

Abstract
Objective. To estimate the incremental costs to public payers for patients with ankylosing spondylitis (AS) of working age compared with reference subjects from the general population.
Methods. We investigated total costs for 3 years (2005–2007) in 116 outpatients under 66 years of age with AS attending rheumatological care in Malmö, Sweden. Mean (SD) age was 46 (11) years and mean (SD) disease duration was 24 (11) years. Two subjects per AS patient matched for age, sex, and residential area were selected from the Population Register to serve as a reference group. We retrieved data concerning sick leave, prescription drugs, and healthcare consumption from Swedish health-cost registers by the unique personal identification numbers.
Results. The mean total cost for the 3-year period 2005–2007 was US $37,095 (SD $30,091) for patients with AS, and $11,071 (SD $22,340) for the reference group. The mean indirect cost was $19,618 and $5905, respectively. Mean cost for healthcare was $8998 for the AS patients and $4187 for the reference subjects, and mean cost for drugs was $8479 and $979, respectively. The patients with AS treated with biological therapy constituted 80% of the total drug cost, but just 40% of the cost for disability pension.
Conclusion. Patients with AS had 3-fold increase in costs compared to reference subjects from the general population, and the drug costs were almost 10 times as high. Production losses (indirect cost) represented more than half of total cost (53%).
Ankylosing spondylitis (AS), affecting approximately 0.2% of the population1, is generally diagnosed in young adults. The disease and its comorbidities lead to impairments, activity limitations, and participation restrictions, e.g., work disability2,3,4, with financial consequences for the individual and society5,6,7,8,9,10,11,12. For decades the only effective treatments for AS have been nonsteroidal antiinflammatory drugs, physiotherapy, and surgery. In the last decade, tumor necrosis factor (TNF) inhibitor therapy was introduced and has shown beneficial effects on consequences of the disease13,14,15,16. Studies on the cost of AS are still rather sparse. In recent studies the total cost varied from US $7720 to $28,769 a year when the societal perspective was used, increasing with worsening disease6,10,11,17,18,19,20,21,22. Indirect costs in these studies ranged from 34% to 73% of the total cost when the human capital method was used for estimation. Studies concerning the cost of AS have mainly reported results based on questionnaires, patient reports, case records, rheumatology registers, patient associations, and estimations10,17,18,19,20,21,22,23.
The objective of our study was to calculate disease-related and all-cause healthcare use and costs for patients with AS attending rheumatological care during the period 2005–2007 compared with reference subjects from the general population, using data from healthcare and administrative data bases in Skåne (South Sweden).
MATERIALS AND METHODS
Study sample
Entry criteria for patients with AS included in this study were as follows: men and women born 1942 or later (age < 66 years in 2007); living in the county of Skåne in southern Sweden on December 31, 2007; diagnosis of AS according to the New York criteria24 verified in case records; and registered for consultation with a doctor in rheumatology specialist care in Malmö between 1993 and 2006. Malmö is a city in Skåne with a population of 230,000 over the age of 15 years. AS patients were identified from outpatient registers of the Rheumatology Department of the University Hospital of Malmö and the 3 rheumatologists practicing privately in the city. Patients were included in the study if they had AS according to ICD-9 (720A) or ICD-10 (M45) or, when no code was available, a written diagnosis of AS, or the synonyms pelvospondylitis or Mb Bechterew was present. In total, 158 patients, 120 men and 38 women, were identified. One of the authors (BS) examined their medical records and found that 36 patients did not fulfil the New York criteria for diagnosis. Two patients had moved out from the region and 4 were no longer alive on December 31, 2007. Thus, in total, 116 patients, 97 men and 19 women, were included. To further validate the sample the prevalence of uveitis and the serology were registered from medical records. The prescription of TNF inhibitors was investigated from the Prescribed Drug Register of the Swedish Board of Health and Welfare. During the 3-year followup period 25 AS patients were treated with TNF inhibitors and cost estimates were made separately for this group.
Using the Swedish Population Register, 2 subjects per AS patient matched for age, sex, and residential area (zip code) were randomly selected in 2006 to serve as a reference group. Three of the reference subjects had died and 2 had moved out of the region before December 31, 2007; thus there was 1:2 matching for all AS patients except 5.
Cost calculation
Costs were determined from the perspective of public payers, based on register information, and estimated for a 3-year period (January 1, 2005, to December 31, 2007). As far as possible we followed the matrix for cost domains suggested by Merkesdal, et al25. Costs are expressed in US dollars using the exchange rate of US $1 = 7.159 Swedish crowns. The matched subjects serve as a reference group for secular trends instead of adjustment to the consumer price index. In an additional sensitivity analysis we calculated the costs when 5% of the persons in each group, with the lowest and highest costs, were excluded.
