

Abstract
Objective. To compare health-related quality of life (HRQOL) of patients with rheumatoid arthritis (RA) to that of the general population and to investigate the association with disease activity, focusing on different clinical remission criteria.
Methods. EQ-5D data from 3156 patients with RA from 11 Danish centers were compared with Danish EQ-5D population norms (n = 16,136). The Disease Activity Score (DAS28) and the Clinical Disease Activity Index score (CDAI) were used as definitions of disease activity and clinical remission. The score difference (ΔEQ-5D) was calculated in each patient as the difference from the age and sex-matched general population and adjusted for age, marital status, education, body mass index, smoking, exercise habits, disease duration, IgM-rheumatoid factor status, joint surgery, extraarticular features, treatment, and comorbidity in multiple linear regression models.
Results. 37% vs 22% fulfilled the DAS28 and CDAI remission criteria, respectively. The ΔEQ-5D values for women/men in clinical remission were DAS28 0.05/0.06 vs CDAI 0.01/0.02; low disease activity: DAS28 0.12/0.13 vs CDAI 0.11/0.14; moderate disease activity: DAS28 0.18/0.20 vs CDAI 0.20/0.23; and high disease activity: DAS28 0.38/0.28 vs CDAI 0.33/0.26. Adjusting for confounders reduced the ΔEQ-5D values between 0 and 0.04 units.
Conclusion. Patients with RA had worse EQ-5D scores than the general population, and the difference was strongly associated with disease activity. The EQ-5D score for patients in clinical remission approached that of the general population, suggesting that strict treatment goals are critical in order to achieve near-normal HRQOL in patients with RA.
- RHEUMATOID ARTHRITIS
- CLINICAL REMISSION
- DISEASE ACTIVITY SCORE
- CLINICAL DISEASE ACTIVITY INDEX
- HEALTH-RELATED QUALITY OF LIFE
Rheumatoid arthritis (RA) is a chronic disabling disease affecting physical, mental, and social aspects of patients’ lives, and current treatment for RA aims at clinical remission and improved health-related quality of life (HRQOL). Clinical remission is frequently defined as the Disease Activity Score based on a 28-joint count (DAS28) below 2.6, but several other definitions exist1–3. Recent work has reported that remission rates vary with different definitions of remission, DAS28 providing the most liberal definition4,5. HRQOL is measured by instruments that identify different aspects of health, disease, and the consequences from the patient’s perspective.
The EQ-5D is a generic HRQOL instrument that may be used in economic evaluations of the influence of various diseases6. Few EQ-5D data have been published for patients with RA, however7,8.
A number of RA studies have provided evidence of progression of joint damage despite apparent clinical remission9–11, suggesting that the latter may not necessarily be associated with a good outcome in other important measures, such as HRQOL. Previous studies using different HRQOL instruments have shown that RA is associated with poor HRQOL compared to the general population7,12–14. However, the impact of disease activity, especially the specific influence of clinical remission, on HRQOL has not been determined. Further, as remission rates vary according to remission criteria4, it is possible that HRQOL will vary accordingly.
Thus, our aims were to compare the HRQOL (measured by EQ-5D) of a large sample of RA patients with an age and sex-matched general population, and to explore the association between disease activity and HRQOL, focusing on different clinical remission criteria.
MATERIALS AND METHODS
Patients and data collection
A cross-sectional study involving 11 Danish outpatient rheumatology clinics was undertaken from July 2006 to July 2007. Patients with a diagnosis of RA as defined by the ACR 1987 criteria were eligible for inclusion. No exclusion criteria were specified. Clinical and patient-reported data were registered by the physicians and patients on separate forms during routine visits in the clinic. Reasons for nonparticipation were recorded. Clinical data included disease duration, disease activity [swollen and tender joint counts (0–28) (SJC28, TJC28), serum C-reactive protein (s-CRP), physician’s global assessment on a visual analog scale (VAS)], disease severity [presence of IgM-rheumatoid factor (IgM-RF), joint erosions on conventional radiographs, and rheumatic nodules], and treatment [i.e., disease modifying antirheumatic drugs (DMARD), biological antirheumatic drugs (BARD), and glucocorticoids]. Patient-reported data included sociodemography (sex, age, marital status, education), lifestyle factors [smoking, body mass index (BMI), and exercise habits], and disease-related factors [patient’s global RA assessment VAS, Health Assessment Questionnaire (HAQ) value, extraarticular features, joint surgery, and the presence of comorbidity from a list of 17 chronic diseases]. Finally, the validated Danish EQ-5D was completed15. All data were subsequently registered in the nationwide Danish Danbio registry16.
