

Abstract
Objective. To ascertain the incidence, cumulative prevalence, persistence, and clearance of human papilloma virus (HPV) infection in patients with systemic lupus erythematosus (SLE), and to assess the risk factors for the acquisition and persistence of HPV infection.
Methods. One hundred forty-four patients with SLE were evaluated at 6-month intervals for up to 3 years. At each visit, a Pap test, a test for HPV DNA, and clinical assessment were performed.
Results. The cumulative prevalence of HPV infection increased significantly (12.5% at baseline to 25.0% after 3 years; p = 0.006). Regarding type-specific HPV infection, 18.8% patients experienced 68 incident infections. The cumulative prevalence of high-risk HPV infection (11.1% at baseline to 20.8% after 3 years; p = 0.02) and multiple HPV infection also increased significantly (6.9% at baseline to 16.7% after 3 years; p = 0.009). Half (33/68, 48.5%) of the incident infections persisted for ≥ 6 months. Overall, 29/32 (90.6%) of the preexisting infection and 10/68 (14.7%) of the incident infections were cleared. Independent risk factors associated with incident HPV infection included younger age at first sexual intercourse (p = 0.025) and baseline Systemic Lupus International Collaborating Clinics score ≥ 1 (p = 0.038). Independent risk factor associated with persistent HPV infection included preexisting HPV infection (p = 0.04) and multiple HPV infection during first incident infection (p = 0.02).
Conclusion. High frequency of persistent HPV infection, especially high-risk and multiple HPV infection, may explain why squamous intraepithelial lesions occurred frequently in patients with SLE. Patients with high inflammatory burden are at risk of acquiring HPV infection.
The prevalence of an abnormal Pap smear1–5 and possibly cervical cancer6 was significantly increased in patients in our study with systemic lupus erythematosus (SLE) compared with healthy controls. The contribution of human papilloma virus (HPV) infection to the pathogenesis of cervical cancer is well established7. The identification of viral and nonviral factors that influence the acquisition and persistence of cervical HPV is necessary to further our understanding of HPV-related carcinogenesis. Persistent high-risk (HR) HPV infection is an important factor in the development of cervical cancer8. Risk factors for persistent HPV infection included hormonal status (estrogen levels), oral contraceptive use, menstruation and/or menopause status, smoking, age, genetic and epigenetic factors and coinfections with other microorganisms, infection with multiple types of HPV, and infection with an HR type9,10. Although the association between persistent infection and multiple types of HPV is not well established, some evidence suggests that women who have multiple types might have certain characteristics, e.g., deficient immune response to HPV that predisposes them to persistent infection11. In patients who have the human immunodeficiency virus (HIV)12, persistent infection was associated with the degree of immunosuppression, as reflected by a low CD4 count. We have reported that patients with SLE are at risk of having multiple infections4. If SLE-related immunosuppression causes persistent HPV infection, this effect may promote the development of squamous intraepithelial lesions (SIL) and cancers in SLE. Information about the natural history of HPV infection in SLE is lacking. Whether immunosuppression related to SLE itself and/or the use of immunosuppressant would result in an increased incidence and risk of persistent HPV infection similar to patients with HIV has never been studied.
We aimed to ascertain the incidence, cumulative prevalence, persistence, and clearance of HPV infection in patients with SLE, and to assess the association among social, demographic, gynecologic, lifestyle, clinical measurements, and the use of immunosuppressants and the risk of acquisition and persistence of HPV infection in patients with SLE.
MATERIALS AND METHODS
One hundred fifty consecutive female patients attending the lupus clinic at the Prince of Wales Hospital who fulfilled the 1997 American College of Rheumatology revised criteria for the classification of SLE13 were recruited for our prospective cohort study. Patients were eligible for the study if they were married or sexually active. Pregnant patients were excluded from the study. None of the patients had received HPV vaccine before. All patients were invited to return for reassessment every 6 months for a total of 3 years. The first visit included a structured interview using a standardized questionnaire covering sociodemographics, lifestyle, and medical and reproductive history. Prior use of immunosuppressants was retrieved by chart review. The Systemic Lupus Erythematosus Disease Activity Index (SLEDAI)14 and the Systemic Lupus International Collaborating Clinics (SLICC)15 were used to indicate disease activity and damage, respectively. At each visit, a Pap test and HPV testing were performed and drug history was recorded. All women with abnormal Pap smears were referred for gynecologic followup (Appendix). Patients with high-grade lesions [high-grade SIL (HSIL) or above] at baseline were excluded from the analysis of incident HPV infection. Patients treated with loop electrosurgical excision procedure (LEEP) or colposcopy with cervical biopsy were excluded from analysis of the persistence and clearance of HPV infection.
