

Abstract
Objective. To measure the prevalence of different types of pulmonary hypertension (PH) and to identify patients with systemic sclerosis (SSc) at highest risk in a multicenter European sample, with a metaanalysis of relevant studies.
Methods. Consecutive patients with SSc recruited at 11 French and Italian centers underwent detailed evaluations, including Doppler echocardiography, chest computed tomography, pulmonary function tests, and right-heart catheterization (RHC), to detect the presence and causes of PH. A metaanalysis was performed, including data from 4 other studies.
Results. Among 206 patients in whom it was suspected, PH was confirmed by RHC in 83 patients (7%). Precapillary PH was found in 64 patients (5%), of whom 42 had pulmonary arterial hypertension (PAH) and 22 had PH secondary to interstitial lung disease (ILD). RHC identified 17 patients (1%) with postcapillary PH secondary to left-heart disease. Patients with DLCO/alveolar volume < 70% were more likely to have precapillary PH (87.5% vs 42%; p < 0.0001). Precapillary and postcapillary PH were associated with advanced age (68 ± 14 vs 59 ± 12 yrs, p < 0.0001, and 74 ± 16 vs 61.5 ± 10 yrs, p < 0.0001, respectively). The metaanalysis of 3818 patients showed a prevalence of precapillary PH of 9% (95% CI 6%–12%) and identified advanced age, longer disease duration, and limited cutaneous disease subset as risk factors for this condition.
Conclusion. The prevalence of precapillary PH in our multicenter study of SSc was 5%, and in the metaanalysis 9%. Our observations support use of RHC to confirm the presence of precapillary PH suspected by noninvasive testing. We also identified patients at high risk who should be carefully monitored.
Pulmonary hypertension (PH) is a fatal disorder characterized by an increase in pulmonary vascular resistance, which leads to right ventricular failure. The Dana Point classification distinguishes pulmonary arterial hypertension (PAH) from PH secondary to other morbid entities1. The interest in PH due to systemic sclerosis (SSc), the connective tissue disease most often associated with PH, has recently increased2. PH, a major cause of death in SSc3, is associated with a worse prognosis and lower therapeutic response rate than idiopathic PAH4,5,6. Obstructive proliferative vasculopathy of the small and medium-size pulmonary arterial circulation and chronic hypoxemia due to advanced lung disease are major causes of precapillary PH in SSc7,8. Pulmonary venoocclusive disease is also a recognized cause of PH, which is thought to be more common in connective tissue diseases9. In addition, left-heart disease and thromboembolic disease may cause, respectively, postcapillary/venous and precapillary PH10,11. Therefore, previous estimates of the prevalence of PH in patients with SSc, ranging widely between 5% and 50%12, were based on (1) various definitions and diagnostic criteria, excluding or including the presence of pulmonary fibrosis, left-heart disease, or both; and (2) various measurement methods, with or without RHC, considered the “gold standard” in the diagnostic confirmation of precapillary PH. Further, the disease characteristics associated with PH remain undefined8,11,13,14.
In view of the latest survival data confirming poor outcomes of SSc-associated PH15, the need to accurately measure its prevalence and identify the subset of patients at highest risk has become pressing. The aims of our study were to measure the prevalence of the different types of PH, using RHC, in 2 large European samples of patients presenting with SSc; and to identify potential associations between presence of PH and patients’ phenotypes in order to identify subsets at risk; and further to perform a metaanalysis of available data to pursue these questions.