The Skåne Health Care Register (SHCR)
The Swedish healthcare system is basically funded by the government and the responsibility for providing healthcare is decentralized to county councils and in some cases to municipalities. Both public and private healthcare providers offer care, all with the same tax-based financing system. Residents are entitled to free healthcare and prescription drugs; only a small co-pay is paid by the patient until a deductible of approximately $125 for healthcare and $250 for prescription drugs is reached. After that the co-pay is waived for the remaining period of the 12 months following the date of the first consultation that added up to the deductible. By law (and to be eligible for free healthcare), all residents have to be registered by their 10-digit personal identification number, a unique number automatically assigned to all residents, which also provides information on date of birth and sex. The population in the county of Skåne is nearly 1.2 million, roughly 12% of the Swedish population. The SHCR contains information on healthcare and costs for all outpatient care and hospital care provided to residents in Skåne. This information was used to define cost for healthcare for AS patients and reference subjects. According to the SHCR, 73% of patients with AS in the region were treated in specialist care during the followup period.
The Register of the Swedish Social Insurance Agency
Under Swedish legislation, all residents aged 16–64 years can be granted economic security from the Swedish Social Insurance Agency in the event of work incapacity owing to sickness, disability, or injuries. The system distinguishes 3 types of income-related benefits that apply after the first day of illness: (1) The waiting period or the qualifying day is the first day of illness. No benefit is paid for this day. (2) From the second to the 14th days of illness, the employer has to maintain the salary. Compensation for sick periods 14 days or less is therefore not registered by the Swedish Social Insurance Agency. (3) Sickness benefit is compensation for illness that reduces work capacity for a limited time from day 15 onward and can be set at 25%, 50%, 75%, and 100%.
Sickness compensation (before 2003 referred to as disability pension) is granted to insured individuals with a permanent or longterm full or partial incapacity for work due to illness or other impairment and can also be set between 25% and 100% as above. Reports on age- and sex-adjusted benefits for days with 100% sick leave (days with sickness benefit or days with sickness compensation) were retrieved from the Swedish Social Insurance Agency. The number of days of partial sick leave (25%, 50%, and 75%) was adjusted to days with 100% sick leave and then multiplied by the actual benefit.
The Prescribed Drug Register of the Swedish National Board of Health and Welfare
The Swedish government determines the work policy of the National Board of Health and Welfare, an agency under the Ministry of Health and Social Affairs. Its duties include the Swedish Prescribed Drug Register. Since July 1, 2005, the register includes personal identification numbers, which makes it possible to calculate the use and cost of prescribed drugs in the population. All prescribed drugs are sold by the national corporation of Swedish pharmacies (Apoteksbolaget).
Using the personal identification numbers, data on costs for sickness benefit/sickness compensation, costs for healthcare, and costs for drugs for AS patients and reference subjects retrieved from the registers were summed to get the total cost to public payers. As the Prescribed Drug Register did not include personal identification numbers until July 1, 2005, we had no register data for prescribed drugs for the first 6 months of 2005. Although the costs for each of the 4 half-years 2006–2007 were higher than for the second half-year of 2005 there was no steadily increasing drug cost. For that reason we assumed that the drug cost for the first 6 months in 2005 was the same as for the second half-year and we thus doubled this cost. Costs for the administration of drugs such as infliximab are included in the costs derived from the healthcare register.
Statistical methods
The median of the difference in total cost between AS patients and reference subjects was determined. The 95% CI for the median was evaluated using the bootstrapping method with respect to matching. Analyses were done using Stata software v. 10.0 (Stata, College Station, TX, USA) and R 2.5.1 (http://www.r-project.org).
The regional ethics board of the University of Lund approved the study (No. 514/2007).
RESULTS
The mean age for AS patients and reference subjects was 46 (SD 11) years and mean disease duration (time since debut) for the AS patients was 24 (SD 11) years. Nineteen AS patients (16%) and 37 (16%) reference subjects were women. Sixty-four (55%) AS patients were HLA-B27-positive, 39 (34%) had ever been treated for uveitis, and 25 (22%) had been treated with TNF inhibitors during the followup period. Characteristics for the total cohort and the subgroup are presented in Table 1. Results given below for men and women are combined.
