

Abstract
Objective. To examine the prevalence of vitamin D insufficiency and the associations of vitamin D concentration with disease status in African Americans with rheumatoid arthritis (RA).
Methods. Study participants (n = 266) were enrolled in the Consortium for the Longitudinal Evaluation of African Americans with Early RA (CLEAR) Registry. The vitamin 25(OH)-D was measured on baseline plasma, and associations of 25(OH)-D with disease status (baseline and at 3 years’ disease duration) were examined using univariate and multivariate regression.
Results. The prevalence of 25(OH)-D insufficiency (≤ 37.5 nmol/l or 15 ng/ml) was 50%, with the highest prevalence in winter. In unadjusted analyses, vitamin D concentrations were inversely associated with baseline pain (p = 0.04), swollen joints (p = 0.04), and Disease Activity Score (DAS28, p = 0.05) but not with measures at 3 years’ disease duration. There were no multivariate associations of 25(OH)-D with any disease measures at baseline or at 3 years, with the exception of a positive borderline association with rheumatoid factor positivity at enrollment (p = 0.05).
Conclusion. Vitamin D insufficiency is common in African Americans with recent-onset RA. Unadjusted associations of circulating vitamin D with baseline pain, swollen joints, and DAS28 were explained by differences in season, age, and gender and were not significant in multivariate analyses. In contrast to reports of Northern Europeans with early inflammatory arthritis, there are not strong associations of 25(OH)-D concentration with symptoms or disease severity in African Americans with RA.
The immunomodulatory effects of vitamin D have been subject to extensive examination, leading to recent speculation that it may play a role in select inflammatory diseases including rheumatoid arthritis (RA). Vitamin D and its analogs have been shown to suppress T cell proliferation and inhibit the expression of proinflammatory cytokines involved in RA pathogenesis including interleukin 2 and interferon-γ1,2. Similarly, vitamin D receptors are constitutively expressed on activated lymphocytes, synoviocytes, macrophages, and chondrocytes in the RA lesion3, while vitamin D metabolites are increased in RA synovial fluid4. In at least 1 epidemiological study, vitamin D intake was inversely associated with the risk of developing new-onset RA5, although conflicting results have been reported6,7. Although investigations of its association with disease activity in RA are limited, preliminary data suggest that levels of circulating vitamin D are inversely associated with disease activity in patients of European ancestry with early inflammatory arthritis8.
Vitamin D insufficiency has consistently been found to be more prevalent in African Americans than in other racial/ethnic populations9–11, possibly related to decreased dietary intake and reduced vitamin D synthesis among individuals with darker skin pigmentation9,12. Data from the Third National Health and Nutrition Examination Survey (NHANES III) demonstrated that, in southern US states, 53%–76% of non-Hispanic blacks compared with only 8%–33% of non-Hispanic whites had insufficient levels of 25-hydroxyvitamin D [25(OH)-D]10. Given the higher prevalence of insufficiency in African Americans, in combination with its potential role in both the incidence and severity of RA, we examined vitamin D status and its associations with disease activity and disease severity in a well characterized group of African Americans with recent-onset RA.
MATERIALS AND METHODS
Study population
The subjects were participants in the Consortium for the Longitudinal Evaluation of African Americans with Early Rheumatoid Arthritis (CLEAR), a multicenter registry of African Americans with RA13. Subjects were enrolled from 4 academic medical centers in the southeastern United States (University of Alabama at Birmingham, Emory University, the Medical University of South Carolina, and the University of North Carolina). There were 266 study subjects with available baseline data (including banked plasma samples) and 191 subjects with data from both baseline and 36 months’ disease duration (time elapsed since symptom onset). Based on the study design, the elapsed time from enrollment to the 36-month visit varied from a minimum of 1 year to a maximum of 3 years. The study was approved by the Institutional Review Board at each participating center. All study subjects provided informed written consent, met the American College of Rheumatology RA classification criteria14, had < 2 years of disease duration from time of first symptom onset, and were of self-reported African American race/ethnicity.