MATERIALS AND METHODS
Prevalence of PH in French and Italian samples
Consecutive Caucasian patients with SSc were recruited at 6 French and 5 Italian medical centers. The samples from each country were combined in a single series of patients, allowing the identification of SSc characteristics associated with the presence of PH. Detailed information was collected from all participating patients, including (1) a cutaneous disease subset, defined by LeRoy, et al16, disease duration, from the date of first disease manifestation other than Raynaud’s phenomenon, and history of digital ulceration; and (2) results of biochemical and serological blood tests, including antinuclear/anticentromere antibodies (HEp-2 cell immunofluorescence) and antitopoisomerase-I antibodies (counterimmunoelectrophoresis or immunodiffusion). Presence of pulmonary fibrosis was ascertained in all patients by a high-resolution computed tomography (CT) scan, and by measurements of forced vital capacity (FVC) and carbon monoxide diffusion capacity divided by the alveolar volume (DLCO/AV). The presence of PH was systematically assessed to determine prevalence, using the following screening indices: (1) an estimated echocardiographic systolic pulmonary arterial pressure > 40 mm Hg17 (sPAP; based on transtricuspid gradient, assessed by continuous Doppler flow, adding 10 mm Hg for right atrial pressure); OR (2) DLCO < 50% of predicted in the absence of pulmonary fibrosis; OR (3) unexplained dyspnea. These indications for RHC were used by us and by other investigators in earlier studies of predictors of PH in SSc10,18. Patients identified by this preliminary screening were asked to undergo RHC. [Precapillary PH was defined as a mean resting PAP > 25 mm Hg in the presence of a pulmonary capillary wedge pressure ≤ 15 mm Hg upon RHC10. Postcapillary PH was defined as mean resting pulmonary artery pressure > 25 mm Hg in the presence of pulmonary capillary wedge pressure > 15 mm Hg upon RHC.] Precapillary PH was considered secondary to interstitial lung disease (ILD) when FVC was < 70% of predicted in addition to significant changes on high-resolution CT, as assessed in recent studies19,20. Isolated PAH was defined as precapillary PH in the absence of prominent ILD, as defined by the above criteria. Pulmonary venoocclusive disease was defined as the occurrence of PH associated with radiographic evidence of pulmonary edema and a normal pulmonary artery occlusion pressure21.
Our study complied with the recommendations of the Declaration of Helsinki; all patients provided informed consent to undergo study procedures, which were approved by the ethics committees of all participating centers.
Statistical analysis
Data are presented as means ± standard deviation (SD) for continuous variables, and numbers (percentages) for categorical variables, unless stated otherwise. Differences in frequency were examined using the chi-square test, and normally distributed continuous variables were compared using Student’s t test. We applied the Bonferroni correction for multiple comparisons, dividing 0.05 by the number of disease characteristics tested (10 sets of variables), yielding a corrected probability value of 0.005. A p value ≤ 0.005 was considered statistically significant. A multiple variable stepwise logistic regression analysis was also performed to determine whether PH was associated with the various phenotypes of SSc. We included in our model all variables identified with a corrected p value < 0.1 in the single variable analysis22, and calculated odds ratios (OR) and 95% confidence intervals (CI). In this model, a p value < 0.05 was considered statistically significant.
Metaanalysis of prevalence. Literature research.
Two reviewers (JA and CM) independently searched for articles published between 1966 and June 2009, and expanded on PubMed and Embase, using the terms “systemic sclerosis,” “scleroderma,” or “CREST,” combined with “pulmonary hypertension.” The search was limited to studies in human adults. There was no language restriction. The Medical Subject Heading (MeSH) terms were used for all databases, and a keyword search was substituted when the MeSH search was not available. All MeSH search terms were exploded. In addition, reference lists of the articles found initially were scrutinized to identify other relevant reports.
Inclusion criteria. Study design.
Cross-sectional, prospective or retrospective studies of the prevalence of PH in SSc. Only studies using RHC for diagnosis of PH were included in the metaanalysis.
Study populations
Adults presenting with SSc, who fulfilled the preliminary classification criteria of the American College of Rheumatology23, the LeRoy criteria for early SSc24, or both.
Data extraction
Two reviewers (JA and CM) independently screened retrieved clinical studies for inclusion and extracted data from all included studies using a customized form. If agreement was not achieved at any stage, a third reviewer (YA) adjudicated.
