/week (range 1–1.5) for PEG-IFN-α2b. Efficacy of antiviral treatment on clinical, virological, and immunological features is summarized in Table 2. Main adverse effects of antiviral treatment were depression (40%), hemolytic anemia (16.6%), and thrombocytopenia (15%). Immunosuppressive treatments were administered in 15 patients (65.2%); all received corticosteroids for a mean duration of 18.5 months (range 3–84), at a mean dose of 0.82 mg/kg/day (range 0.2–1). Methylprednisolone pulses were administered to 8 patients, cyclophosphamide to 7, and methotrexate to 1 patient. A mean of 10.9 (range 4–28) plasma exchanges were performed for 11 patients. Of note, no case was noted of cessation of immunosuppressive treatment due to infection.
Response to antiviral treatment in patients with HCV cryoglobulinemia vasculitis after 3 months of treatment. Patients who died are compared with surviving patients at the end of the study.
Causes of death
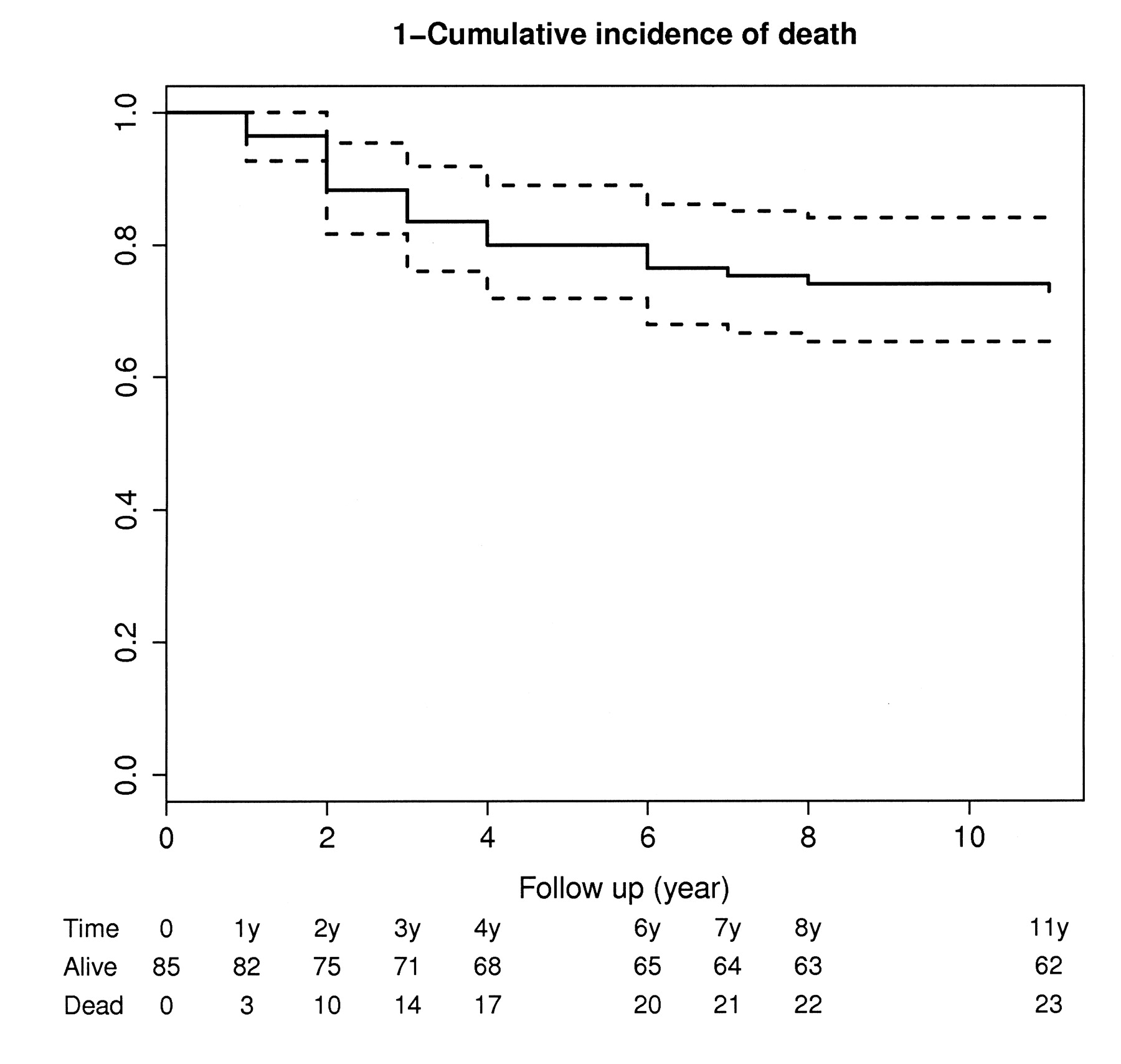
Causes of death were available for 22 of the 23 patients who died (Table 3). Most deaths occurred during the first 4 years of followup (Figure 1).
