

Abstract
Objective. To determine factors associated with work in patients with ankylosing spondylitis (AS).
Methods. Three hundred fifteen patients with AS were enrolled in a 24-week, randomized controlled study of adalimumab with a longterm, open-label, adalimumab extension phase. Patient-reported outcome (PRO) measures included the Medical Outcome Study Short Form 36 Health Survey (SF-36), AS Quality of Life Questionnaire (ASQOL), Health Utilities Index Mark 3 (HUI-3), and Work Productivity and Activity Impairment-Specific Health Problem Questionnaire (WPAI-SHP). Multivariate logistic regression was used to analyze differences between working and nonworking patients. The relationships between PRO and WPAI-SHP scores were assessed using Pearson correlation coefficients. Multivariate modeling was applied to determine factors associated with productivity while at work. WPAI-SHP was assessed through 3 years of adalimumab exposure.
Results. Younger age (p = 0.002) and male sex (p < 0.001) were significantly and independently associated with working patients with AS. The SF-36 Physical Component Summary score (p < 0.001), ASQOL score (p < 0.001), HUI-3 scores (p < 0.001), and both patient’s global assessment of disease activity (p < 0.001) and nocturnal pain (p < 0.001) scores were independently associated with working status. Work absenteeism due to AS was weakly correlated with all PRO scores. WPAI-SHP components of work presenteeism (lack of productivity at work), activity impairment, and overall work productivity loss due to AS were moderately correlated with quality of life as measured by the ASQOL, the SF-36 Physical Component Summary score, and the SF-36 Bodily Pain domain. Linear multivariate analyses indicated that work presenteeism was significantly associated with pain, functioning, and disease activity. Longterm adalimumab treatment was associated with sustained improvements in WPAI-SHP scores.
Conclusions. Quality of life and the physical consequences associated with AS have a direct relationship with a patient’s ability to work. Adalimumab sustains improvements in work outcomes in patients with AS.
- ANKYLOSING SPONDYLITIS
- ADALIMUMAB
- WORK PRODUCTIVITY
- PATIENT-REPORTED OUTCOMES
- HEALTH-RELATED QUALITY OF LIFE
- EMPLOYMENT STATUS
Ankylosing spondylitis (AS) is a chronic inflammatory rheumatic condition affecting the sacroiliac joints, the spinal column, and the peripheral joints1. Patients with AS have pain, morning stiffness, and gradual disability2. Population studies have reported the prevalence of AS to be between 0.5% and 1.6%; it is more commonly found in men than women3,4. The onset of the disease is generally between the ages of 20 and 40 years2, and the effects of AS are present for most of the patient’s life1,2. The onset and progression of AS typically occurs during income-producing years in a patient’s life, which can result in a significant burden for patients and their employers2,5. Because of a historical lack of effective, longterm therapy, this situation damages the health-related quality of life of many patients with AS5–7.
Because of the early onset and chronic nature of the disease, the lifetime costs and socioeconomic impairment to individuals with AS are substantial5,6,8. Work disability is an important socioeconomic outcome as it is associated with psychosocial and financial consequences for individual patients, as well as for society6. The withdrawal rates from work in patients with AS have been shown to be about 3 times greater than those in the general population9. It has also been reported that work-disabled patients with AS experience a significantly reduced quality of life9. The costs associated with loss of work productivity, also referred to as indirect costs in clinical studies, are a substantial component of the economic impact of chronic rheumatic diseases, including AS6,7. For example, a study by Boonen, et al6 in 2002 showed that lost work productivity due to AS was estimated to cost society approximately €3,595 (2008 US $4,900) per patient per year.