Characteristics of the main group and subgroup of patients with ankylosing spondylitis (AS) in rheumatological care and reference subjects drawn from the general population (matched for age, sex, and residential area).
Cost calculation. Total cost.
The public payers’ total mean cost for patients with AS for the 3-year period 2005–2007 was $37,095 (SD $30,091; median $38,845; range $0–175,378) and $11,071 (SD $22,340; median $1708; range $0–162,189) for the reference subjects (Table 2). The mean total cost per year was $11,092–13,288 for AS patients and $2797–4206 for the reference subjects (Table 3). The median of the difference in total cost between AS patients and reference group for the 3-year period was $25,958 (95% CI $17,789, $33,679). Fifty-five percent of AS patients and 89% of reference subjects had a mean total cost below $34,920 (250,000 Swedish crowns), and 0.8% of the AS patients and 12% of reference subjects had no costs during the followup period.
Cost (US $) and resource consumption for the 3-year period 2005–2007 for patients with AS in rheumatological care and reference subjects drawn from the general population (matched for age, sex, and residential area).
Cost (US $) and resource consumption per year 2005, 2006, and 2007 for patients with AS in rheumatological care and reference subjects drawn from the general population (matched for age, sex, and residential area).
Direct costs for healthcare
The mean total cost for healthcare for the 3-year period 2005–2007 was $8998 (SD $14,274; median $4627; range $0–127,527) for AS patients and $4187 (SD $11,892; median $1143; range $0–134,831) for the reference subjects. Inpatient care amounted to 36% of the healthcare cost for AS patients and 24% for the reference group. Concerning the outpatient costs, physicians (75%), physiotherapists (11%), and nurses (7%) were the main care providers, accounting for 93% of outpatient costs for AS patients. For the reference group, corresponding values were 55%, 7%, 33%, and 95%, respectively. Table 2 presents the costs for the whole 3-year period; the costs per year are given in Table 3.
Costs for prescription drugs
The mean cost for the cases for the 3-year period 2005–2007 was $8479 (SD $15,203; median $1068; range $0–662,866) for the AS patients and $979 (SD $3001; median $0; range $0–30,983) for the reference group (Table 2 and Table 3).
Indirect costs. Cost for sickness benefit and sickness compensation (disability pension)
The mean sickness benefit for the 3 years 2005–2007 was $5982 (SD $14,905; median $0; range $0–73,953) for the AS patients and mean $2131 (SD $8497; median $0; range $0–73,953) for the reference subjects. The corresponding mean amounts for sickness compensation (disability pension) were $13,636 (SD $17,593; median $0; range $0–46,039) for AS patients and $3774 (SD $9789; median $0; range $0–49,965) for the reference group (Table 2 and Table 3).
Subgroup analysis. Cost for patients treated with TNF inhibitors.
The 25 (22%) AS patients ever treated with TNF inhibitors during the 3-year followup period were younger and had shorter disease duration than those not treated with TNF inhibitors (Table 1). Total mean costs for the 25 AS patients treated with TNF inhibitors were $57,632 (SD $23,549; median $55,306; range $18,772–109,535) and the corresponding values for the remaining 91 AS patients were $31,592 (SD $29,348; median $26,921; range $0–175,378). Fifteen patients were treated with infliximab, 4 with etanercept, and 7 with adalimumab during the period. One patient was treated with both etanercept and adalimumab. The drug costs amounted to 57% of the total cost for AS patients treated with TNF inhibitors and 6% of total cost for the remaining 91 AS patients. The mean numbers of days with sickness benefits were 86 days (SD 195; median 0; range 0–791) for the 25 AS patients with anti-TNF treatment and 86 days (SD 220; median 0; range 0–1093) for the remaining 91 AS patients during the followup period. The mean numbers of days with disability pension (sickness compensation) were 162 days (SD 325; median 0; range 0–1095) for the anti-TNF-treated AS patients and 416 days (SD 481; median 0; range 0–1095) for the group not treated with anti-TNF (Table 4). A 30% decrease in costs for sickness benefits for the anti-TNF-treated patients was seen from 2006 to 2007 (Figure 1).