The Ethics Committee of the Chinese University of Hong Kong approved this study, and all patients provided written informed consent.
HPV sampling procedure and identification
The method of cervical sample collection, detection, and identification of HPV have been described16. Briefly, a cervical sample was collected with a Cervex brush (Rovers Medical Devices) from each woman for routine liquid-based cytologic examination. After cytologic examination, the remaining sample was used for HPV DNA detection. DNA was extracted as described17. HPV DNA detection was by the PGMY polymerase chain reaction (PCR) targeting the consensus region of the HPV L1 gene18. Serial dilutions of recombinant plasmids containing the whole genome of HPV-6, -11, -16, and -18 were used to estimate the analytic sensitivity of the PCR. The amplification reactions allowed for consistent and reproducible detection of ≥ 50 copies of these HPV genomes. Samples tested positive for HPV DNA were subjected to HPV typing using the Linear Array HPV Genotyping Test that can detect 37 HPV types. HPV are classified into HR, probable HR, low risk, and unknown risk based on their epidemiological risk for cervical cancer development19–21. For the purpose of analysis in this study, HPV types were grouped as HR (including those with probable HR) and low-risk (LR; including those with unknown risk).
Definition of HPV infection
Preexisting infection was defined as any positive HPV type(s) detected in the first visit sample. Incident HPV infection was defined as an HPV genotype not identified on a previous visit. For the incident infections, transient infection was defined as any HPV type that was detected only at 1 visit, followed by 2 or more negative samples. Persistent infection was defined as the detection of the same type of HPV at 2 or more subsequent examinations (≥ 6 months apart). If a woman tested positive, negative, and then positive for the same HPV type over 3 consecutive visits, the infection was considered to be persistent with an intercurrent false-negative result22. Clearance of the type-specific infection (including preexisting, incident, or persistent infections) was defined as the HPV type that was detected at any visit, followed by 2 or more negative samples. Multiple infections was defined as > 1 HPV type detected in 1 or more visits. For the purpose of study analysis, subjects were grouped to the worst category, i.e., subjects with both transient and persistent infection were considered to have persistent infection.
Statistical analysis
Results are expressed as mean ± SD for normally distributed data. Non-normally distributed data are expressed as median (interquartile range). The incidence of new infections was defined as the number of newly detected HPV infections after 1 or more negative tests, divided by the total number of followup visits per woman-month. For the type-specific infection, time to acquisition was defined as the time of the positive test result. The time to clearance was defined as the duration from baseline for patients with preexisting infection, or the first visit when an incident infection was detected, to the first visit when the HPV infection was negative. The duration of persistent HPV infection was defined as the duration between the onset of incident infection to the first visit when the HPV was negative or the last visit if the infection continued to persist. The Kaplan-Meier method was used to construct a cumulative acquisition curve to calculate median [95% confidence interval (CI)] time to acquisition, and the duration until clearance of HPV infection.
The differences between the baseline and cumulative prevalence of HPV infection over 3 years are compared by the z-statistics23. The associations among social, demographic, lifestyle, gynecologic, clinical variables, the use of immunosuppressants, and the risk of incident and persistent HPV infection were examined by univariate analysis. In addition, viral factors and the risk of persistent infection were examined. Chi-squared tests were used for categorical variables. For continuous variables, Student’s t test and Mann-Whitney U tests were used where appropriate. All the risk factors identified in the univariate analysis with p < 0.1 were entered into regression analysis (backwards, Wald). SPSS for Windows, version 13.0, 2006 (SPSS Inc., Chicago, IL, USA), was used for the analyses.
RESULTS
Baseline social, demographic, and clinical characteristics
The cohort was composed of 150 women with SLE. The mean age was 41 ± 9 years and 55 (36.7%) were postmenopausal; 114 (76%) were married. The mean disease duration was 8.6 years (range 4.6–14.4). Except for the significantly higher prevalence of nephritis (59% vs 50%; p = 0.01), the clinical and immunological profile (ever) of patients recruited in this study was similar to other patients followed in the same clinic (Table 1).