Work productivity is considered a critical factor in the strength and sustainability of any economy10. It is clear that time off from work (absenteeism) affects productivity; but even when employees are physically present in the workplace, they may experience decreased productivity (presenteeism) because of a specific condition such as AS, which decreases both the quantity and quality of their work10,11. When estimating the burden of employee illness, many employers focus on the cost of healthcare benefits, which is usually large and easily measured12. However, the effect of employee health on absenteeism and work performance and productivity is substantial. Studies of chronic conditions and certain health risk factors indicate that the costs of lost productivity can exceed the costs of medical care13. Thus, presenteeism can be very costly, particularly to employers12,13. Studies of presenteeism of patients with AS are limited6,14,15, and this is an important economic burden that needs to be addressed.
There have been major advances in the understanding of the pathogenesis of AS over recent years7,16–18. Several clinical trials have demonstrated the beneficial effects of tumor necrosis factor (TNF) blockade in the treatment of AS, with significant improvements in symptoms, function, and importantly, patients’ health-related quality of life14,16,17,19,20. Of the available TNF antagonists, adalimumab is the first fully human monoclonal antibody with a very high affinity for human TNF, and it has been demonstrated that TNF blockade by adalimumab is safe and effective in the treatment of patients with AS18,21,22.
The purpose of these analyses was to determine what demographic characteristics and health factors are associated with an AS patient’s ability to work. Because many patient-reported outcomes (PRO) have been shown to directly relate to the burden of AS23,24, a hypothesis of this study was that PRO variables are directly related to work productivity in patients with AS. Additional analyses were performed to test the hypothesis that factors that influence a patient’s working status (i.e., working vs not working) would differ from those affecting work presenteeism. The effect of 3 years of adalimumab treatment on work productivity in patients with active AS was also assessed.
MATERIALS AND METHODS
Data collection
Data were obtained from the Adalimumab Trial Evaluating Long-Term Efficacy and Safety in AS (ATLAS), a multicenter, randomized, double-blind, placebo-controlled clinical study conducted to assess the efficacy and safety of adalimumab 40 mg every other week in patients with active AS who have had an inadequate response to non-steroidal antiinflammatory drug (NSAID) therapy18. Enrolled patients were naïve to TNF-antagonist therapy. Active disease was defined as a Bath AS Disease Activity Index (BASDAI) score ≥ 4, a visual analog score (VAS) for total back pain ≥ 40 mm, and morning stiffness ≥ 1 hour. The complete study design and efficacy and safety results of ATLAS have been reported previously18. The current analyses use baseline data from all patients enrolled in the ATLAS study except for the analysis of adalimumab treatment’s effect on work productivity, which is based on duration of adalimumab exposure. However, retirees and homemakers were excluded from these analyses, as only employed patients (i.e., those working for pay) were included.
PRO measures
A PRO is a measure of health status that is reported by the patient. Several PRO measures were used as secondary endpoints in the ATLAS study. These PRO measures included the Medical Outcome Study Short Form 36 Health Survey (SF-36), which is a generic measure of physical and emotional health via 8 domains and 2 composite summary scores, the Physical Component Summary (PCS) and the Mental Component Summary (MCS)25; BASDAI, which rates disease activity based on questions pertaining to AS disease activity, including fatigue, spinal pain, joint pain, and morning stiffness26; the Bath AS Functional Index (BASFI), a disease-specific index to assess physical functional impairment due to AS27; the AS Quality of Life Questionnaire (ASQOL), which is a disease-specific quality-of-life measure28; total back pain and nocturnal pain, by VAS; the Health Utilities Index Mark 3 (HUI-3) score, a generic preference-scored tool for measuring quality of life and producing health utility scores29; and the patient’s global assessment of disease activity by VAS18.