Outcome measure and calculation of pooled prevalence
Prevalence was calculated as the number of cases of PH at a specific time, in a sample of patients with SSc. Precapillary PH was defined as a mean PAP > 25 mm Hg at rest, with pulmonary capillary wedge pressure ≤ 15 mm Hg. Prevalence was calculated as the number of patients with previously or newly diagnosed PH divided by the overall number of patients in the study. Each individual prevalence was first transformed into a quantity via the Freeman-Tukey variance-stabilizing transformation25. A weighted mean of the transformed proportions was calculated, using a DerSimonian-Laird random effects model26,27. The combined prevalence was calculated as the back-transform of this weighted mean. Statistical heterogeneity was determined by Q test (chi-square)28. The effect of publication and selection bias on the summary estimates was tested by Egger bias indicator29.
RESULTS
Study samples
We consecutively included 698 Italian and 467 French patients with SSc. The characteristics of each population and combined samples are provided in Table 1.
Characteristics of the French and Italian samples, separately and combined. Values are means ± SD, or numbers (%) of observations.
Prevalence of PH in both cohorts
RHC was performed in 206 patients who had suspected PH (Table 2). PH in general was found in 83 (7%) patients. The point prevalence of precapillary PH was 5% (64/1165) in the combined populations. Among these 64 patients, 42 had PAH and 22 had PH secondary to ILD. The prevalences of postcapillary PH secondary to left-heart disease and pulmonary venoocclusive disease were 1.5% (17/1165 patients) and 0.2% (2/1165 patients), respectively. Among the 206 patients who underwent RHC, 123 patients had normal hemodynamic measurements (Figure 1).

The distribution of patients with suspected pulmonary hypertension (PH) according to the noninvasive screening process and results of right-heart catheterization (RHC). PAH: pulmonary arterial hypertension; DLCO: carbon monoxide diffusion capacity; ILD: interstitial lung disease.
Numbers (%) of patients with suspected pulmonary hypertension, decreased diffusion capacity, and confirmed pulmonary hypertension at right-heart catheterization in the French and Italian samples, separately and combined.
Relationship between PH and characteristics of SSc
The results of multiple corrected chi-squared analyses are shown in Table 3. By multiple variable logistic regression analysis, DLCO/AV < 70% of predicted (OR 12.9, 95% CI 4.7–33.3, p < 0.0001), FVC < 70% of predicted (OR 4.3, 95% CI 2.2–8.2, p < 0.0001), and age (OR 1.1, 95% CI 1.0–1.2, p = 0.0002) were independent factors associated with precapillary PH.
Disease characteristics of patients with versus those without pulmonary hypertension (PH). Values are mean ± SD, or numbers (%) of observations.
In separate multiple variable regression analyses, the mean disease duration was significantly longer (16 ± 9 vs 12 ± 8 yrs; p = 0.02), and the likelihoods of limited cutaneous subtype (OR 2.3, 95% CI 1.4–4.9, p = 0.008), positive anticentromere antibodies (OR 2.8, 95% CI 1.3–5.7, p = 0.007), and DLCO/AV < 70% of predicted (OR 9.6, 95% CI 3.4–27.4, p < 0.0001) were significantly higher in the 42 patients with PAH than in the 1101 patients without PAH (Table 3). The 22 patients presenting with PH secondary to ILD were significantly more likely to be men (OR 4.7, 95% CI 1.7–12.5, p = 0.003), to have diffuse cutaneous SSc (OR 13.1, 95% CI 2.9–59.1, p = 0.0008), and to have DLCO/AV < 70% of predicted (OR 17.4, 95% CI 2.3–133.5, p = 0.006).
Finally, postcapillary PH secondary to left-heart disease (n = 17) was associated in univariate analysis only with increased age (74 ± 16 vs 61.5 ± 10 yrs; p < 0.0001).