The clinical features according to the definitions of the American College of Rheumatology criteria and immunological profiles (ever) of patients with SLE recruited in this study were similar to the rest of the patients in the cohort. The treatment variables on patients not having a Pap smear were not available. “Ever” refers to use of immunosuppressants since the diagnosis of SLE.
Preexisting cervical HPV infection
HPV DNA was detected at the initial examination in 20/150 (13.3%) patients with SLE, with a total of 38 HPV infections. Thirty of the 38 (78.9%) were HR HPV infections. The prevalence of HR and multiple HPV infections was 12% (18/150) and 6.7% (10/150), respectively. Five women did not have a second HPV test, and 1 of them had positive HPV-16. One patient who had HSIL with positive HPV-16 was excluded from analysis.
Incidence and cumulative prevalence of cervical HPV infection
One hundred forty-four (96.0%) women with at least 2 HPV tests done were included in the analysis for the incidence of HPV infection. The median followup duration was 30.8 (range 26.1–31.7) months, with a total followup duration of 4001 patient-months. The median number of visit was 5 (range 4–5) per patient. Six (4.2%) patients had atypical squamous cell of unknown significance (ASCUS) and 7 (4.9%) patients had low-grade SIL (LSIL) at baseline.
The cumulative prevalence of HPV infection increased significantly after 3 years (12.5% at baseline to 25.0% after 3 years; p = 0.006; Figure 1). Twenty-seven (18.8%) patients experienced a total of 68 incident infections (Tables 2A and 2B). The risk of acquiring any HPV infection in this cohort was 17.0 per 1000 patient-months.

Baseline and cumulative prevalence of human papilloma virus infection.
Prevalence at enrollment and incidence rate of high-risk cervical HPV infections in 144 patients with SLE.