Work Productivity and Activity Impairment-Specific Health Problem (WPAI-SHP) questionnaire
The WPAI-SHP questionnaire is a frequently used generic disease instrument that measures work productivity and activity impairment24. It is a quantitative measure of reduced productivity, both at work and during nonwork activities, that has been validated for measuring work impairment in a number of disease groups24,30. Results of the WPAI-SHP are expressed as a percentage of impairment, with greater percentages indicating greater impairment and less productivity. Patients were asked to recall work-specific situations in the past 7 days and then provide the following information: (1) percentage of work time missed due to AS (absenteeism); (2) percentage of impairment while working due to AS (presenteeism); (3) percentage of other activity impairment due to AS (i.e., activities outside of work); and (4) the overall percentage of work impairment due to AS (i.e., work productivity loss). The percentage of work time missed due to AS (absenteeism) is calculated as Q2/(Q2 + Q4) x 100%. The percentage of impairment due to AS while working (presenteeism) is calculated as Q5/10 x 100%. The percentage of activity impairment due to AS is calculated as Q6/10 x 100%. The percentage of overall work impairment (i.e., work productivity loss) is Q2/(Q2 + Q4) + (1–Q2/(Q2+Q4) x (Q5/10) x 100%. Detailed scoring methods for the four components of the WPAI-SHP are available at http://www.reillyassociates.net/WPAI_Scoring.html (accessed October 22, 2009).
Measure of comorbidities
The chronic disease score (CDS) is a validated and weighted method for measuring patient comorbidity status using prescription medication data31. The CDS was calculated for all patients using prescription medication reported at baseline. For the purposes of these analyses, all analgesic medications or other prescription medications taken by patients specifically for the management of their AS were eliminated from the CDS score for each patient.
Measures of disease activity
BASDAI scores, as described18, were used as an indicator of disease activity, as this score encompasses the key clinical features of AS, including fatigue, axial and peripheral disease, enthesitis, and morning stiffness26. In addition to the BASDAI scores, data were captured to identify, as a marker of disease state, those patients who had total spinal ankylosis before enrollment in the study. A diagnosis of total spinal ankylosis was determined by the patients’ physician. Duration of disease (in years) was also obtained from patients and used as a marker of disease state.
Analysis of differences between working and nonworking patients with AS
Potential associations of characteristics of patients with AS (baseline demographic and clinical characteristics, including AS disease activity and comorbidity status, and PRO measures) with working status were evaluated. Univariate descriptive statistics were used to show the distributions of working and nonworking patients with AS at study baseline. Independent Student t-tests were used to compare the differences for continuous variables and chi-square tests were used to compare categoric variables between working and nonworking patients. Patient working status was derived from the patient’s response to Question 1 of the WPAI-SHP questionnaire at baseline, "Are you currently employed (working for pay)?" Logistic regression models were developed to determine what independent factors were associated with a patient’s working status. The dependent variable was the patient’s working status (nonworking versus working). Because of the colinearity between the PRO instruments, each instrument was tested individually in separate logistic regression models while adjusting for other patient factors — age, sex, disease activity (BASDAI), and comorbidity status.
Correlation of baseline WPAI-SHP measures with baseline PRO measures in patients with AS
Only patients reported to be working at baseline were included in this analysis. Descriptive statistics were used to describe the overall responses to the WPAI-SHP summary scores. Correlation coefficients were calculated between all PRO and each WPAI-SHP summary score using Pearson correlation coefficient tests. All correlations were adjusted for age, sex, baseline disease activity (BASDAI), and comorbidity status. All coefficients were tested for statistical significance. Interpretation of the correlation coefficients was: 0.00–0.29 = little or no correlation; 0.30–0.49 = weak; 0.50–0.69 = moderate; 0.70–0.89 = strong; and 0.90–1.00 = very strong32.
Factors affecting work presenteeism
Only patients reported to be working at baseline were included in these analyses. Multivariate models were undertaken to determine what factors were independently associated with work presenteeism. Because the majority of patients (87.8%) reported some level of decreased work productivity at baseline, logistic modeling could not be applied; therefore, multivariate linear models were developed, with presenteeism scores defined as the continuous dependent variable. All PRO were tested individually in independent linear regression models while adjusting for other patient factors including age, sex, disease activity (BASDAI), and comorbidity status.