EQ-5D
The EQ-5D is a generic preference-based health status instrument including 5 dimensions of health (mobility, self-care, usual activities, pain/discomfort, anxiety/depression). In the original version it is divided into 3 levels of severity. In this study, we used 5 levels of severity, as suggested by Kind and Macran17. Patients were asked to describe their health state as of today, and the recommended Danish scoring algorithm was applied to create a health utility score between 0 (death) and 1 (perfect health)15,18. A minimally important difference (MID) in EQ-5D score of 0.05 has been reported for patients with stable RA in a Canadian study19.
A random sample of 16,136 individuals from the general population was pooled from 3 Danish health surveys from year 2000 and applied as the EQ-5D population norm20.
Definitions of disease activity and clinical remission
We applied the following 2 definitions of disease activity and clinical remission:
-
DAS28 calculated according to the following algorithm: DAS28 based on s-CRP = 0.56 * √ (TJC28) + 0.28 * √ (SJC28) + 0.36 * ln (s-CRP + 1) + 0.014 * patient’s global RA VAS score + 0.9621. Patients were categorized into 4 categories: DAS28 remission (< 2.6), low DAS28 (2.6–3.19), moderate DAS28 (3.2–5.1), and high DAS28 (> 5.1).
-
CDAI score = SJC28 + TJC28 + patient’s global VAS (cm, 1 decimal) + physician’s global VAS (cm, 1 decimal). Patients were categorized into 4 categories: CDAI remission (≤ 2.8), low CDAI (2.9–9.9), moderate CDAI (10.0–21.9), and high CDAI (≥ 22)22.
We also calculated EQ-5D scores for patients fulfilling 2 other clinical remission criteria as suggested by Sokka, et at4.
-
Clinical remission 28; 3 of 3 of the following criteria met: no swollen joints on 28-joint count, no tender joints on 28-joint count, and normal s-CRP.
-
MD remission: no disease activity according to the rheumatologist (physician’s global VAS score ≤ 0.3 cm).
Missing data
Missing items in the EQ-5D were replaced by the median value of the item in question, when a minimum of 4 of the 5 questions had been answered, otherwise the observation was excluded.
Missing values in the disease-related variables were replaced by predicted values based on regression models with sex, age, disease duration, and s-CRP as explanatory variables.
Missing observations analyses comprised demographic, disease, and treatment-related comparisons between patients included in the analyses and those excluded due to incomplete EQ-5D data.
Statistical analyses
Statistical analyses were performed with Stata version 9.0 (Stata Corp., College Station, TX, USA), and a p value of ≤ 0.01 was chosen as the level of statistical significance.
EQ-5D scores for RA patients stratified by sex and divided into 3 age groups were presented according to the DAS28 and CDAI disease activity categories. EQ-5D score differences (ΔEQ-5D) between patients and the age and sex-matched general population were calculated by subtracting the patient scores from the norm scores for each patient. Possible confounders were taken into account by estimating 4 multiple linear regression models with ΔEQ-5D for men and women as outcome variables and disease activity according to DAS28 and CDAI as explanatory variables, adjusting for factors related to sociodemography (age, marital status, education), lifestyle (BMI, smoking, exercise habits), RA (disease duration, IgM-RF, HAQ, joint erosions, joint surgery, extraarticular features), treatment (methotrexate, BARD, and glucocorticoids), and comorbidity. Collinearity was assessed in a Spearmans rank correlation matrix prior to estimating the models. Age, disease duration, and joint surgery were included regardless of the level of association with other variables because of an a priori hypothesis of an independent effect on HRQOL. Joint erosions and HAQ were excluded from the models based on correlations above 0.30 (0.30–0.52) with disease duration, joint surgery, DAS28, and CDAI and thus at risk of causing collinearity. Except from a correlation coefficient of 0.43 between disease duration and joint surgery, no other coefficients exceeded 0.30.
According to Danish law, no ethical approval was needed for this study. The Danbio registry is approved by the National Board of Health and the Danish Data Protection Agency.