Results of the prevalence metaanalysis
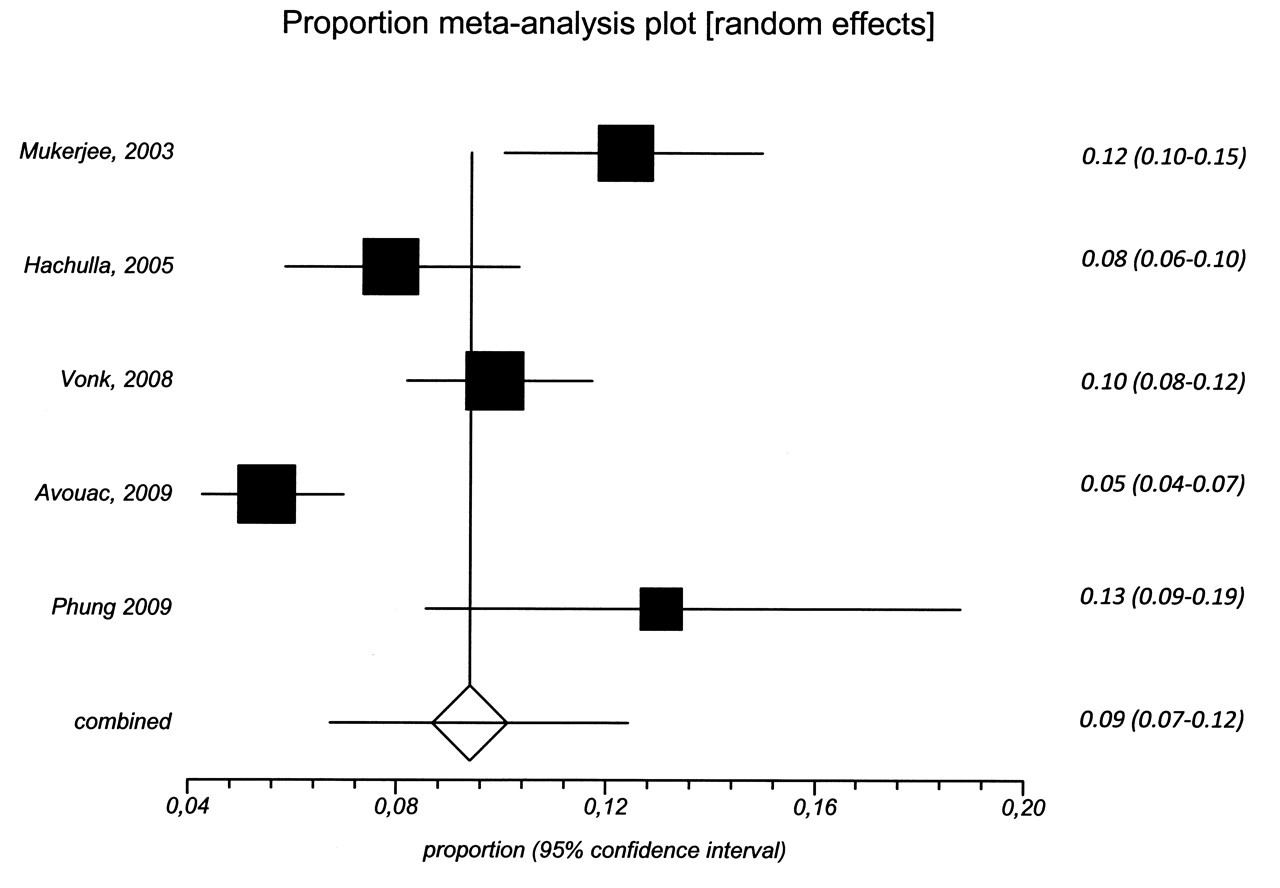
The selection of studies included in the metaanalysis is summarized in Figure 2. Out of 739 articles identified, 4 that reported the prevalence of precapillary PH in SSc, ascertained by RHC, were ultimately retained and added to our combined sample10,11,30,31. It is noteworthy that the criteria for RHC, based on noninvasive screening, differed among these studies (Table 4). The metaanalysis included 3818 patients (age 58 ± 14 yrs, 82% women) with SSc for a mean duration of 9 ± 8 years. The pooled prevalence of precapillary PH was 9% (95% CI 7%–12%; Figure 3, Table 4). This result was based on a random effects model because of significant heterogeneity among studies (Cochran Q = 34.7 for 4 degrees of freedom, p < 0.0001). The Egger bias indicator was not significant (5.2; 95% CI −3.9 to 14.3, p = 0.2). In 4 studies reporting data specifically applicable to patients with precapillary PH, the mean age was 66 ± 12 years, mean disease duration 13 ± 9 years, 72% (95% CI 66%–77%) presented with the limited cutaneous disease subtype, and 32% (95% CI 26%–38%) had pulmonary fibrosis. Separate analyses of patients with PAH compared to those with PH secondary to ILD were missing in 2 studies10,30, and one study excluded patients with PH secondary to ILD11. The metaanalysis of the remaining 2 studies revealed that 63% (95% CI 55%–72%) had PAH and 36% (95% CI 28%–45%) had PH secondary to ILD (Table 4). Among 430 patients who underwent RHC in 4 studies, 44% (95% CI 40%–49%) had normal hemodynamic measurements and 9% (95% CI 7%–12%) had postcapillary PH secondary to left-heart disease (Table 4).
