

Abstract
Objective. To explore muscle-specific force (force per physiological cross-sectional area, or PCSA) and muscle activation in cachectic patients with rheumatoid arthritis (RA).
Methods. In 14 muscle-wasted patients with RA and age and sex matched healthy controls, vastus lateralis (VL) force and voluntary activation capacity were assessed during maximal isometric contractions with electromyography and superimposed electrical stimulations. VL PCSA was determined from ultrasound measures of fiber fascicle length (Lf), pennation angle, and volume, together with assessments of body composition by dual energy x-ray absorptiometry and objective physical function.
Results. Although patients with RA had reduced physical function, lower muscle mass, and VL volume relative to controls, there were no differences in muscle-specific force and activation. PCSA, force, and pennation angle tended to be lower in RA, with no differences in Lf.
Conclusion. Muscle-specific force and activation are not compromised and thus are unlikely to contribute to reduced function in cachectic patients with RA.
Impaired physical function is characteristic of patients with rheumatoid arthritis (RA) and is strongly correlated with muscle mass, the main predictor of muscle strength1. Muscle wasting, termed rheumatoid cachexia, is more prevalent and severe in patients with RA than in the general population, perhaps because of increased muscle protein catabolism induced by inflammatory cytokines2.
Compared to published research on muscle quantity, little is known about qualitative changes of rheumatoid muscle. Muscle-specific force, a measure of the force produced per cross-sectional area of a muscle, is reduced in sarcopenia of old age and disuse atrophy, due in part to impaired muscle activation capacity and changes in muscle architecture3.
We aimed to determine whether muscle-specific force, voluntary muscle activation capacity, and muscle architecture are compromised in cachectic patients with RA compared to healthy age and sex matched controls.
MATERIALS AND METHODS
Fourteen cachectic patients with RA (disease duration ≥ 3 yrs) were recruited from Gwynedd Hospital Rheumatology clinics. Patients with pain/swelling in the right knee, disease flare, change in medication in the previous 3 months, other catabolic diseases, or joint replacement were excluded. Significant muscle wasting (“cachexia”) was determined following assessment of appendicular lean mass (ALM) by whole-body dual-energy x-ray absorptiometry using the definition by Baumgartner, et al4. Age and sex matched healthy controls were recruited from the local community.
Maximal voluntary isometric knee extension and flexion torques of the right leg (knee joint angle 70°, hip angle 90°, arms crossed) were determined on an isokinetic dynamometer (CSMi Medical Solutions, Stoughton, MA, USA). Vastus lateralis (VL) force was calculated taking into account maximal voluntary torque, patellar tendon moment arm length as detailed by Onambele-Pearson, et al5, and antagonist co-contraction estimated from electromyographic activity6. Superimposed and postcontraction supramaximal percutaneous double twitches from a DSV Digitimer Stimulator (Digitimer Ltd., Welwyn Garden City, UK) were applied over the quadriceps to determine voluntary activation capacity6.
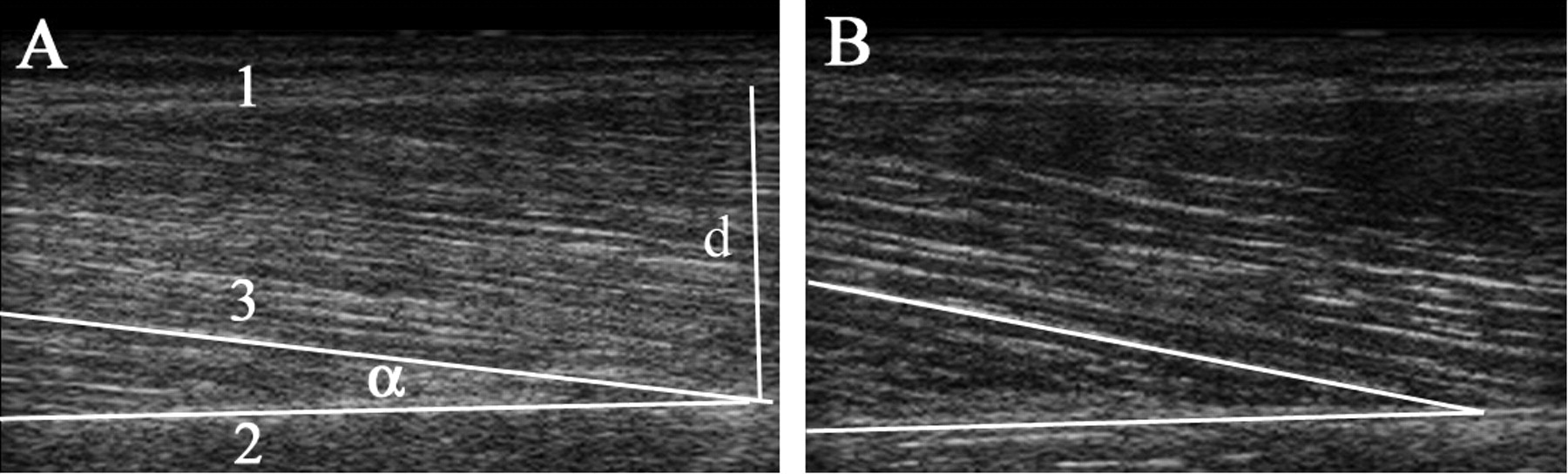
Ultrasonography was used to assess VL volume (VOL; from VL length and VL anatomical cross-sectional area) and muscle architecture, i.e., pennation angle and fiber fascicle length (Lf; Figure 1), which in turn determined physiological cross-sectional area (PCSA = VOL/Lf)6. The primary measure, muscle-specific force, was calculated as VL force/PCSA6.