Vitamin D status
The vitamin 25(OH)-D was measured using baseline plasma samples and a commercial radioimmunoassay (Immunodiagnostic Systems Limited, Boldon, UK). The intraassay coefficient of variation was 7.7%. Additional assessments of 25(OH)-D during followup were not available. To facilitate comparisons with other African American populations without RA11, vitamin D insufficiency was defined as a 25(OH)-D concentration ≤ 37.5 nmol/l (15 ng/ml), a threshold used in investigations of older Caucasian populations15–18. The vitamin 25(OH)-D was studied rather than the more active form [1,25-dihydroxyvitamin D (1,25[OH]2D)], because reported associations with disease activity have been shown to be stronger for 25(OH)-D8. Vitamin 25(OH)-D acts as a substrate for 1,25(OH)2D, levels of which are also dependent on calcium and phosphorus status in addition to parathyroid hormone concentrations, measures not available for the participants in our study.
Measures of RA disease activity and severity
In addition to 25(OH)-D levels, baseline evaluations included tender and swollen joint counts (0–28), high sensitivity C-reactive protein (hsCRP, mg/l), rheumatoid factor (RF-IgM) positivity, anticyclic citrullinated peptide (anti-CCP) antibody positivity, the Health Assessment Questionnaire Disability Index (HAQ, range 0–3)19, pain (0–10), subcutaneous nodules (present vs absent), prior use of glucocorticoids, self-reported comorbidity (including a history of liver disease, renal disease, or inflammatory bowel disease), and use of disease-modifying antirheumatic drugs (DMARD) at enrollment. DMARD included methotrexate, anakinra, azathioprine, etanercept, gold salts (oral or intramuscular), leflunomide, hydroxychloroquine, sulfasalazine, and infliximab. There were no patients taking cyclosporine, cyclophosphamide, or adalimumab (the latter was not available at the time of study enrollment for many patients). We also examined associations of vitamin D concentration with a 3-variable Disease Activity Score (DAS28) at enrollment calculated using the Nijmegen formula, substituting an hsCRP for a standard CRP and accounting for the difference in units of measurement:
(DAS28 = [0.56 * sqrt (tender joint count) + 0.28 * sqrt (swollen joint count) + 0.36 * ln (hsCRP = 1)] * 1.10 + 1.15)
Information about calculating the score is available from http://www.reuma-nijmegen.nl/www.das-score.nl/index.html (accessed November 11, 2009).
The methods of autoantibody measurements and assessments of corresponding metric/diagnostic properties in this population have been reported20. There were 9 patients with missing values for both anti-CCP antibody and RF-IgM. In addition, baseline radiographs of the hands and wrists (available for 184 patients at enrollment) were scored using van der Heijde modified Sharp score21 and subjects were categorized by the presence or absence of radiographic erosions (erosion score ≥ 1 vs erosion score = 0). This threshold was used rather than an erosion score of ≥ 2 to 3 based on the low proportion of subjects meeting this threshold at baseline (10% and 7%, respectively). At 36 months’ disease duration (n = 191 subjects with baseline and 36-month followup data), tender and swollen joint counts, HAQ, radiographic severity (n = 134), and pain were reassessed on subjects with available followup. DAS28 measures were not examined at 36 months’ of disease duration because hsCRP measures were not available for that time.
Statistical analysis
The prevalence of vitamin D insufficiency [25(OH)-D level ≤ 37.5 nmol/l, equivalent to ≤ 15 ng/ml] was examined in the overall study population in addition to subgroups that included women of reproductive age (18 to 49 years) and excluding those taking vitamin D supplements. Ninety-five percent confidence intervals (95% CI) were generated for all prevalence estimates using the logit Wald interval, which inverts a Wald-type interval for a logit-scaled prevalence22. Similarly, we examined the prevalence of vitamin D deficiency, defined as a 25(OH)-D level ≤ 25 nmol/l (10 ng/ml). Based on reports suggesting optimal 25(OH)-D concentrations are ≥ 80 nmol/l (32 ng/ml) in Caucasians23, we also examined the prevalence of insufficiency using this cutoff. Vitamin 25(OH)-D concentrations below 78 nmol/l (31 ng/ml) have been shown to lead to elevations in circulating intact parathyroid hormone (iPTH) concentrations24. Chi-square tests and Wilcoxon rank-sum tests were used to compare categorical and continuous variables for those with insufficiency versus individuals with 25(OH)-D levels above this threshold. Variables examined in association with vitamin D status included age, gender, ever smoking, prior or current use of glucocorticoids, DMARD use, vitamin D supplement use at enrollment, education level (high school education vs other), current alcohol use, body mass index (BMI; kg/m2), disease duration, season of study enrollment (summer: June 21–September 20; fall: September 21–December 20; winter: December 21–March 20; or spring: March 21–June 20) in addition to the measures of RA disease activity and severity.