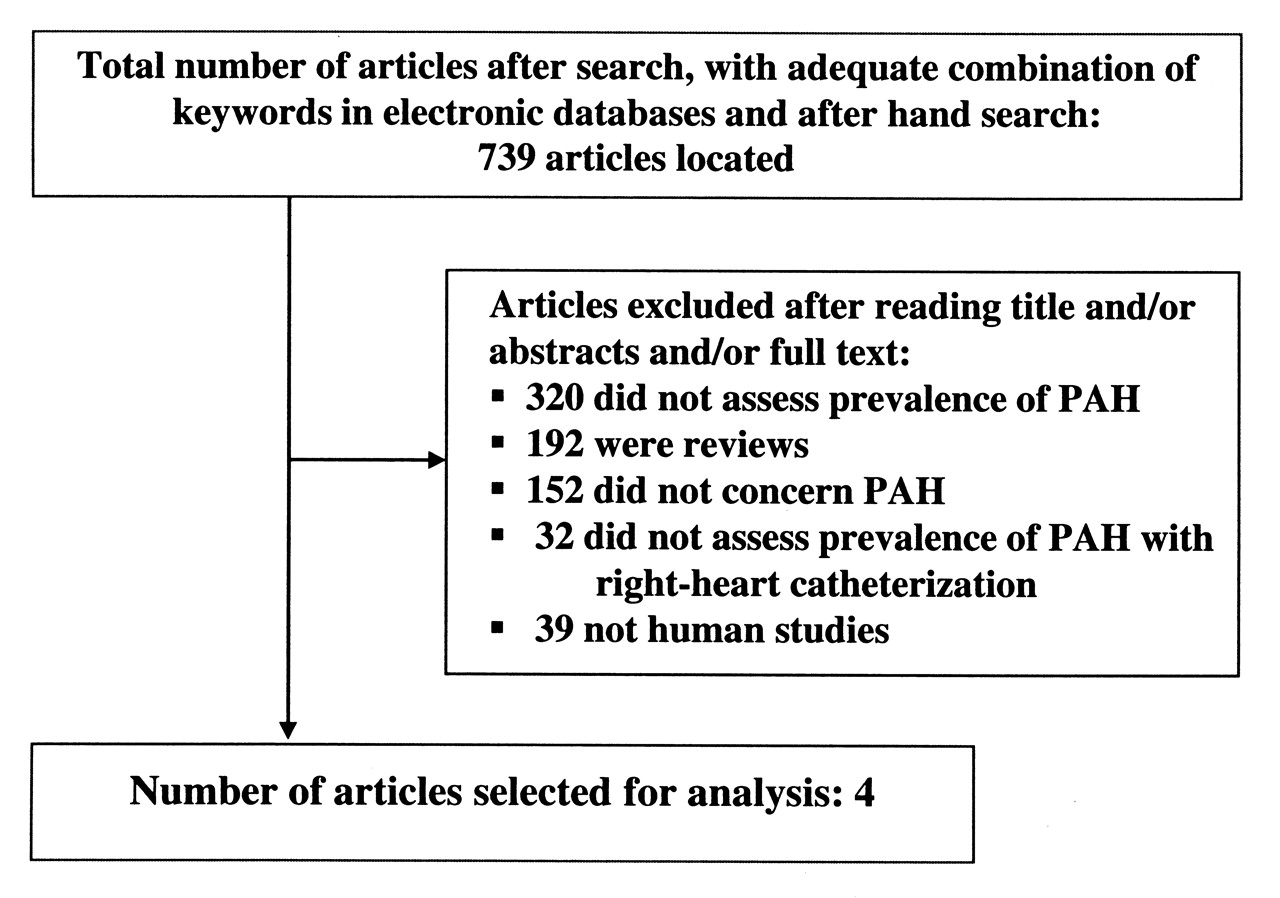
Screening of publications reporting the prevalence of pulmonary hypertension.