Effect of adalimumab on work productivity
WPAI-SHP scores were collected for all patients enrolled in ATLAS at baseline and after 24, 52, 76, 104, 128, and 156 weeks of adalimumab exposure. The mean change from baseline in WPAI-SHP scores for all patients treated with any dose of adalimumab was calculated for each of these time points. Only working patients were included in the analyses of absenteeism, presenteeism, and overall work productivity loss; all patients were included in the analysis of overall activity impairment.
For all analyses, missing data were excluded and the significance level was set at 0.05. All analyses were conducted using SAS Version 9.1 (Cary, NC, USA).
RESULTS
A total of 315 patients (75% male) were enrolled in the ATLAS study18. As reported, 288 patients (91.4%) entered the open-label extension phase of the trial, and 81.9% (236/288) had 3-year data (i.e., 3 years following baseline visit)33. Fifty-two patients enrolled in the extension portion of the trial but did not complete 3 years; of these 52, 17 discontinued because of adverse events.
Of the 315 enrolled patients, 205 (65.1%) reported working for pay at baseline. Of the 110 patients who were not working, 71.8% were men less than 65 years old. The mean baseline WPAI-SHP summary scores of patients working at baseline indicated that AS had considerable impact on all summary scores (Table 1). At baseline, patients had considerable impairment in work productivity. For example, these patients missed, on average, 3–4 hours of work per week because of the disease.
Baseline WPAI-SHP summary scores.
Differences in patient characteristics between working and nonworking patients with AS
Descriptive, univariate analyses showing differences in patient characteristics between working and nonworking patients at baseline are shown in Table 2. Patients with concomitant diseases and total spinal ankylosis were less likely to be employed; young men were more likely to be working. In addition, all PRO except for the SF-36 Mental Health domain and the SF-36 MCS score showed independent associations with working status at the univariate level. For each PRO instrument, patients reported to be working had scores indicating less disability and better quality of life. The duration of AS was not statistically associated with working status at the univariate level [p = 0.503; 95% confidence interval (CI) = –1.45, 2.96].
Differences in patient characteristics between nonworking and working patients with AS at baseline. Values are mean ± SD unless otherwise noted.
All multivariate analyses confirmed that age, sex, and comorbidity status were statistically significant independent predictors of patient working status. As expected, older patients were less likely to work than younger patients, and female patients were less likely to be employed than male patients. Patients with a concomitant disease were also less likely to be working. Multivariate analyses for each PRO showed that ASQOL (OR = 1.11; p = 0.001; 95% CI = 1.04, 1.18), BASFI (OR = 1.01; p = 0.050; 95% CI = 1.002, 1.020), SF-36 PCS (OR = 0.96; p = 0.021; 95% CI = 0.93, 0.99), HUI-3 (OR = 0.21; p = 0.002; 95% CI = 0.08, 0.57), nocturnal pain (OR = 1.02; p = 0.004; 95% CI = 1.01, 1.03), and total back pain (OR = 1.01; p = 0.023; 95% CI = 1.002, 1.03) were associated with patient working status while controlling for age, sex, comorbidities, and total spinal ankylosis status. BASDAI (OR = 1.01; p = 0.075; 95% CI = 1.00, 1.03) and SF-36 MCS (OR = 0.98; p = 0.138; 95% CI = 0.96, 1.01) did not have statistically significant associations with working status.
Correlation of WPAI-SHP measures with PRO measures in patients with AS
Of the 65.1% of working patients, missing data on work absenteeism and work presenteeism resulted in the exclusion of 15 and 11 patients, respectively, from the analysis. The results of the correlations between baseline WPAI-SHP summary scores and PRO measures are shown in Table 3.
Pearson’s correlation coefficients between WPAI-SHP summary scores and PRO at baseline.