The associations of continuous 25(OH)-D concentrations (per 10 nmol/l increments) with measures of disease activity and severity (at baseline and 3 years’ disease duration) were first examined using univariate regression analyses (logistic regression for dichotomous outcomes and linear regression for continuous outcomes). All outcome variables were modeled separately and, given possible colinearity, were not included as covariates in models of other outcomes. Multivariate regression analyses were then performed, adjusting for age, gender, and season of enrollment8. All analyses involving 36-month disease duration outcomes were adjusted for the corresponding baseline measure. Using additional models, we also examined the influence of including glucocorticoid and DMARD use in addition to BMI as covariates, particularly since a higher BMI has been associated with lower circulating concentrations of vitamin D (a fat-soluble vitamin)11. All analyses were performed using SAS version 9.1 (SAS Inc., Cary, NC, USA).
RESULTS
Patient characteristics
Baseline sociodemographic, health, and disease-specific characteristics of study participants are shown in Table 1 (n = 266). Women made up 81% of the study participants; patients with RA had a mean age of 51 years and disease duration just over 1 year. Over half the participants had a history of smoking, while the mean BMI was more than 30. There were 40 patients using vitamin D supplements, including 15 women of reproductive age. The most common season of study enrollment was winter (29%), followed by spring (27%), summer (26%), and fall (18%). Overall, the mean (± SD) concentration of 25(OH)-D was 40.5 (± 15.6) nmol/l. The frequency of self-reported health conditions that might affect 25(OH)-D concentrations was low; they included liver disease (2.9%), kidney disease (6.1%), and inflammatory bowel disease (2.5%).