Prevalence at enrollment and incidence rate of low-risk and overall HPV cervical infections in 144 patients with SLE.
The cumulative prevalence of HR HPV infection increased significantly after 3 years (11.1% at baseline to 20.8% after 3 years; p = 0.02) while the cumulative prevalence for LR HPV infection remained similar (p = 0.15; Figure 1). The rate of acquiring HR HPV infection was twice as high as that of LR HPV infection (11.5 and 5.5 per 1000 patient-months, respectively).
The cumulative prevalence of multiple HPV infections also increased significantly after 3 years (6.9% at baseline to 16.7% after 3 years; p = 0.009; Figure 1). Out of the 25 patients who had multiple HPV infections, 18 (72%) had multiple infections during the first incident infection. The majority of the incident infections (59/68, 86.8%) were multiple infections. The risk of multiple infections in HR HPV was increased compared to LR HPV (43/46 and 16/22, respectively; p = 0.049). The maximum number of HPV types detected at 1 visit was 7, and 50% of the coinfection involved 3 or more HPV types. Among patients who tested positive for HPV, 64.9% harbored multiple HPV types.
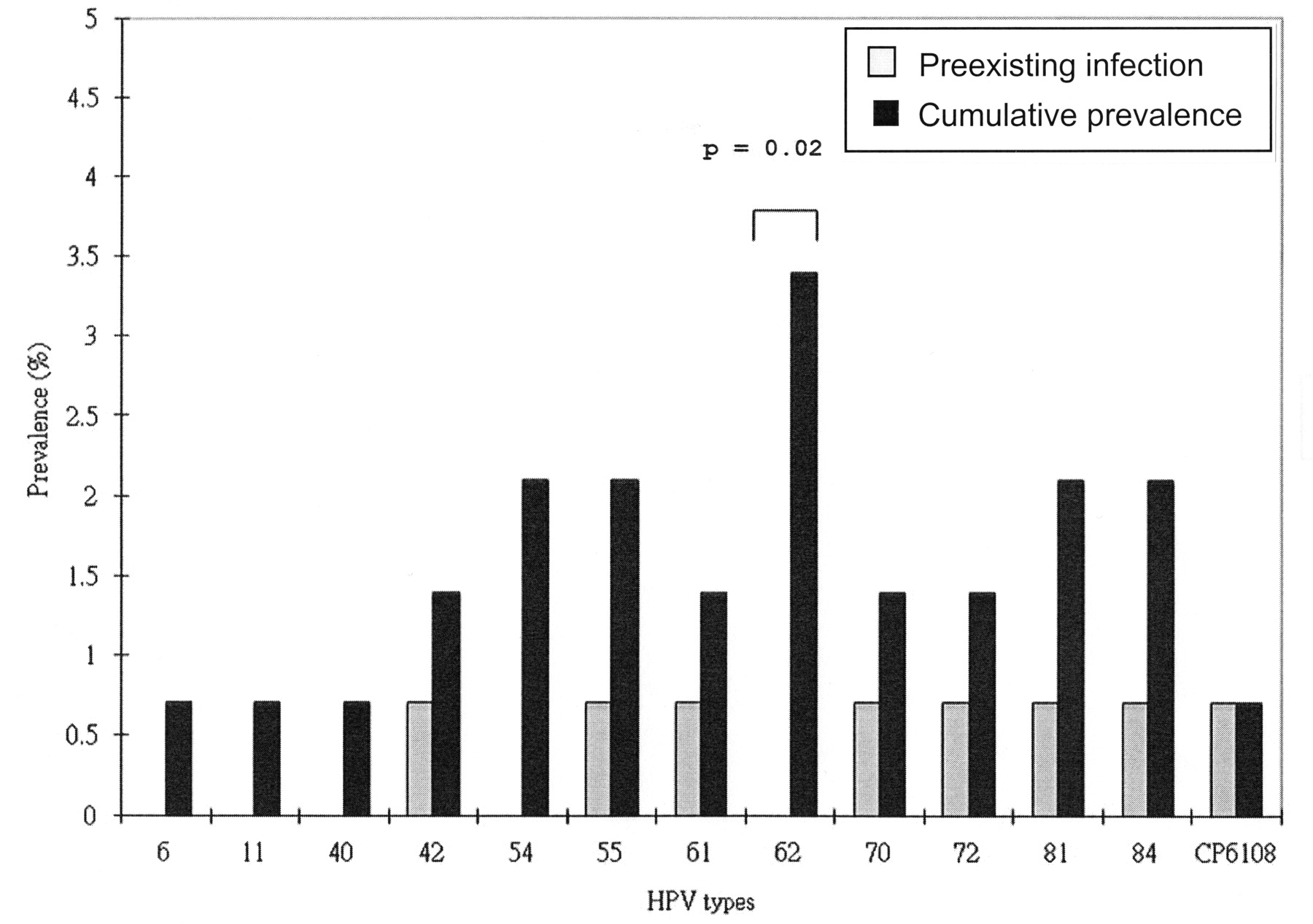
Figures 2 and 3 summarize the baseline and cumulative prevalence of the HR and LR HPV infection, respectively. The most common newly acquired HR types were HPV-16 and 52 (1.7 per 1000 patient-months), followed by HPV-18 and 58 (1.2 per 1000 patient-months; Table 2A). The cumulative prevalence of HPV-62 increased significantly after 3 years (p = 0.02; Figure 3).
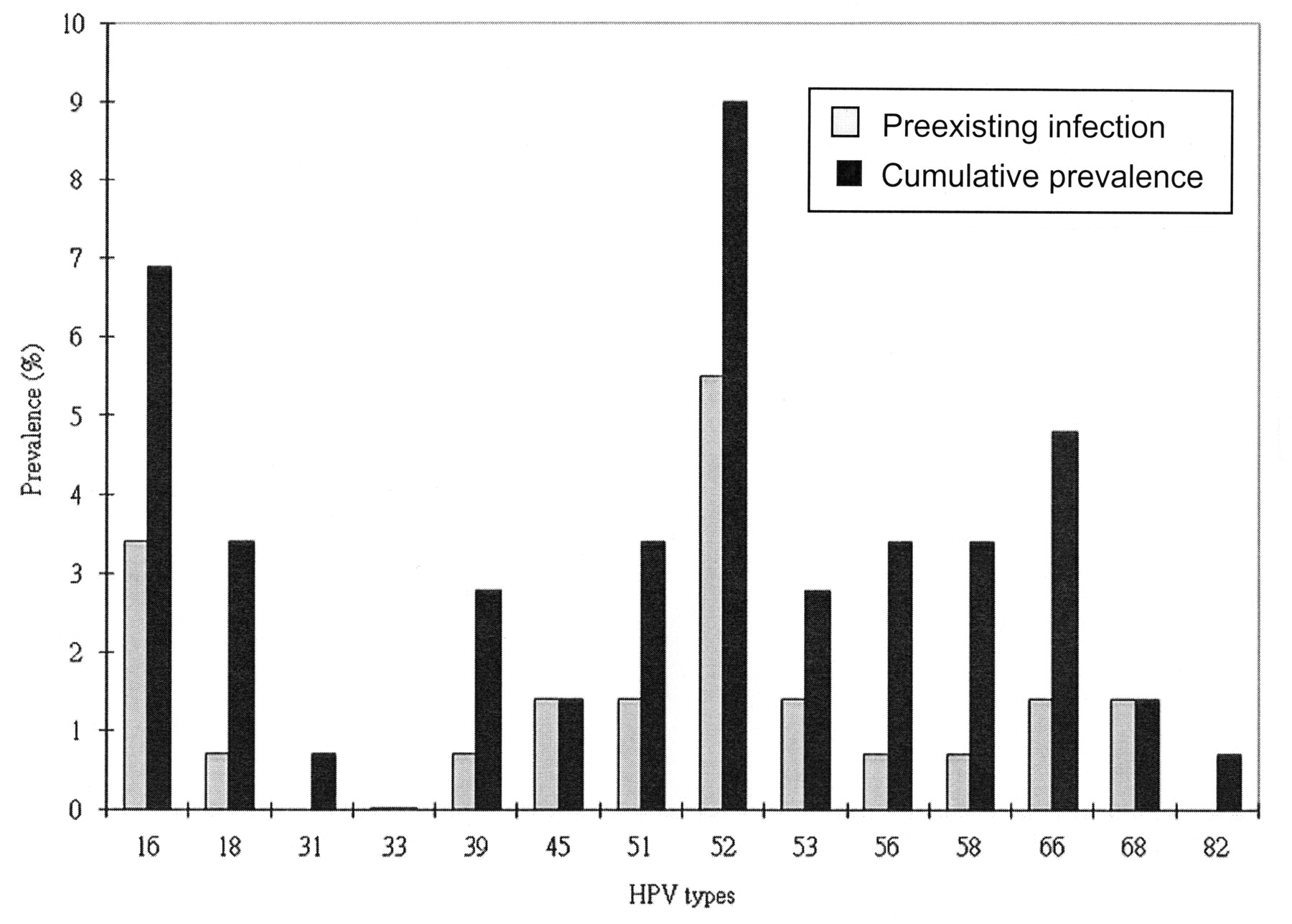
Baseline and cumulative prevalence of high-risk human papilloma virus infections.

Baseline and cumulative prevalence of low-risk human papilloma virus infections.
Acquisition, persistence, and clearance of HPV infection