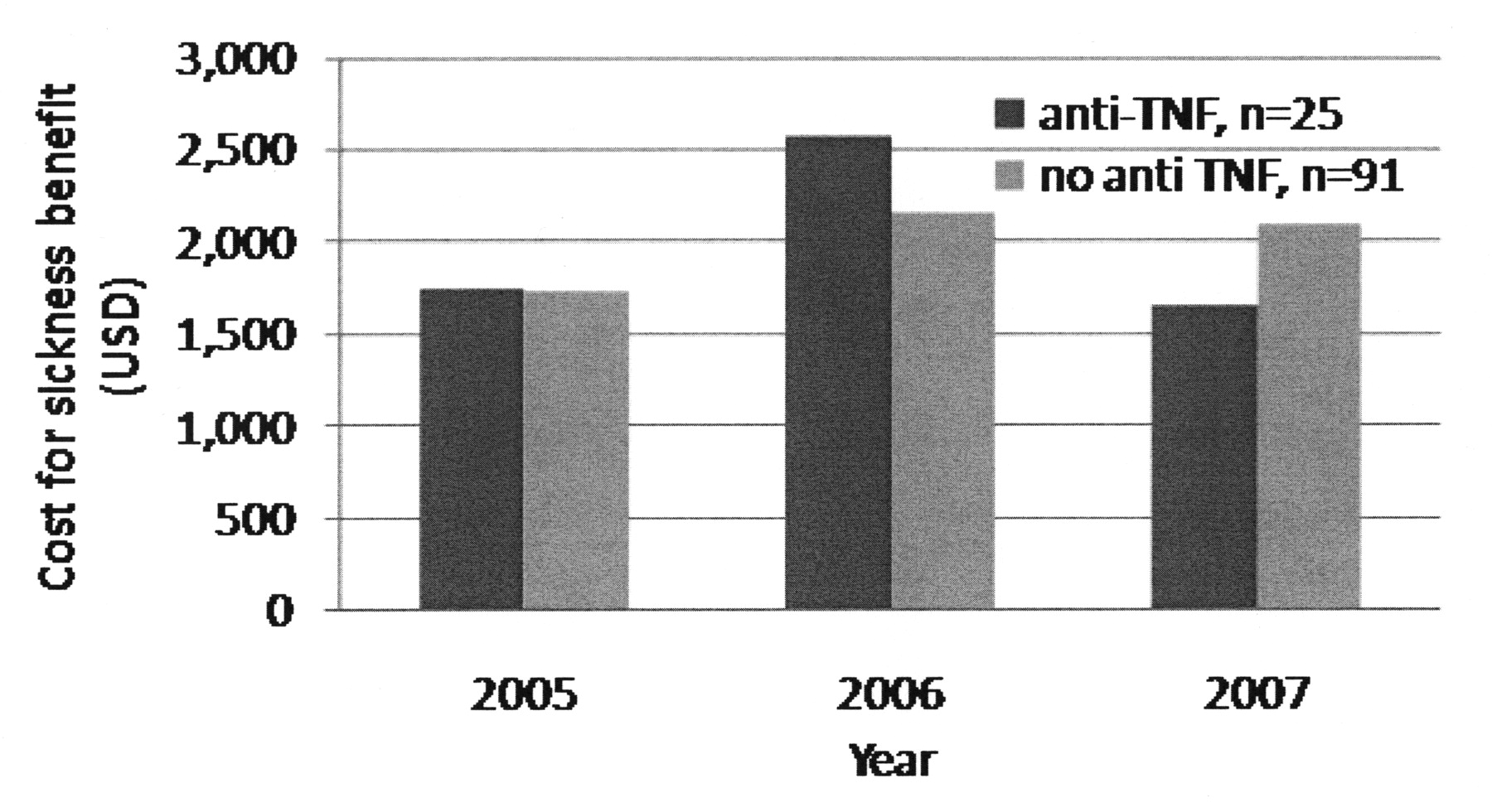
Mean cost per year for sickness benefits (US dollars). Patients with AS were treated/not treated with TNF inhibitors.
Cost (US$) for the 3 year period 2005–2007 for 25 patients with AS in rheumatological care treated with tumor necrosis factor (TNF) inhibitors and 91 patients not treated with TNF inhibitors.