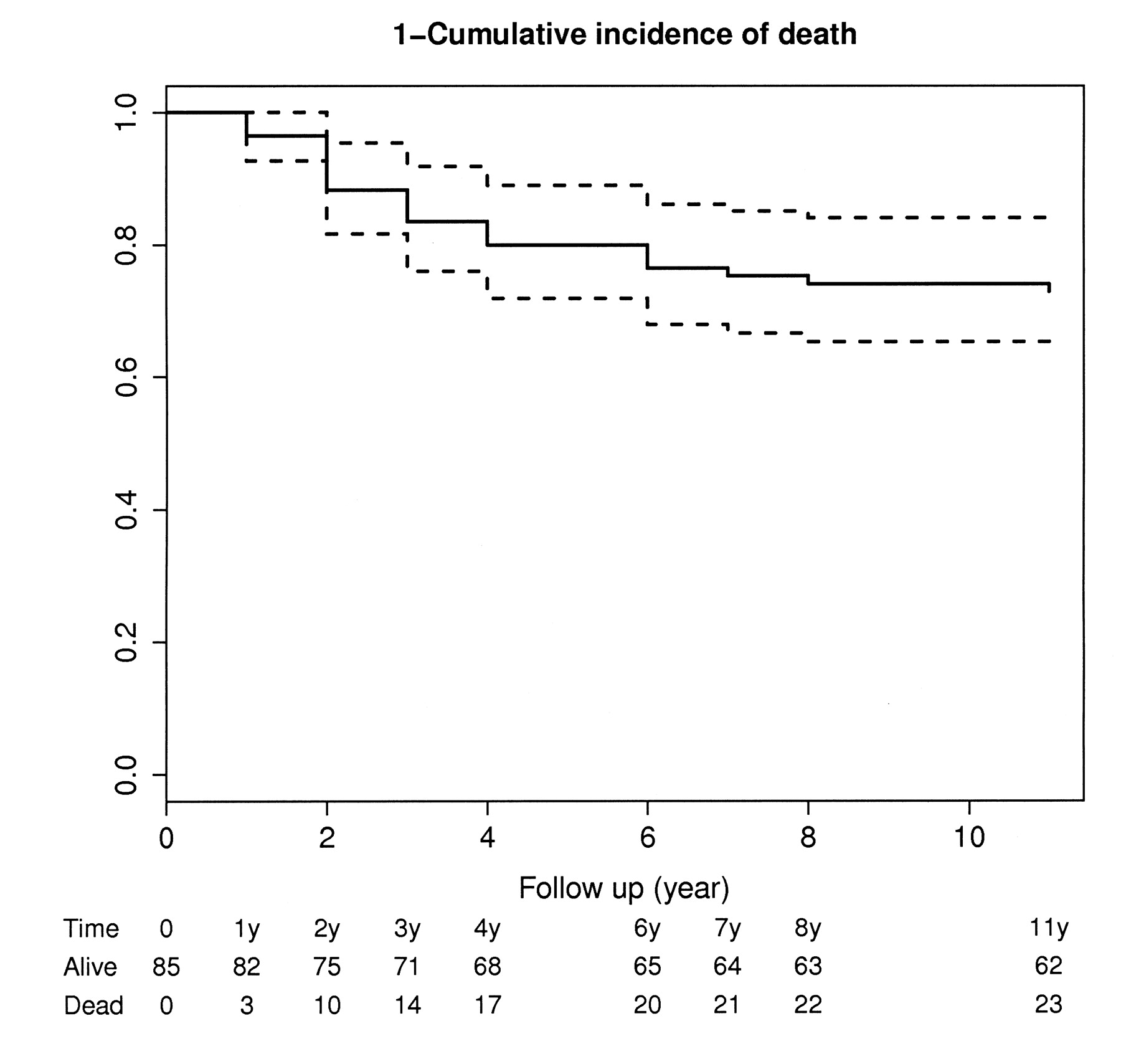
Kaplan-Meier plot showing the cumulative incidence of death by years of followup. Broken lines represent 95% confidence interval.