The time to acquisition of LR HPV was significantly shorter than HR HPV (p = 0.007; Table 3). For the preexisting infections, 4 HPV infections in which LEEP or cervical biopsy was done were excluded from analysis of persistence and clearance. Almost half (48.5%) of the incident infections persisted (Table 3).
Potential risk factor that may affect the time to acquisition, persistence, and clearance of HPV infection.
By 12 and 24 months, 22/32 (68.8%) and 27/32 (84.4%) of the preexisting infections were cleared, respectively. For the incident infections, 26/68 (38.2%) infections acquired during the last 2 visits had undetermined outcome. By 12 months, 13.2% of the incident infections were cleared.
Infections that persisted for ≥ 6 months had a lower clearance rate and longer time for clearance than those without persistence. The persistence rate, clearance rate, and the time to clearance were not affected by the risk type and the presence of multiple infections (Table 3).
Baseline risk factors for incident HPV infection in SLE
Potential risk factors associated with incident HPV infection included younger age at first sexual intercourse (p = 0.024), number of lifetime sexual partners ≥ 3 (p = 0.019), SLICC score ≥ 1 (p = 0.009), the use of cyclophosphamide ever (p = 0.059), and current use of leflunomide (p = 0.05; Table 4). The risk of acquiring HPV was also associated with a longer duration of followup (30.4 ± 4.1 months vs 27.4 ± 6.8 months; p = 0.004) but not with the number of visits (4.9 ± 0.9 vs 4.7 ± 1.0; p = 0.3) during this study period. Independent risk factors associated with incident HPV infection included younger age at first sexual intercourse (OR 0.87, 95% CI 0.77–0.98) and baseline SLICC ≥ 1 (OR 2.62, 95% CI 1.05–6.51).
Unadjusted odds ratio (OR) for potential risk factors for incident or persistent HPV infections in patients with SLE.