Sensitivity analysis
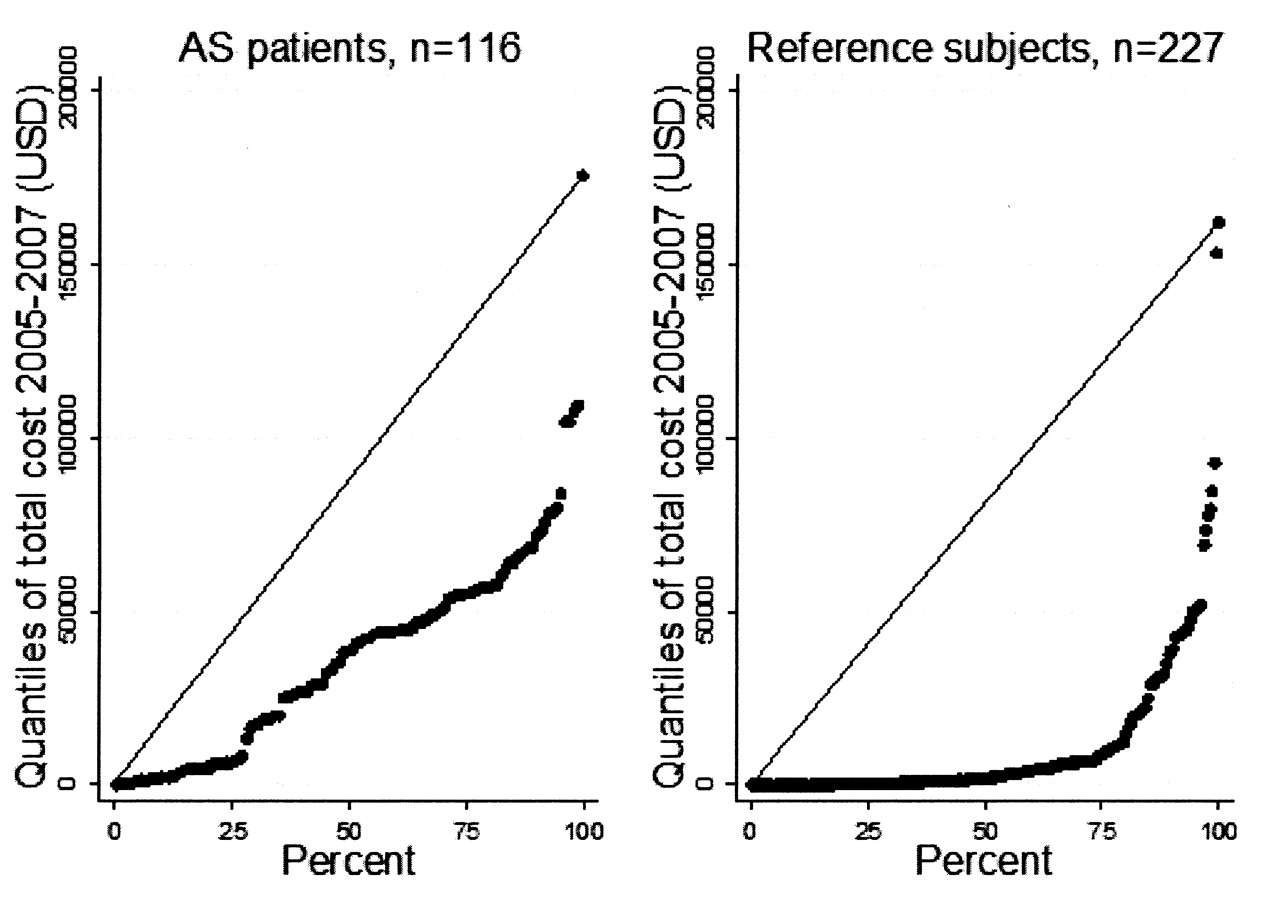
As expected, there was a more uneven distribution of costs in the reference group than among the AS patients (Figure 2). Sensitivity analysis showed that exclusion of 5% of the persons in the groups with the lowest and highest costs influenced the results mainly for the mean total cost for the reference subjects (Table 5).

Quantile plots show the distribution of total costs for AS patients and reference subjects. The x-axis represents fraction of data (percentage) and the y-axis represents all quantiles of total costs for the 3-year period 2005–2007. Diagonals represent theoretical normal distribution.
Total cost of illness (US $) in AS patients and reference subjects before and after the lowest and highest 5% of patients in terms of cost were excluded.
DISCUSSION
Cost of illness studies provide important information on resource utilization and the resulting costs, including identification of cost drivers, costs in different subgroups of patients, and trends over time. Such data are useful to policy-makers setting research and treatment priorities. The studies also provide useful input in economic analyses, such as cost-effectiveness and cost-utility of different treatment strategies. We describe the cost of patients with AS in rheumatological care from the perspective of public payers compared with matched subjects from the general population. To our knowledge this is the first study on the costs of AS compared to a reference group. We found substantially increased costs in patients with AS. The proportion of individuals using healthcare as well as number of units of resource consumed were higher in AS patients than for reference subjects. Indirect costs (for sick leave) were the most important for both AS patients and reference subjects; examining only the direct costs, expenses for drugs represented the highest costs for the AS patients, and expenses for outpatient care the highest costs for the reference subjects.