The results showed that work absenteeism due to AS was weakly correlated with all PRO scores. Work presenteeism was moderately correlated with ASQOL, SF-36 PCS, SF-36 Bodily Pain domain, SF-36 Physical Functioning domain, BASFI, and the patient’s global assessment of disease activity, and was weakly correlated with all other PRO scores. Activity impairment due to AS was moderately correlated with diminished SF-36 Physical Functioning, SF-36 Role–Physical, SF-36 Bodily Pain, SF-36 PCS, ASQOL, BASDAI, BASFI, HUI-3 Overall, and the patient’s global assessment of disease activity. Activity impairment due to AS was weakly correlated with all other PRO scores. Overall work productivity loss due to AS was moderately correlated with SF-36 Physical Function, SF-36 Role–Physical, SF-36 Bodily Pain, SF-36 PCS, ASQOL, BASFI, and HUI-3. Overall work productivity loss due to AS was weakly correlated with all other PRO scores.
Factors affecting work presenteeism
Results of the linear multivariate model demonstrated statistically significant associations at baseline between work presenteeism and the components of the SF-36: Physical Functioning (p < 0.001), Role–Physical (p < 0.001), Bodily Pain (p < 0.001), General Health (p < 0.001), Vitality (p = 0.004), Social Functioning (p < 0.001), Role–Emotional (p = 0.001), and Mental Health (p = 0.006). Model findings also demonstrated associations between work presenteeism and the 2 summary scores of the SF-36 - PCS (p < 0.001), and MCS (p = 0.007) - as well as ASQOL (p < 0.001), HUI-3 overall (p < 0.001), BASFI (p < 0.001), BASDAI (p < 0.001), total back pain (p < 0.001), nocturnal pain (p = 0.001), and the patient’s global assessment of disease activity (p < 0.001). Interestingly, presenteeism in employed patients was not statistically associated with age, sex, or patient comorbidity status.
Impact of adalimumab treatment on work productivity
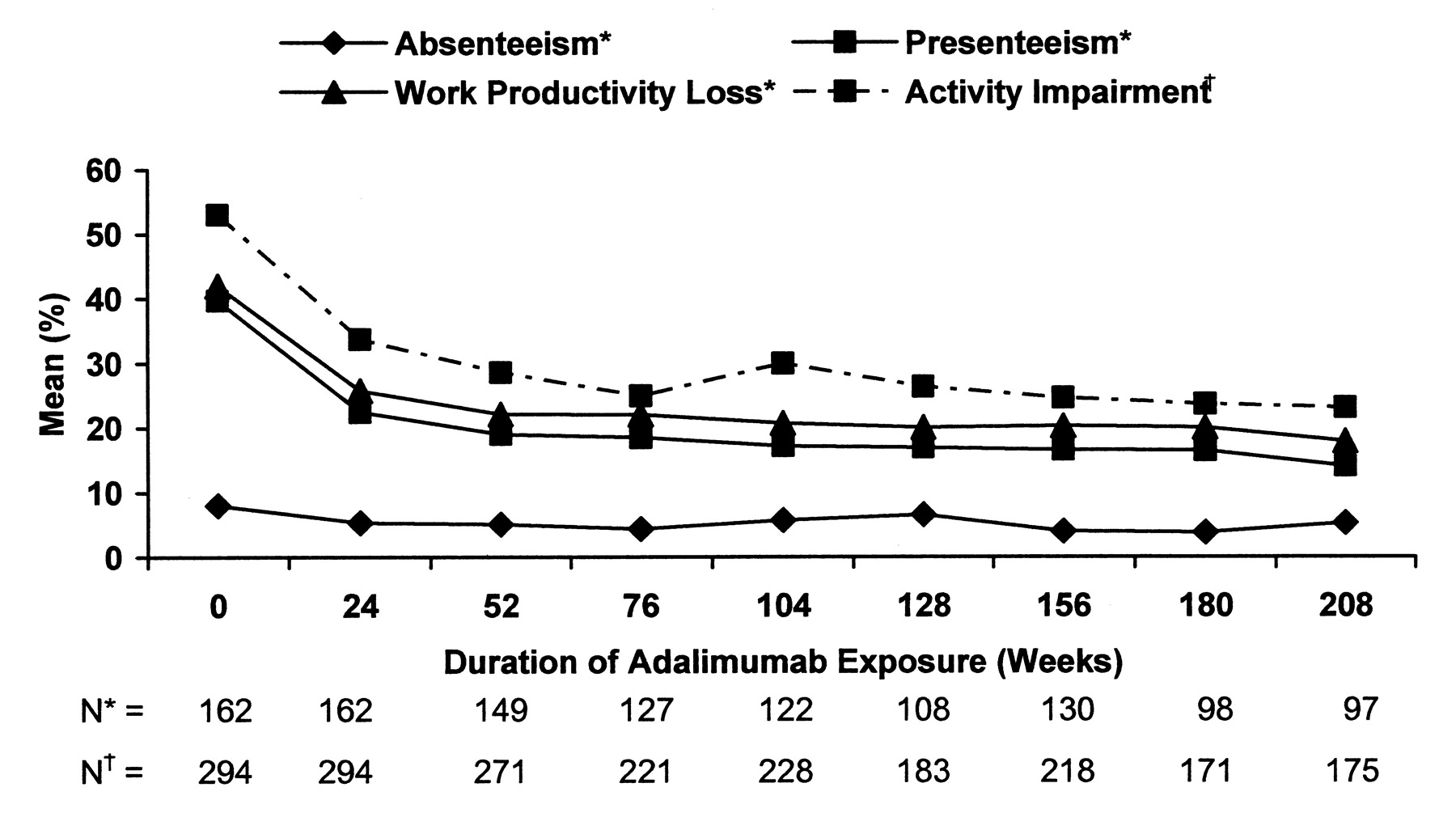
A reduction in WPAI-SHP score indicates an improvement in productivity. Sustained improvements for each WPAI-SHP item from baseline through 156 weeks of adalimumab treatment were observed for all patients treated with adalimumab (Figure 1). The mean change from baseline at Week 24 was –2.7% for absenteeism, –17.24% for presenteeism, –16.22% for overall work productivity loss, and –19.29% for activity impairment. At Week 156, the corresponding changes