Risk factors for persistent HPV infection
Nine of the 144 (6.3%) patients treated with LEEP or cervical biopsy were excluded from analysis. Sixteen of the remaining 135 (11.9%) patients experienced ≥ 1 episode of persistent infection. Potential risk factors associated with persistent HPV infection (ever) included younger age at first sexual intercourse (p = 0.062) and number of lifetime sexual partners ≥ 3 (p = 0.025; Table 4). HPV status associated with persistent HPV infection included (all p values < 0.001) preexisting infection, HPV ever, multiple HPV infections at baseline, at first incident infection, or ever; and HR HPV at baseline or ever (Table 5). The risk of having persistent HPV was also associated with the duration of followup (30.7 ± 2.3 months vs 27.7 ± 6.7 months; p = 0.001) and the number of visits (5.1 ± 0.7 vs 4.7 ± 1.0; p = 0.059) during this study period. Independent risk factors associated with persistent HPV infection included preexisting infection (OR 11.4, 95% CI 1.2–111.4) and multiple HPV infections at first incident infection (OR 14.0, 95% CI 1.4–135.9).
The association between HPV status and the development of persistent HPV infection (ever) in SLE.
DISCUSSION
This is the first prospective study looking at the natural history of HPV infection in patients with SLE. An important finding of this study is that in patients with SLE, the cumulative prevalence of HPV infection, including HR HPV and multiple HPV infections, increased significantly over time.
Compared to other studies in younger cohorts of healthy women (mean age 18–33 years, 9.8–19.0 per 1000 patient-months9,24–27), the rate of acquisition of new infections for any HPV type appeared similar or even higher in our patients with SLE (mean age 41 years, 17.0 per 1000 patient-months). In our study, the cumulative prevalence of HPV infection after a median of 5 examinations was 25.0%. This cumulative prevalence was considerably higher than the point-prevalence in our previous study4. Studies that have tested patients with SLE for HPV infections on a single occasion may have considerably underestimated the prevalence of such infections. Our study clearly indicates that infections continue to appear throughout the 3 years of followup, mainly because of increased incidence of HR HPV infection. The apparent increase in infection rate may be related to vaginal dryness. Twenty-eight (19.3%) patients with SLE in this cohort had secondary Sjögren’s syndrome, and 55 (36.7%) were postmenopausal. Vaginal dryness as a result of these conditions could potentially increase their risk of microtrauma and viral entry during heterosexual intercourse. Further, we cannot unequivocally differentiate an incident infection from a reactivation of a prevalent or latent infection. Although there are no well controlled studies to support reactivation, it seems to occur when immunocompetent patients undergo immunosuppressive challenges, such as during chronic steroid use or chronic illness. In celibate women with HIV, CD4 T-cell count was strongly associated with newly detected HPV types, presumably reactivation of (latent or quiescent) HPV that had been previously acquired28.
Based on data from healthy subjects, the cumulative incidence of HR HPV infection was similar to the LR types9,24,25,27. In contrast, we noticed a 2-fold increase in the overall incidence of HR HPV infection compared to the LR type. The cumulative prevalence of HR HPV was higher than that of LR HPV because the majority of the incident infections (59/68, 86.8%) were multiple infections, and the majority of the multiple infections (43/59, 72.9%) consisted of HR HPV. The interaction between distinct HPV types may influence the acquisition and clearance of cervical infection24,29.
Other studies on healthy women found that 19%–38% of those who tested positive for HPV harbored multiple HPV types27,30. Such prevalence is much lower than that observed in our lupus cohort (64.9%). Moreover, the risk of coinfection was much higher in HR than in LR HPV in our patients. The observed association could be explained by shared risk factors, or differential type-specific host susceptibility. In immunocompromised hosts such as patients with HIV12, the cumulative prevalence of HR HPV was also increased compared with the LR types.
In our study, coinfection of HPV with multiple types did not affect the acquisition, persistence, and clearance of the HPV infection. Results from other studies are mixed, in part because the time between cervical HPV sampling and the definitions for persistence vary between studies. Some reported that viral clearance was significantly delayed by multiple HPV types detected in a previous visit9,31, although this finding was not confirmed in other studies24,25,30.
Studies of the natural history of cervical HPV infection showed that most incident infections were transient, lasting < 6 months9,24. In subjects with either ASCUS or LSIL at baseline, 37% of the newly observed HPV infection persisted for 6 months32. In contrast, the rate of persistent infection in our subjects with SLE appeared increased (48.5%). Studies have suggested that a woman is likely to lose her existing HPV infection if it was newly acquired, and the longer an infection persisted the more difficult it was to lose it9,32. Results from this study also concur with this observation since the only determinant for the time to clearance was whether the infection had persisted.