Sociodemographics, health behaviors, and disease characteristics in African Americans with recent-onset rheumatoid arthritis (RA); values shown as mean (SD) or number (%) for total group and based on vitamin D status.
Measures of RA disease activity and severity
Study participants had disease-related measures at enrollment suggestive of moderate to severe disease, with a mean HAQ score of 1.6 and mean swollen and tender joint counts of 5 and 8, respectively (Table 1). A majority of patients had received prior glucocorticoid therapy (80%) and most (84%) were taking DMARD at enrollment. The mean plasma hsCRP was elevated (15.7 mg/l, normal ≤ 3 mg/l), while 14% had rheumatoid nodules, 60% were anti-CCP antibody-positive, and 69% were RF-positive. Twenty-seven percent of participants’ baseline radiographs demonstrated erosions. Clinical measures available at 36 months’ disease duration (n = 191) included HAQ score (mean 1.46, SD 1.00), swollen joint count (mean 3.8, SD 5.6), tender joint count (mean 6.4, SD 8.2), and pain (mean 6.1, SD 5.4), and the presence of radiographic erosions (41%; data not shown).
Prevalence of vitamin D insufficiency and deficiency
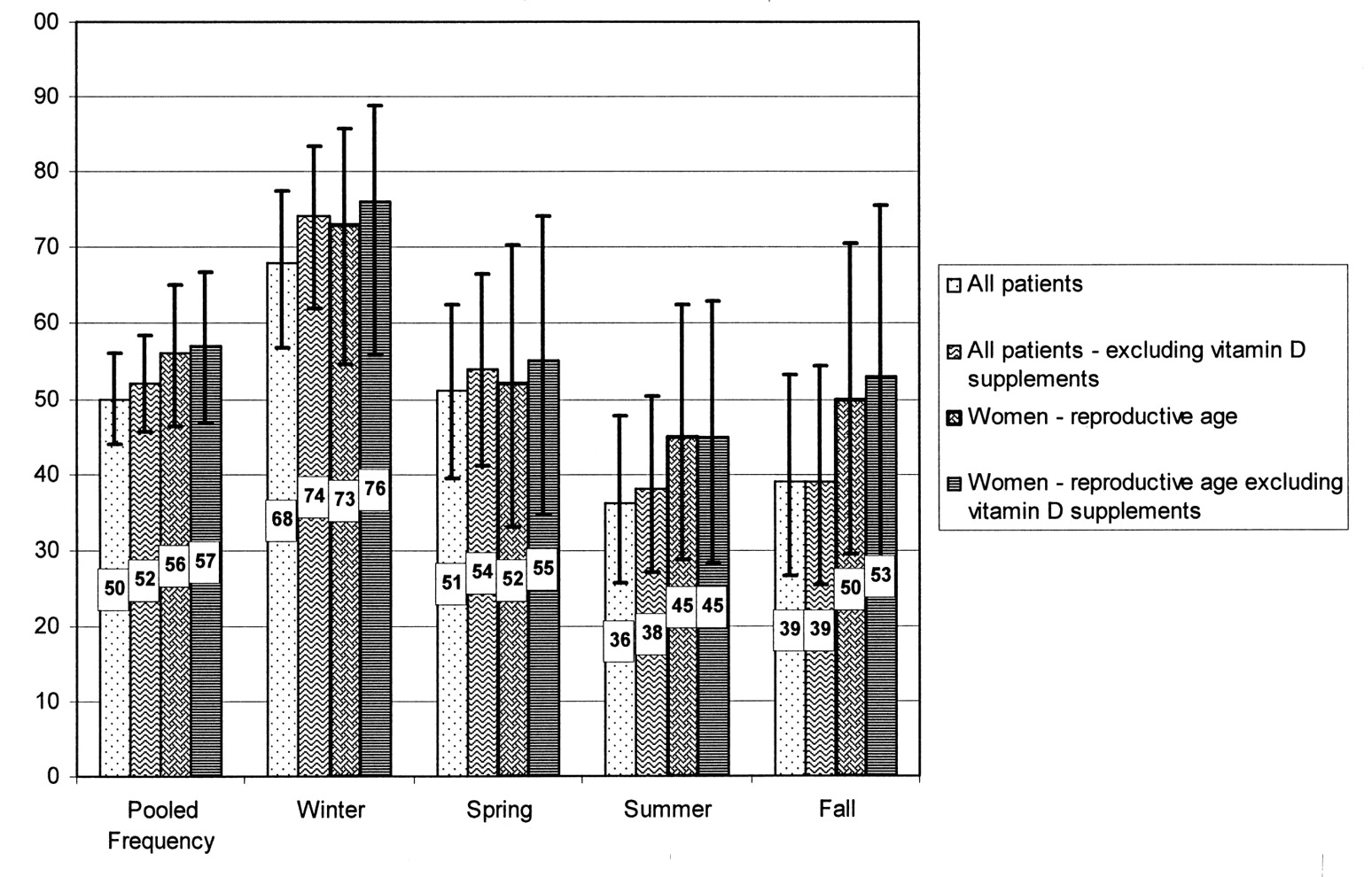
The overall prevalence of vitamin D insufficiency (≤ 37.5 nmol/l) was 49.6% (95% CI 43.6%–55.6%; Figure 1), a frequency that increased to 52.2% (95% CI 45.7%–58.7%) when subjects taking vitamin D supplements were excluded (n = 40). Vitamin D insufficiency was more common in women of reproductive age (18–49 years), with a prevalence of 55.7% (95% CI 46.1%–64.8%), a frequency that increased only slightly after the exclusion of women taking vitamin D supplements (57.1%; 95% CI 46.8%–66.9%). Factors associated with vitamin D insufficiency included younger age, the absence of vitamin D supplementation (11% with vitamin D insufficiency reported supplement use vs 20% among those with sufficient levels; p = 0.04), current alcohol use (22% of patients with insufficiency vs 11% of others; p = 0.01), and season of enrollment (p = 0.0003).