The strength of our study is that we used prospectively collected data of high quality from registers based on personal identification numbers and collected from independent, reliable, and identical sources for both AS patients regularly attending rheumatological care and reference subjects. This eliminated the need for annualizing or extrapolating data and prevented the interference of errors, e.g., recall bias, that may occur in collecting patient-reported data.
Comparisons between published studies are difficult due to differences in timing, study perspective, sample selection, sources of data, components of costs studied, and cultural and social differences between countries, and thus must be done with caution. Most cost studies in patients with AS use the societal perspective, i.e., all costs are included regardless of who pays6,10,17,18,19,20,21,22,26. Since we used only data from public registers, private healthcare costs are not included, and cost calculations were made from the public payer perspective. Nevertheless, we can conclude that, regardless of the perspective, production losses represent the largest individual cost item in our study as well as in most other studies6,10,17,20,21,22.
The mean annual numbers of inpatient care days in our study were 1.8, 0.9, and 1.3 days/patient, respectively, for the 3 followup years. Three European studies have reported similar values; AS patients in the UK were found to have 1.620 and 1.927 days in hospital/year and the annual number in Spain was 1.7 days18. Boonen, et al reported somewhat higher values for patients in The Netherlands, 2.6 days, and France, 2.7 days, but lower values for patients in Belgium, just 0.3 days per patient/year11. Huscher, et al diverge from other studies by reporting a mean of 20.8 days per year in hospital for patients in Germany21. Apart from that, however, the hospital inpatient care data shown in our findings seem similar to results from other studies. The annual number of physician visits in our study (6–7 visits) lies in the range of European data from other reports11,18,20,22,27. Patients with AS in our sample had fewer physiotherapy visits than reported in other studies11,18,22,27. There also was a trend to fewer physiotherapy visits over the followup period. The reason for this may be that in recent years patients in Sweden were increasingly given individual home exercise programs or recommended to exercise in health and wellness centers. A further reason may be that diagnoses are given earlier, resulting in earlier treatment and thus reduced risk for functional limitations and reduced need for physiotherapy.
Due to drug costs, the 25 patients with AS treated with TNF inhibitors had almost twice the total cost compared to those not treated with biologics. On the other hand the cost for sickness benefits tended to decrease more for the anti-TNF-treated AS patients (Figure 1), and the cost for disability pensions was just 42% of that of the AS patients with no biologic treatment (Table 4). AS patients receiving biologics were younger and had shorter disease duration and it is possible that the biologic treatment will lower their need for future sickness benefits and disability pensions, which may balance the costs in the long term13. It is our intention to continue the cost studies in a larger cohort and with a longer followup period to study the longterm effects of biologic treatment on costs for sick leave and healthcare.
In our study all-cause costs for patients with AS were calculated whether the cost was generated by AS or by other disease not related to AS. The difference, compared with reference subjects, can be considered the total extra cost associated with AS.
The extrapolability of the cost calculations in our study to other countries with other social security and financing systems has limitations. However, we provide a transparency in our presentation of results, detailing each cost and resource consumption to enable such comparisons.
Patient selection in our sample may represent a slight bias, as it was restricted to patients treated by rheumatologists. These patients can be expected to have more active disease, to be more severely affected by the disease, e.g, with more restricted mobility, and thus to receive more intensive treatment than patients treated in primary care. Also, patients with early disease might not have been included, as the New York criteria for diagnosis of AS were fulfilled by all cases in our study. The costs reported may therefore not be representative for the whole spectrum of disease28,29.
We found that the cost to public payers of patients with AS in rheumatological care was more than 3 times higher than the cost of reference subjects from the general population. Indirect costs (for sickness benefits and disability pensions) constituted the major part of total cost. The majority of direct costs were for drugs. The 25 patients treated with anti-TNF therapy had a lower cost for disability pensions (sickness compensation), just 42% of that of the remaining patients. It may thus be that a more active and effective treatment strategy could lower the cost of sick leave and other healthcare in the long term, and this will be a matter for further research.
Acknowledgment
The authors thank Thor Lithman and Dennis Norén for data management.
Footnotes
-
Supported by grants from The Regional Health Service Authorities in Skåne (Region Skåne), The Swedish Social Insurance Agency (Försäkringskassan), and the Swedish Rheumatism Association (Reumatikerförbundet).
- Accepted for publication June 9, 2010.








{kind=link}
{kind=link}