We noticed that patients with a high inflammatory burden as reflected by a SLICC score ≥ 1 were at higher risk of acquiring HPV infection, after adjusting for the known risk factors as well as the use of immunosuppressants. Failure to induce an effective cellular immune response because of inefficient activation of innate immunity and ineffective priming of the adaptive immune response in patients with lupus may lead to an increased prevalence as well as persistence of any viral infection, including HPV infection. Patients with SLE are known to have impaired cellular and innate immunity, e.g., mannose-binding lectin gene polymorphism, which was associated with a higher risk of infection as well as more major lupus exacerbations33.
In healthy young females, infection with HR types and multiple infections were risk factors for persistent infection9. Similarly, patients with SLE with multiple infections during the first incident infection are at risk of having persistent infection, since 75% of the patients who had multiple infections had coinfection during the first incident infection. Unlike in healthy women, patients with lupus with any HPV infections at baseline are at risk of having persistent infection regardless of risk type. In subjects with HIV, both HIV seropositivity and higher levels of immunosuppression were important determinants for persistent HPV infection12. In our patients with lupus, it would be more difficult to quantify the degree of immunosuppression. After adjusting for the host factors and the use of immunosuppressants, the viral factor probably played a more important role for viral persistence.
The prior use of immunosuppressants, e.g., cyclophosphamide, was associated with an increased risk of incidence infection only in the univariate analysis. This could potentially reflect the disease severity, since these drugs are usually given to patients with major organ involvement, and therefore the association is lost after adjusting for a disease severity marker, e.g., the SLICC. We did not have information on the cumulative dose of immunosuppressants used since the diagnosis of SLE. Whether a higher cumulative dose of cyclophosphamide is an independent risk factor associated with an increased risk of infection could not be ascertained in our study. Future prospective studies with larger sample sizes and longer followup duration would be required to formally assess the risk of HPV infection and the use of immunosuppressants.
Five of 44 (11.3%) persistent infections had an intercurrent false-negative result. There could be multiple reasons for such false-negative findings. The most likely reason was variation in virus shedding over time. The sample quality was unlikely to be a cause of concern as the specimen quality was checked by amplifying a housekeeping gene, as well as by cytological examination of the samples. The assay used was one of the highly sensitive methods commonly used for detecting HPV from clinical samples. Based on the existing criteria, incident infections that were detected only at the next-to-last visit, and persistent infections that were detectable up to the next-to-last visit, will not fulfill the criteria of clearance. Therefore, the total number of transient infections and cleared infections may be underestimated.
The main limitation of our study is the lack of a healthy control group. Whether the natural history of HPV infection in patients with SLE is different from controls would need to be addressed in a future study. Moreover, the majority of our patients did not belong to the highest-risk age group. Further research is also needed to understand the natural history of HPV in other lupus populations with different ethnic and socioeconomic backgrounds. Studies have speculated that disease activity may be as important as or more important than disease therapy in increasing the risk for lymphoma in RA and SLE34,35. Unfortunately we did not have data on the disease activity since the diagnosis of SLE. It would be of interest for future study to include a measure such as average mean SLEDAI since disease onset as a potential predictor of incident or prevalent HPV infection. Finally, the relationship among HPV acquisition, persistence, and clearance and the change in lupus activity and medications would need to be examined by time-dependent proportional-hazards regression analysis. This could only be done in a larger group of patients followed for a prolonged period of time with a larger event rate.
This natural history study adds to the sparse data on cervical HPV infection in immunocompromised women. The high frequency of persistent HPV infection, especially HR and multiple HPV infection, may explain why SIL occurred frequently in patients with SLE.
APPENDIX
Colposcopy (Colpo) followup for subjects with abnormal cytology results. Colposcopy was performed within 2 months if the Pap smear (PS) results fulfilled the following criteria: Abn: abnormal; ASCUS: atypical squamous cell of unknown significance; LGSIL: low grade squamous intraepithelial lesion (SIL); HGSIL: high grade SIL; CIN: cervical intraepithelial neoplasia; LEEP: loop electrosurgical excision procedure. 6/12 = 6 months; 2/12 = 2 months.
Footnotes
- Accepted for publication September 29, 2009.








{kind=link}
{kind=link}
{kind=link}