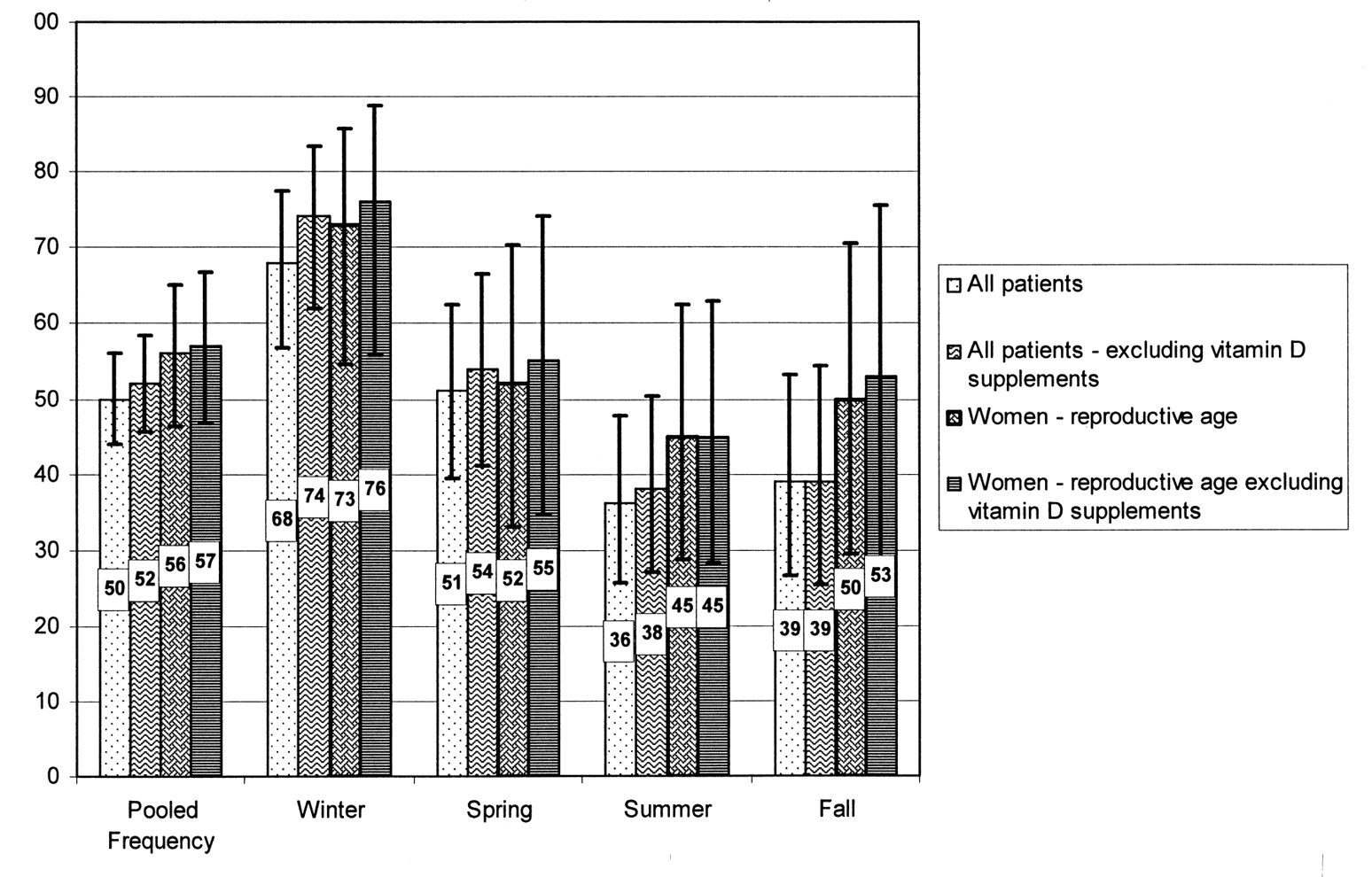
Overall and seasonal prevalence (%) of vitamin D insufficiency in African Americans with recent-onset rheumatoid arthritis (n = 266). Frequency is shown for (1) all patients, (2) all patients after excluding individuals using vitamin D supplements, (3) women of reproductive age (18 to 49 yrs), and (4) women of reproductive age after excluding those taking vitamin D supplements (pooled frequency and frequency for each season of enrollment). Black bars show 95% confidence intervals.
Vitamin D deficiency (≤ 25 nmol/l) was observed in 14.7% of patients (95% CI 10.9%–19.4%). Using the suggested threshold of 80 nmol/l23, vitamin D insufficiency was nearly universal (98.5%; 95% CI 96.1%–99.4%). Using this threshold, there was a single woman of reproductive age with adequate concentrations of circulating 25(OH)-D.