were –4.24%, –23.72%, –23.35%, and –29.37% for absenteeism, presenteeism, work productivity loss, and activity impairment, respectively. Based on a 40-hour work week for employed patients, a 4.24% reduction in work time missed (absenteeism) translates to 1.7 hours of work time gained per week; a 23.72% reduction in impairment (presenteeism) translates to 9.5 hours of improved performance per week; and a 23.35% reduction in work productivity lost translates to 9.3 hours of productivity gained per week compared with baseline values.

Mean percentage of absenteeism, presenteeism, work productivity impairment, and activity impairment through 4 years of adalimumab exposure. Data are as observed. *Only employed patients were considered for the first 3 items of the WPAI-SHP (absenteeism, presenteeism, and work productivity loss). †All patients, including unemployed patients, were considered for the fourth item of the WPAI-SHP (activity impairment). WPAI-SHP: Work Productivity and Activity Impairment-Specific Health Problem Questionnaire.
DISCUSSION
Overall, the use of adalimumab was effective in improving physical function and reducing the signs and symptoms of active AS that are the primary causes of reduction in work productivity in patients who have had an inadequate response to or intolerance of NSAID therapy18. The results demonstrated the sustained benefit and effectiveness of adalimumab in improving work productivity for up to 3 years (156 weeks), based on WPAI-SHP scores. With a 40-hour workweek assumed, a 32.6% lower overall work impairment for patients with AS treated with adalimumab is equivalent to 13 hours of increased productivity per workweek. Work impairment is even more pronounced for part-time workers.
Our findings are consistent with results of other studies that have demonstrated improvement in work productivity during anti-TNF therapy14,34,35. A 24-week randomized, placebo-controlled study of infliximab used a visual analog scale to assess the impact of AS on work productivity. Disease activity and functional impairment were both significantly associated with work productivity, and infliximab treatment was associated with a significant increase in work productivity and a reduction in workdays lost because of disability14. Similarly, other studies have shown a reduction in workdays lost when patients with AS are treated with TNF antagonists34,35.