RESULTS
Patients
A total of 3704 patients were recruited, and 85% (3156) completed the questionnaires. Patient characteristics for the 3156 respondents are shown in Table 1. Thirty-seven percent of the patients were in DAS28 remission, while 22% were in CDAI remission. Twenty-five percent and 33% of the patients were in clinical remission 28 and MD remission, respectively (data not shown). There was a tendency that patients in CDAI remission had less severe disease, as illustrated by lower HAQ scores and smaller proportions of radiographic erosions and IgM-RF-positive patients. Across the remaining DAS28 and CDAI disease activity categories, largely comparable baseline patient characteristics were observed.
Patient characteristics for all respondents and stratified according to disease activity using the DAS28 and CDAI criteria (n = 3156). Values are median (interquartile range) unless otherwise stated.
EQ-5D
We excluded 244 observations from further analyses due to missing EQ-5D items, yielding 2912 complete observations. The excluded patients were 9 years older and used more glucocorticoid medication (28% vs 20%, respectively) compared to those included in the analyses, but did not differ in other patient characteristics (data not shown).
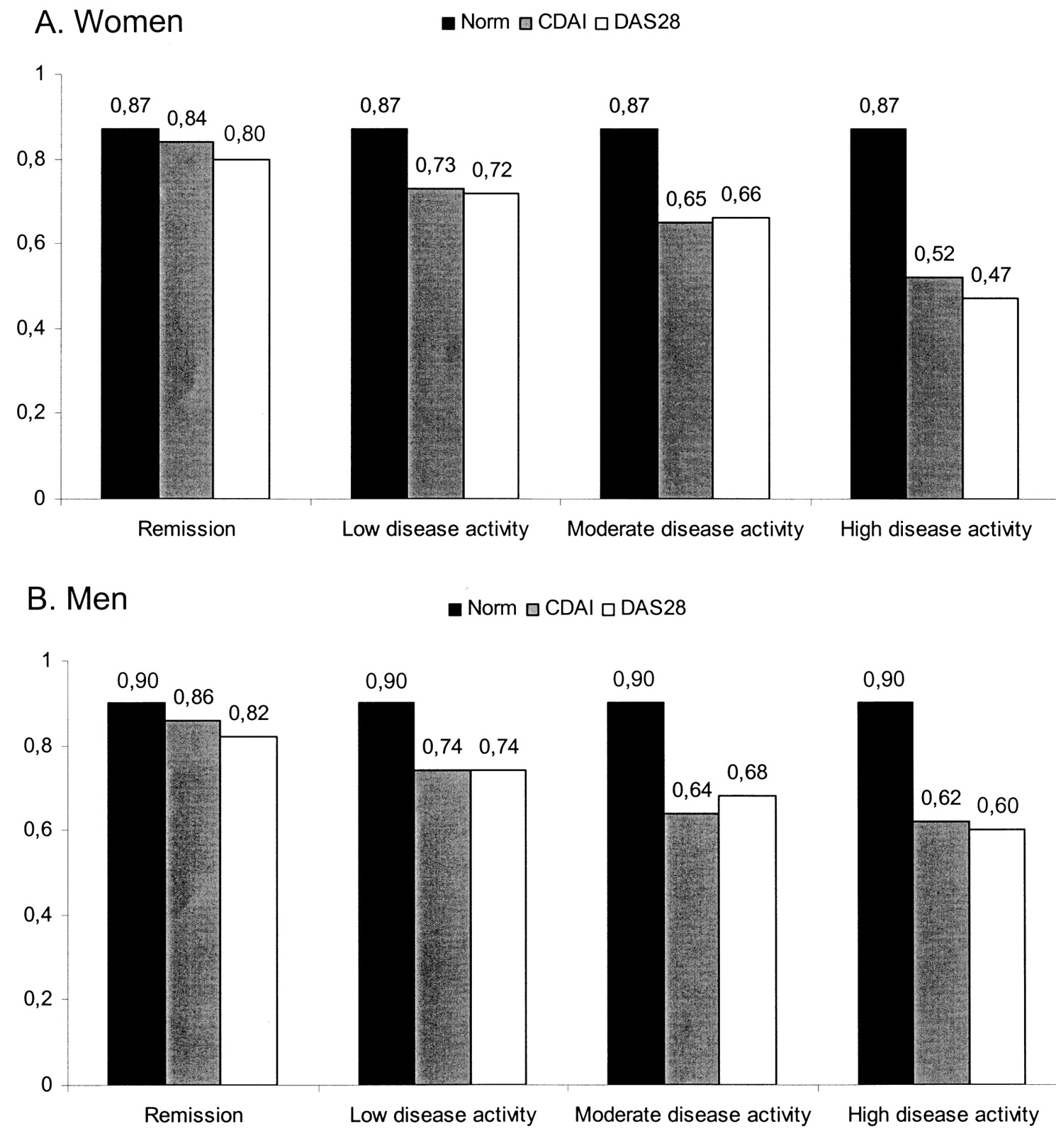
Figure 1 suggests an almost linear association between EQ-5D and disease activity. Patients with high disease activity scored consistently worse than patients with less disease activity, regardless of the definition used. Patients in CDAI remission scored better than patients in DAS28 remission.