Rates of vitamin D insufficiency (≤ 37.5 nmol/l) based on season of enrollment are shown in Figure 1. The highest prevalence was observed for those enrolled during winter (68.4%; 95% CI 57.2%–77.8%), with the lowest prevalence during summer (35.7%; 95% CI 25.4%–47.5%). Similar seasonal variation was observed with vitamin D deficiency (≤ 25 nmol/l), with the highest prevalence in winter (21.0%; 95% CI 13.3%–31.6%), although the lowest prevalence was observed in the fall (4.1%; 95% CI 1.0%–14.9%).
Associations of vitamin D with measures of RA disease activity and severity
In unadjusted analyses, baseline 25(OH)-D levels were inversely associated with baseline pain scores (ß-coefficient –0.24, p = 0.04, per 10 nmol/l), swollen joint counts (ß-coefficient –0.49, p = 0.04), and DAS28 (ß-coefficient –0.11, p = 0.05; Table 2). There were no associations with other measures of disease activity or severity at baseline or any of the outcomes assessed at 36 months of disease duration (Table 2). The associations of vitamin D concentration with baseline pain, swollen joint counts, and DAS28 scores were attenuated and not statistically significant after multivariate adjustments for age, gender, and season of enrollment. Of the covariates modeled, age had the strongest confounding effects on baseline pain (ß = –0.041, p = 0.003) and DAS28 (ß = –0.014, p = 0.04), while season of enrollment (ß = –0.14 to –1.30, p > 0.1) had the strongest association with swollen joint counts (data not shown). Although not significant in univariate analysis, higher concentrations of 25(OH)-D were positively associated with seropositivity for RF-IgM (OR 1.22, 95% CI 1.00–1.49, p = 0.05, per 10 nmol/l increase) after adjusting for age, gender, and season. This association was attenuated and not statistically significant after additional adjustment for BMI (p = 0.08; data not shown). None of the multivariate results was significantly changed after additional adjustment for glucocorticoid or DMARD use (data not shown).
Univariate and multivariate associations of plasma vitamin D [25(OH)-D] concentrations with rheumatoid arthritis (RA) baseline and 36-month measures of disease activity and severity in African Americans with recent-onset disease (n = 266).
DISCUSSION
Our patient population demonstrated high rates of vitamin D insufficiency (50%) that were in accord with data from national population-based studies, underscoring the relatively high prevalence of vitamin D insufficiency in African Americans10,11. Recognizing the limitations of making comparisons across studies, the frequency of vitamin D insufficiency in reproductive-age African American women with RA (56%) appears to be higher than that reported in NHANES III of a similar population without RA (42%)11. In contrast to our a priori hypothesis, we observed no conclusive associations of vitamin D concentrations with disease activity or severity. Although baseline pain, swollen joints, and DAS28 scores were inversely associated with vitamin D concentration in univariate analyses, these associations failed to meet statistical significance following multivariate adjustments, suggesting that this association is explained primarily by differences in age and season of assessment. Although of borderline significance and potentially representing a spurious finding, the association of 25(OH)-D concentration with RF seropositivity was not anticipated.
The results regarding the association of vitamin D status and self-reported pain may not be surprising given conflicting literature regarding hypovitaminosis D and musculoskeletal pain. Previous studies have suggested a link between low vitamin D and musculoskeletal pain25,26, and some have even suggested that patients with chronic pain should be routinely screened for hypovitaminosis D27. More recently, the notion of an association between pain and vitamin D status has been refuted28,29. Further, treatment of hypovitaminosis D does not appear to be effective in management of patients with chronic pain29.
Our results conflict with those of Patel and colleagues8, who observed evidence of an inverse relationship between vitamin D concentrations and measures of disease activity in early inflammatory arthritis both at baseline and after 1 year of followup. Specifically, these investigators observed inverse associations between 25(OH)-D and baseline tender joint counts, DAS28 score, and HAQ score, with only the associations with HAQ score remaining significant after 1 year of followup. Interestingly, associations of vitamin D status with pain scores were not examined in this population8. There are several factors that may account for the differences observed between the present study and previous findings, mainly regarding differences in the study populations (i.e., RA in the present study vs inflammatory arthritis, African Americans vs Northern Europeans, and differences in exposure to therapies including glucocorticoids and DMARD). Patients in the Patel, et al study were treatment-naive at baseline, enrolled within 6 months of disease onset, and with a cumulative DMARD use of less than 6 weeks. In contrast, patients in our study had disease durations of up to 2 years at enrollment and most patients had received therapy for their RA for at least a limited time, reflected in the high rate of DMARD and current or past glucocorticoid use. Recognizing these potentially important study differences, our results call into question the role of vitamin D status as an important disease modifier, at least in this population.