Causes of death in patients with HCV cryoglobulinemia vasculitis. For 3 patients, 2 different causes contributed to death.
The most common cause of death was infection, accounting for 8 patients (34.7%). Septic shock was the common final pathway, secondary to pneumonia in 3 patients, peritonitis related to dialysis catheter in 1 patient, cutaneous abscess for 1 patient, and with undetermined origin for the remainder. In 2 patients, the infection occurred in the setting of mesenteric ischemia secondary to gastrointestinal involvement of the MC vasculitis. Among these 8 infection-related deaths, 5 patients received immunosuppressive treatment (corticosteroid treatment in 5, cyclophosphamide and plasmapheresis in 4, and methothrexate in 1 patient), although only 1 patient was receiving immunosuppressive treatment at the time of death. Four patients had renal insufficiency, 4 had cirrhosis, and 2 had lymphoproliferative disorders (Waldenström’s macroglobulinemia and splenic lymphoma with villous lymphocytes).
Death occurred as a result of endstage liver disease in 7 patients (30.4%), i.e., 4 hepatocellular carcinoma and 3 direct complications of cirrhosis. Death was related to a cardiovascular disease in 4 patients (17.4%), i.e., heart failure in 2, sudden cardiac death in 1, and myocardial infarction in 1. In 2 patients, the cause of death was cerebral involvement of the MC vasculitic process, in 2 cases the cause was endstage renal disease, and 2 additional patients died from a malignant disease (tonsillar T cell lymphoma, lung cancer).
Prognostic factors for mortality
Factors associated with mortality were studied by comparing the 23 patients who died with 63 patients who were alive at the time of analysis. In a Cox model regression analysis (values expressed as HR, 95% CI), increased mortality was strongly associated with immunosuppressive treatment (6.51, 2.75–15.37), cutaneous ulcers (5.37, 1.79–16.14), and renal insufficiency (3.25, 1.37–7.72; Table 1). Other factors associated with increased mortality were Raynaud’s phenomenon (3.95, 1.13–13.77) and peripheral nerve involvement (2.91, 1.02–8.71). A 2 log10 decrease in HCV viral load at month 3 after starting antiviral treatment was associated with a lower mortality rate (0.39, 0.16–0.95; Table 2). Only 4 of the 23 patients who died had a genotype 2 or 3. Genotype (genotype 1 compared with other genotypes grouped together) did not have a statistically significant effect on mortality (0.53, 0.21–1.34).
In a multivariate analysis with model selection based on the Akaike criteria, the strongest factors influencing mortality rates were immunosuppressive treatment (HR 5.1, 95% CI 2.1–12.6), renal insufficiency (2.9, 1.2–7.3), and virological response at month 3 after starting antiviral treatment (0.4, 0.2–0.9). Virological response at month 12 of treatment and at the end of followup was far more common in patients who were alive at analysis compared with the patients who died (74.2% vs 17.4% and 62.9% vs 4.3%, respectively). Clinical response was more frequent at month 12 of treatment among patients who died, but less frequent at end of followup (30.6% vs 47.8% and 72.6% vs 21.7%), while immunological response was lower in patients who died at both timepoints (48.4% vs 34.8% and 48.4% vs 39.1%).