Forest plots show prevalence of pulmonary hypertension in the studies included in the metaanalysis.
Characteristics and metaanalysis of studies of patients with SSc and pulmonary hypertension. Values are mean ± SD or number (%) of observations, unless otherwise specified.
DISCUSSION
In this large sample of European Caucasians with SSc, 7% of patients had PH, confirmed by RHC. Among these, 5% had precapillary PH, of whom a majority had PAH. We identified 2 distinct groups of SSc patients at particularly high risk of precapillary PH: (1) patients with the limited cutaneous disease subset, in the late stage of the disease and with a decreased DLCO/AV, were at risk of PAH; and (2) men with the diffuse cutaneous subtype and a decreased DLCO/AV were at risk of PH secondary to ILD. The meta-analysis of 5 studies, including nearly 4000 patients, revealed a 9% point prevalence of precapillary PH, with heterogeneity mainly related to the definition of PH and indications for RHC. The originality of our study lies in the selection of SSc patients for RHC according to recently validated criteria and the absence of exclusion for RHC of patients with ILD18. In our cohort and in the metaanalysis, we also make a clear distinction among patients with precapillary PH, between those with isolated PAH and those with PH secondary to ILD.
The overall point prevalence of precapillary PH was 5% in our combined sample, with a higher prevalence of PAH than PH secondary to ILD, as previously reported7,8. There was no prevalence difference between French and Italian patients, although the Italian sample was older, with higher proportions of limited cutaneous subtype and anticentromere antibodies. In our metaanalysis, the 9% pooled prevalence of precapillary PH was higher than in our study, although the distributions of PAH and PH secondary to ILD were similar (with statistical heterogeneity, however). This may be partially explained by differences in study designs (3 studies were prospective and 2 were cross-sectional), definition of PH (one study excluded patients with ILD), and indications for RHC. Although all studies used Doppler echocardiography to select candidates for RHC, there were disparities among studies in the echocardiographic measurements and thresholds applied to identify potential cases of PH. We used a previously published systolic PAP of 40 mm Hg as a threshold for PH18, a cutoff point supported by other studies, which suggested that a Doppler echocardiographic threshold < 40 mm Hg has a negative predictive value of 92%32,33.
Six patients with DLCO < 50% of predicted, in the absence of pulmonary fibrosis, had confirmed precapillary PH despite normal sPAP. This emphasizes the contribution of DLCO measurement as a screening tool, in addition to echocardiography.
Our results underline the difficulties of echocardiography in making an accurate diagnosis of PH. This method is limited by its low specificity in the presence of left-heart disease and elevated pulmonary capillary wedge pressure, leading to overestimation of the prevalence of PH. This is supported by our 5% prevalence of PH at RHC, compared with 12% at echocardiography. Moreover, the exclusion of left-heart dysfunction may be challenging with echocardiography alone, as illustrated by our data and by 2 prospective studies included in our metaanalysis10,11. Respectively, 17 of 142 (12%), 3 of 33 (9%), and 19 of 147 (13%) SSc patients had PH secondary to left-heart disease at RHC despite the absence of echocardiographic manifestations of left-heart dysfunction. When PH is suspected, these data emphasize the importance of systematically proceeding with RHC, which remains the gold standard for diagnosis1,34,35.