Sagittal-plane sonographs of the vastus lateralis (VL) muscle of a patient with rheumatoid arthritis (A) and a healthy control (B). Note the greater pennation angle in the muscle of the healthy control. 1: superficial aponeurosis, 2: deep aponeurosis, 3: fiber fascicles; the pennation angle α is the angle of insertion of the fiber fascicle into the deep aponeurosis of the VL. Fiber fascicle length (Lf) was calculated from the pennation angle and the muscle thickness (d) by the equation Lf = d/(sin)(pennation angle).
Further measures were disease activity using the modified RA Disease Activity Index7 and erythrocyte sedimentation rate, objective physical function8,9, the Modified Health Assessment Questionnaire10, and the Medical Outcomes Study Short Form-36. A questionnaire used previously in RA and aging populations11 assessed habitual physical activity and was used to exclude very active participants (> 6 on a scale from 2 to 8).
Depending on normality of the data, the Student’s paired t test or Wilcoxon test was used to detect differences between patient and control groups (p < 0.05).
RESULTS
All patients were taking disease-modifying antirheumatic medication and had low disease activity (Table 1). The groups were well matched for age and habitual physical activity (Table 2). Relative to controls, patients had reduced objective and self-assessed physical function, less ALM and smaller VL volume, and trends toward lower PCSA, lower force, and a smaller pennation angle (Table 2). However, there were no differences in either muscle-specific force or voluntary muscle activation capacity (Table 2).
Clinical characteristics of patients with RA (n = 14: 11 women).
Demographics, body composition, physical function, and muscle-specific force data of sarcopenic patients with RA (n = 14; 11 women) compared to sex matched healthy controls.
DISCUSSION
We observed that muscle-specific force and muscle activation capacity are preserved in patients with RA with significantly impaired physical function and reduced muscle mass.
This finding leads to 2 important conclusions. First, it confirms that muscle loss in RA is a process that differs from that seen in aging and disuse, where muscle-specific force and activation capacity are reduced2. Second, it suggests that the ability of rheumatoid muscle to adapt to physical training is not different from healthy muscle. This emphasizes the potential of high intensity exercise to increase muscle quantity and function in RA, as demonstrated in training studies12–14.
Muscle wasting was a selection criterion in our study. This is a phenomenon seen more frequently in patients with RA2 than in the healthy population, and is thought to reflect systemic effects of inflammatory cytokines on muscle tissue. The relative reduction of muscle mass of 13% was in accord with other studies2.
In determining muscle-specific force, we used definitions of force and size that are standard in muscle physiology research, which take into account architectural features (Lf and pennation angle), influencing the mechanical output of the muscle, and factors affecting force production (co-contraction of antagonist muscles)6. Since the trend toward lower force levels in our patients with RA corresponded with loss of PCSA, the force normalized for PCSA was not compromised. Although the pennation angle tended to be smaller in the patient group, this architectural change was not sufficient to influence the force output.
Similarly, muscle activation capacity was not different between our groups, contrasting with Bearne, et al15, who found 8% lower muscle activation in patients with RA with confirmed involvement of the knee joint compared to healthy controls. However, those results may have been compromised by confounding factors such as fatigue, pain, and joint effusions on muscle force and activation, while we excluded patients with active disease in general and with local knee inflammation. Although our data cannot be extrapolated to patients with persistently active disease, which may affect muscle properties, our stable patients with RA were a relevant population to study, because in rheumatological practice most patients only start exercising once disease control has been achieved with medication.
Limitations of the study
First, the wide age range of the participants and the inclusion of both sexes contributed to the variability of force levels. Second, the work-intensive nature of muscle-specific force assessments necessarily limited the subject numbers.
This is the first study to report on muscle-specific force of the rheumatoid muscle. Further research is required to determine other factors influencing muscle function and the causes of muscle loss.
Even in patients with significant muscle loss, muscle-specific force and the ability to recruit muscle fibers are not compromised. Therefore, these factors are unlikely to contribute to the disability seen in patients with RA.
Acknowledgments
We thank Dr. Jeremy Jones for reviewing the manuscript.
Footnotes
-
This work was supported by a grant from the North West Wales NHS Trust.
- Accepted for publication September 30, 2009.








{kind=link}