DISCUSSION
We evaluated the causes of death and prognostic factors associated with mortality in a large group of patients with HCV-associated MC vasculitis. Our first main finding was that the most common cause of death, accounting for over one-third of the patients, was infection. Infectious etiology was followed by liver disease, including endstage cirrhosis and hepatocellular carcinoma, heart disease, and in only a small proportion of patients, endstage renal failure or other vasculitis target-organ involvement. This is a stark difference from earlier studies in which vasculitis renal disease was the most common cause of death. This finding is particularly interesting considering the second major finding— that immunosuppressive treatment was the strongest negative prognostic factor, even after controlling for disease severity measurements.
In one of the largest case series, published by Ferri, et al, the most common cause of death for 231 patients with MC vasculitis was endstage renal disease, responsible for 33% of deaths with known cause10. The second most common cause was malignancies, accounting for 23% of deaths, followed by liver involvement, diffuse vasculitis, B cell lymphomas, and lung involvement. In an earlier report by Monti, et al17, liver disease and endstage renal disease were the most common causes of death, and others have reported similar findings18. Interestingly, although it is difficult to directly compare because of different definitions used, infectious causes have not been marked as an important cause of mortality in the previous large case series. Although in our study renal disease remained an important negative prognostic factor, renal disease is no longer the foremost cause of mortality, a difference that may stem from improved care and improved survival rates among patients with endstage renal disease, as demonstrated by the US Renal Data System cohort19.
When first described early in the 20th century, the vasculitidis syndromes were regarded as uniformly fatal. However, the use of corticosteroids and cytotoxic agents, notably cyclophosphamide, has significantly increased 5-year survival rates20. In most studies, mortality was most often a result of the primary vasculitic disorder21,22, because of either renal failure or other target-organ involvement23–26. However, infection remained an important cause of mortality, particularly in more recent case series22,24,25,27,28, as well as among patients in intensive care29. Predictors of poor prognosis were predominantly older age22,25,27, renal dysfunction22,27,30, central nervous system involvement22,30, and hepatic involvement30. Immunosuppressive treatment or its intensity were not found in multivariate analysis to be linked with increased mortality22. Our findings are also contrasted with epidemiological data from patients with chronic HCV, where the most common causes of mortality were related to liver disease and substance abuse31–33.
Considering the contribution of infections to mortality in MC vasculitis and the link with immunosuppressive treatment suggested in this study, the shift toward antiviral treatment is highly important. Further, in our study, early response to antiviral treatment was a strong positive prognostic factor. Antiviral therapy with standard IFN plus RBV has provided much better short-term and longterm results in patients with HCV-related vasculitis than historically reported with IFN7–9. More recently, it has been reported in 72 consecutive patients with HCV-MC that PEG-IFN plus RBV achieved a higher rate of complete clinical (67.5% vs 56.2%) and virological response (62.5% vs 53.1%) and a lower mortality rate (5% vs 18.8%) compared with standard IFN plus RBV, regardless of HCV genotype and viral load6. Importantly, more effective antiviral treatment was associated with a 12% decrease in the use of corticosteroids as well as a decrease in the use of other immunosuppressive agents6.
It is also worthwhile to consider that the latest addition to the therapeutic options in HCV-induced MC vasculitis, the anti-CD20 monoclonal antibody rituximab, is an immunosuppressive agent, albeit specific to the B cell compartment. Although we and others have described its efficacy in refractory HCV-induced MC vasculitis34–39, and it is largely considered a safe treatment40–43, there have been reports linking its use with infectious complications44–49.
Our study has several important limitations, including its retrospective design. This is relevant in particular to the determination of the actual cause of death, which may result from several factors in an acutely ill patient. We may have underestimated the contribution of vasculitis itself, as patients receiving immunosuppressive drugs were those with a more severe form of vasculitis. In addition, the relatively small number of patients may limit the analysis; however, considering the rare incidence of this illness we have presented a relatively large group.
Our study demonstrated how evolving trends in available therapeutic options affected the causes of death in MC vasculitis, as well as prognostic factors predicting mortality. While renal disease as a cause of death has significantly decreased, infection and immunosuppressive treatment now have a significant influence on mortality associated with MC vasculitis. Development of more effective anti-HCV agents may further affect the natural history of this severe illness.
Footnotes
- Accepted for publication October 6, 2009.








{kind=link}