The marked effects of PH on the survival of patients with SSc urgently requires identification of the subset of patients at highest risk, in order to implement an appropriate response. Our observations confirm the strong association between precapillary PH and decreased DLCO/AV. A retrospective case-matched controlled study showed a correlation between progressive decline in DLCO and subsequent development of isolated PAH14. These investigators also showed that patients presenting with limited cutaneous SSc who subsequently developed isolated PAH had a progressive decrease in DLCO that started > 10 years before the diagnosis of PAH. We also confirmed that a decrease in DLCO/AV is a factor strongly associated with PAH, using a threshold value of 70% of predicted18. The mean age of patients with precapillary PH in our study and in the meta-analysis was significantly older than that of patients without PH. This was also the case for patients with postcapillary PH secondary to left-heart disease, as previously shown36. This late onset of PH in patients with SSc may promote complacency among clinicians. However, recent data indicate that PH may affect both sexes at all ages36,37, highlighting the need for a high index of suspicion and routine screening of all patients, to allow an early diagnosis8. The duration of SSc in our study was associated with development of PAH, but not with PH related to ILD. In the meta-analysis, precapillary PH appeared nevertheless to be a late complication of the disease, although no consensus on this has been reached8,13,38. A recent French study showed that the incidence of PAH developing within 5 years after the diagnosis of SSc was approximately 50% among patients with diffuse disease as well as among patients with limited cutaneous SSc38. These observations suggest that all patients should be screened for PH immediately after the diagnosis of SSc has been made39,40. Our data support the impression that PAH develops in patients with the limited cutaneous subset14, although others have suggested that patients with all subtypes are at risk of developing PAH8,10,11. This disagreement may be related to the definition of PH. Although we found no association between precapillary PH and the cutaneous subtype, a subgroup analysis showed that PAH was associated with the limited subset, and PH secondary to ILD with the diffuse cutaneous subset. Moreover, in our study, the antibody subtypes accurately predicted the risk of development of PAH. The anticentromere antibodies in particular, usually detected in the limited cutaneous subset, were positively correlated with development of PAH41,42.
Limitations of our study
This was an observational study. The disease phenotype associations must be interpreted cautiously as the study was cross-sectional. Moreover, the different disease characteristics identified were associated with prevalent PH, and not with incident PH. Thus, groups at risk of prevalent PH may be biased toward survivors, as patients with the diffuse cutaneous subtype have a more fulminant disease course. The exclusion from RHC of patients with DLCO < 50% of predicted with pulmonary fibrosis and normal sPAP on echocardiography may have underestimated the prevalence of PH secondary to ILD. However, these 32/1165 (3%) patients had a low suspicion of PH, as their sPAP ranged from 22 to 33 mm Hg.
All patients in our study were European Caucasians. More studies are needed to confirm these results in other ethnic groups. SSc patients were recruited by tertiary medical centers, and therefore might have had more active and severe disease than patients at less specialized centers. On the other hand, all recruiting centers are highly active in the field of SSc clinical research, which guaranteed a high quality and accuracy of the data collected. Finally, the reliability of the Doppler echocardiographic examinations is pivotal, and the experience of the echocardiography specialist is critical in accurate measurement of sPAP.
In the metaanalysis, it is noteworthy that we could not identify the factors associated with PAH and PH secondary to ILD, as we had no access to individual data.
In summary, our study shows that 7% of this large sample of European Caucasians with SSc had PH. Among them, 5% had precapillary PH. Our metaanalysis of 5 studies found a 9% pooled prevalence of precapillary PH, with distributions of PAH and PH secondary to ILD similar to those observed in our study, although they were markedly heterogeneous. In more than 50% of patients in whom it was suspected, precapillary PH was not confirmed by RHC, which strongly supports the validity of performing this definitive examination. Our analysis also identified subgroups of patients at particularly high risk of PH according to age, disease duration, cutaneous disease subtype, or antibody status, and these should be carefully monitored.
Acknowledgment
We thank Prof. Emmanuel Touzé, Neurologie Sainte Anne Hospital, Paris, for helpful contribution in the performance of the prevalence metaanalysis.
- Accepted for publication June 10, 2010.








{kind=link}
{kind=link}
{kind=link}