Our analysis is unique because it is the first (to the authors’ knowledge and based on a review of the literature) to address the effect of physical function and quality of life on work productivity in patients with active AS during longterm anti-TNF therapy. The results of these analyses show that the PRO, including measures of poor physical function due to AS, were significantly correlated with working status and with work presenteeism. The striking result was that presenteeism and restrictions in unpaid work were actually more important than absence from paid work. As the PRO demonstrated weak correlations with absenteeism in employed patients, it is unclear whether societal pressures keep patients with AS at work or whether patients with AS with active disease acquire occupations best suited to accommodate the limitations of their disease as compared with the general population. Previous studies have alluded to the importance of contextual factors such as type of job (i.e., manual vs mainly intellectual, degree of job control and autonomy), educational level, income level, social security system, coping, and job satisfaction36,37.
The results of our study are useful and applicable in clinical practice for several reasons. First, although patients recruited for the ATLAS study were selected for high disease activity, these patients were otherwise typical of the general AS population in that they were young (99.1% = 65 years of age), predominantly male (74.9%), and predominantly HLA-B27 positive (78.8%)18. In addition, patients with AS and total spinal ankylosis were allowed to enroll, which is atypical of other AS clinical trials17,38.
This study, however, has limitations. First, recruitment was limited to patients with AS with baseline BASDAI scores of 4 (mean BASDAI score, 6.3). Therefore, these results may not be applicable to patients with AS with more mild disease. Second, although all patients enrolled in this study were naïve to TNF-antagonist therapy, they could receive other medications such as NSAID to manage the signs and symptoms of AS. The effects of such treatments were not assessed in these analyses; however, these concomitant AS drugs were deemed ineffective at study screening. For the purpose of this study, other demographic or PRO data (such as socioeconomic analyses) were not explored. In addition, the work-productivity analyses are based on observed data collected during a longterm study. Patients who may not have been responding to adalimumab treatment may have withdrawn during longterm treatment. Therefore, the potential for self-selection bias cannot be eliminated in this type of study design. Finally, since the WPAI was not implemented at Week 12, direct comparison of the effects of adalimumab vs placebo on work productivity could not be conducted. The study results, therefore, suggest but cannot prove that the improvements in WPAI observed in ATLAS were the direct result of adalimumab therapy.
One previous study in The Netherlands demonstrated that patients with AS withdraw from work 3 times more often than the general population9. Of note, The Netherlands has a social safety net that may not be representative of the rest of the world. A retrospective cost-of-illness study in patients with AS conducted in France determined that 74% of unemployed patients with AS were in the working-age population34 (i.e., ages 16–65 years)9. Of those, 20% were permanently work-disabled and 6.6% were temporarily disabled39. The inability to work or appropriately perform at work is therefore a devastating consequence of AS, both socially and economically6,7,39. One can assume that significant barriers exist for patients with AS who might want to reenter the workforce after being unemployed because of their underlying disease.
Results of our study indicate that there is a direct relationship between impaired quality of life and physical consequences of AS and patients’ working status and productivity while at work. These observed results suggest that such detriments to physical function and quality of life have a causal effect on ability to work. Therefore, for patients diagnosed with AS, timely intervention with treatments to minimize the symptoms associated with the debilitating disease, such as adalimumab, could potentially diminish the economic burden for working patients with AS and their employers.
Acknowledgments
We thank Dana L. Randall, MS, PharmD, of Arbor Communications, Ann Arbor, MI, and Michael A. Nissen, ELS, of Abbott Laboratories, Abbott Park, IL, USA, for editorial assistance in the development and revision of this manuscript.
Footnotes
-
Funded by Abbott Laboratories, Abbott Park, IL, USA. Assistance in editing and formatting this manuscript was funded by Abbott.
- Accepted for publication September 19, 2009.








{kind=link}