Sex-stratified EQ-5D scores (A: women; B: men) for the general population and patients with RA grouped according to disease activity using the DAS28 and CDAI criteria.
The EQ-5D scores deteriorated with increasing age in patients and the general population, and women scored overall worse than men (Table 2A, 2B). There was a tendency that older patients in CDAI remission scored equally well or better than the general population, while the younger patients, across all levels of disease activity including remission, scored worse. The mean (standard deviation) EQ-5D scores for patients in clinical remission 28 were women 0.79 (0.15) and men 0.82 (0.13), and for those in MD remission, women 0.79 (0.15) and men 0.80 (0.15).
EQ-5D scores for the female general population (n = 8543) and RA patients (n = 2183) stratified according to age and disease activity using the DAS28 and CDAI criteria. Data are mean (standard deviation).
EQ-5D scores for the male general population (n = 7593) and RA patients (n = 729) stratified according to disease activity using the DAS28 and CDAI criteria. Data are mean (standard deviation).
The EQ-5D score differences (ΔEQ-5D) between the general population and RA patients (norm-patients) according to DAS28 and CDAI disease activity categories are given in Table 3. Patients with RA had overall worse scores than the general population. The score differences were smaller for patients in CDAI remission than for patients in DAS28 remission, and for women the difference between patients and the general population was statistically insignificant.
EQ-5D score differences (∆EQ-5D) between the general population and RA patients [(norm)–(patients)] (n = 2912). Values are mean (standard deviation). EQ-5D norm values used in the calculation of the ∆EQ-5D may differ from the norm values observed in Table 2A and 2B because of the different age distribution in the norm and patient sample. This may lead to slightly different ΔEQ-5D values than could be expected from Table 2A and 2B.
Regression analyses
The EQ-5D score differences (ΔEQ-5D) between the general population and RA patients (norm-patients) according to DAS28 and CDAI disease activity categories after adjustment for age, marital status, education level, body mass index, exercise, smoking status, disease duration, extraarticular features, joint surgery, IgM-RF, comorbidities, and treatment with methotrexate, biological antirheumatic drugs and glucocorticoid are given in Table 4. The adjusted ΔEQ-5D values were generally lower (0 to 0.04) than the unadjusted values in Table 3, but the pattern across disease activity levels was similar.
Regression model estimates illustrating the association of disease activity with EQ-5D score differences (∆EQ-5D) between the general population and patients with RA (n = 2912). Estimates were adjusted for age, marital status, education level, body mass index, exercise, smoking status, disease duration, extraarticular features, joint surgery, IgM-rheumatoid factor status, comorbidities, and treatment with methotrexate, biological antirheumatic drugs and glucocorticoid.
DISCUSSION
Our aim was to compare one aspect of HRQOL, namely the EQ-5D, of patients with RA to that of the general population, and to determine the association between disease activity and HRQOL, focusing on the comparison of different definitions of clinical remission. For the first time age- and sex-specific data on EQ-5D in patients with RA stratified by disease activity were presented and compared with a large population sample. Our findings confirmed that the HRQOL in patients with RA overall was reduced in comparison with the general population. Moreover, we discovered a strong association between disease activity and HRQOL, and most interestingly that the HRQOL of patients in CDAI remission approached that of the general population.