The results of this investigation are specific to African Americans with recent-onset RA, which limits the possibility of generalizing these findings. Despite its high prevalence, the precise impact of hypovitaminosis D in African Americans has not been well established, and preliminary data suggest that the physiological effects of vitamin D concentration may differ by race or ethnicity. Compared to Caucasians, African Americans appear to be less sensitive to changes in circulating 25(OH)-D with respect to bone mineral density30. It is conceivable that African Americans may also be less sensitive than Caucasians to the effects of vitamin D status in relation to its effects on other disease pathways, including systemic inflammation in RA. Further studies aimed at improving our understanding of racial or ethnic differences in the antiinflammatory effects of vitamin D could provide insight into RA pathogenesis, with potential application to other diseases in which hypovitaminosis D has been implicated.
It is worth noting that the threshold used to define vitamin D insufficiency (≤ 37.5 nmol/l) in our study might be considered conservative. This threshold was used primarily to facilitate historical comparisons with reports from other African American populations11. Different authors have argued in support of optimal 25(OH)-D levels as high as 75 to 80 nmol/l, levels based primarily on fracture prevention data also derived from older Caucasian populations23,31. As our data illustrate, using higher thresholds renders hypovitaminosis D nearly universal among African Americans with recent-onset RA. Indeed, an optimal threshold and the potential benefit of increased vitamin D intake in African Americans remain to be defined32. Given the potential consequences of vitamin D deficiency with the risk of other chronic diseases including diabetes, multiple sclerosis, malignancy, and heart disease33,34, its health implications in African Americans (including those with RA) may extend well beyond bone health and musculoskeletal disease.
There are limitations to our study. Study participants were enrolled in the southeastern United States, where sun exposure rates (and resulting vitamin D concentrations) may differ significantly from other populations in other geographic regions. It is possible, for instance, that African Americans with RA from northern latitudes may have a substantially higher prevalence of hypovitaminosis D. Our study also reflects limited followup, as vitamin D status was assessed only at baseline, and disease activity recorded at enrollment and after 3 years of disease duration, with the latter available for a majority of patients. Although participants had a limited disease duration at the time of enrollment, the possibility exists for unmeasured confounding from different RA treatments received, varying amounts of sun exposure, and dietary intake of vitamin D. However, we would anticipate that confounding secondary to the effect of RA on mobility, sun exposure, and nutritional status would have resulted in even stronger associations with measures of disease activity, particularly HAQ scores.
This is the largest study to date examining the role of vitamin D status in African Americans with RA, a vastly understudied population. Although vitamin D concentrations do not appear to play a major role in RA disease activity in this population, the high prevalence of hypovitaminosis D underscores the critical need for additional studies examining the longer-term effects of vitamin D status in African Americans with RA.
Vitamin D insufficiency is common in African Americans with recent-onset RA, affecting approximately half of this population. Associations of lower concentrations of circulating vitamin D with increased pain, higher swollen joint counts, and DAS28 values in this group appear to be primarily related to differences in season, age, and gender and were not significant in multivariate analyses. In contrast to reports of Northern Europeans with early inflammatory arthritis, there are not strong associations of 25(OH)-D concentration with symptoms or disease severity in African Americans with RA.
Acknowledgments
The CLEAR Registry is an NIH-sponsored resource, with clinical data, DNA, and other biological samples available to approved users. Details on obtaining data or biological samples are available at http://www.dom.uab.edu/rheum/CLEAR%20home.htm. We acknowledge these CLEAR Registry staff members and coordinators: Stephanie Ledbetter, Zenoria Causey, Selena Luckett, Laticia Woodruff, Candice Miller, Joyce Carlone, Karla Caylor, Sharon Henderson, Diane Bresch, Trisha Sturgill, and Teresa Arb. We also acknowledge these physicians who enrolled patients into the CLEAR Registry: Jacob Aelion, Charles Bell, Sohrab Fallahi, Richard Jones, Maura Kennedy, Adahli Estrada Massey, John Morgan, Donna Paul, Runas Powers, William Shergy, Cornelius Thomas, and Ben Wang.
Footnotes
- Accepted for publication September 2, 2009.








{kind=link}