Strengths of the study include the large sample size of RA patients, and the age and sex-matched comparisons of EQ-5D scores from the general population. Further, the patients were recruited from clinics in different geographic areas (urban and rural) and environments (university vs general hospitals) with a highly satisfactory response rate of 85%. We believe that the patient sample is representative of a typical, unselected RA outpatient population, which increases the weight of our findings. The normative EQ-5D data add to the strength of the study through the large and randomly selected sample, which has ensured a broad and representative standard of reference.
Limitations of the study relate to the fact that the general population data were collected 6–7 years earlier than the patient sample. It is unknown whether the HRQOL of the general population has improved over this period; however, the better scores in the older subgroups of patients than in the general population may indicate this. Another explanation includes adaptation to disease, leading to an adjustment of life expectations over time in patients with a chronic disease. Therefore, the differences in our study between patients and the general population may be underestimated.
Clinical remission has become a realistic goal in RA, and to our knowledge, this is the first study to investigate the association between disease activity and HRQOL focusing on the influence of different remission criteria. In agreement with data from the cross-cultural QUEST study, we found CDAI remission to be a more strict remission criterion than DAS28 remission, as fewer patients fulfilled the former4. The proportion of patients fulfilling the other investigated remission criteria was intermediate to those in DAS28 and CDAI remission, while their EQ-5D scores were lower than the scores of both the DAS28 and CDAI remission groups. Moreover, we found that the EQ-5D scores for patients in CDAI remission approached those of the general population, suggesting near-normal HRQOL in these patients. By contrast, the EQ-5D for patients in DAS28 remission was reduced by 0.05 to 0.06 compared to the general population, which is equal to published MID values19. As noted, however, a possible underestimation of the score differences due to the 6–7 year time lag between the population data and patient data should be kept in mind. Moreover, MID in patients with RA has not been thoroughly investigated for the EQ-5D, and the published value should be considered mainly as a guideline for comparison. Studies comparing different indices for remission have shown that these may be highly correlated23, and yet seem to reflect different levels of disease activity or severity4,24, and our findings are in accord with this. Our results, moreover, raise the question whether patients in DAS28 remission may achieve improved EQ-5D scores from a further reduction in DAS28.
A possible explanation for the difference in EQ-5D when applying the 2 different remission criteria may be offered from the composition of the indices: in the CDAI, all included items are given equal weight. In contrast, the DAS28 components are weighted differently, so the patient’s global VAS score is given less weight than the physician-determined and biochemical variables (swollen/tender joint counts and s-CRP). As EQ-5D is self-reported, it thus seems plausible that the CDAI would be more associated with other self-reported measures than the DAS28.
Previous studies have sought to describe the effect of rheumatic diseases, such as RA, osteoarthritis, and fibromyalgia on HRQOL as measured by the Medical Outcomes Study Short Form-36 (SF-36), SF-6D, EQ-5D, 15D, HAQ, and Modified HAQ in comparison with the general population7,12–14. The main results have been that rheumatic diseases are associated with worse HRQOL and that patients with RA are among the most severely affected. However, differences in aim and study design limit the comparability with our findings. Thus, one study included only women13, another used self-reported prevalence of musculoskeletal diseases7, and 2 studies were limited to describing patients with a new hospital referral or patients with early RA12,14. In addition, these studies were small and unable to describe the effect on HRQOL of rheumatic disease in subgroups based on sex, age, and disease activity. A Norwegian study included a sample sufficiently large to evaluate age and sex-specific variations in the effect of RA on HRQOL25. The authors studied 1052 RA patients and 2323 individuals from the general population, and reported decreased utility scores (by SF-6D) for RA patients in comparison with the general population across age groups. Female RA patients scored worse than male patients, and the gender difference was equally apparent in the general population25. Although not directly comparable due to the different measurement instruments used (EQ-5D vs SF-36 and SF-6D), our findings are in accord with those of the Norwegian study.
We found decreased HRQOL as measured by the EQ-5D in patients with RA in comparison with the general population in this large cross-sectional study, and this impairment was strongly related to the disease activity. The EQ-5D of patients in CDAI remission approached that of the general population, while this was not to the same extent the case for patients in DAS28 remission. Our results document that the selection and fulfilment of strict remission criteria is critical in order to achieve near-normal HRQOL in patients with RA.
Footnotes
- Accepted for publication September 29, 2009.








{kind=link}