

Abstract
Objective. To determine whether the mortality in a cohort of patients with psoriatic arthritis (PsA) from a single center in the UK is significantly different from the general UK population.
Methods. Patients who were entered onto the PsA database at the Royal National Hospital for Rheumatic Diseases, Bath, between 1985 and 2007 were included in this study. Information on patient deaths was collected retrospectively. The National Health Service (NHS) Strategic Tracing Service was used to establish which patients were alive and which had died. Date and cause of death were confirmed by death certificates from the Registry of Births, Marriages and Deaths. A standardized mortality ratio (SMR) was calculated by matching the patient data to single-year, 5-year age-banded England and Wales data from the Office of National Statistics.
Results. In this cohort of 453 patients with PsA (232 men, 221 women), there were 37 deaths. Sixteen men and 21 women died. The SMR for the men was 67.87% (95% CI 38.79, 110.22), and for the women, 97.01% (95% CI 60.05, 148.92) and the overall SMR for the PsA cohort was 81.82% (95% CI 57.61, 112.78). The leading causes of death in this cohort were cardiovascular disease (38%), diseases of the respiratory system (27%), and malignancy (14%).
Conclusion. These results suggest that mortality in our single-center PsA cohort is not significantly different from the general UK population. No increased risk of death was observed in this cohort.
Psoriatic arthritis (PsA) is a chronic inflammatory arthritis associated with psoriasis with an estimated incidence rate of up to 6.6 per 100,000/year1,2,3,4. While previously thought to be a benign arthropathy, PsA is now known to be associated with significant joint damage and disability5,6,7,8.
In recent years, it has been firmly established that rheumatoid arthritis (RA) is associated with increased mortality, particularly due to cardiovascular disease9,10. Longterm outcome, including mortality, in other forms of inflammatory joint disease has been the subject of fewer studies. Such studies in PsA have thus far shown conflicting results, with a community-based study showing no increase in mortality2,3 while analysis of a hospital- based cohort estimated a combined standardized mortality ratio (SMR) for both men and women to be 1.6211. Cardiovascular disease was the commonest cause of death in the latter study.
Patients with PsA have been found to have increased cardiovascular risks12. PsA is associated with increased incidence of subclinical atherosclerosis13,14 and an atherogenic lipid profile has been identified in active PsA15. There is increased prevalence of the metabolic syndrome in patients with psoriasis, particularly in those with moderate to severe skin disease16. Therefore, increased mortality in PsA, particularly due to cardiovascular disease, would not be entirely unexpected.
In an attempt to further clarify this issue, we examined whether mortality in our PsA cohort is significantly different from the general UK population.
MATERIALS AND METHODS
A PsA clinic was established in the Royal National Hospital for Rheumatic Diseases (RNHRD), Bath, in 1985. The majority of the patients attending the clinic came from Bath and the surrounding area. Initially, most of the cohort (> 70%) was recruited from other rheumatology clinics at the RNHRD while a proportion of them were new referrals from primary care. In later years the proportion referred directly from primary care increased (> 70%). A small number of patients were referred directly from dermatology (< 20%). Patients attending the clinic were invited to be entered onto a PsA database. All patients who were entered onto the database between 1985 and 2007 were included in this study. Any patients entered onto the study needed to fulfil diagnostic criteria for PsA, which until 2007 were according to Moll and Wright17. From 2007 patients were required to fulfill ClASsification of Psoriatic ARthritis study group criteria18 for inclusion.
The NHS Strategic Tracing Service was used to establish which patients had died. The status of every patient in the cohort was confirmed using this service, a practice that ensured that all deaths in the cohort were recorded. Date and cause of death was confirmed by obtaining death certificates from the Registry of Births, Marriages, and Deaths.
To determine whether there was a difference in the mortality in our cohort and that of the general UK population, data on 453 patients from the PsA cohort was matched to single-year, 5-year age-banded England and Wales data from the Office of National Statistics. SMR were calculated separately for men and women and an overall SMR for the total cohort was also calculated.
RESULTS
The study population consisted of 453 patients, 232 of whom were men (51.2%) and 221 of whom were women (48.8%). All patients were traced and whether they were living or dead was confirmed by the NHS Strategic Tracing Service. The dataset was therefore complete and there was no loss to followup. The minimum duration of followup was 1 year. There were 37 deaths in the cohort; 21 women and 16 men. The total number of person-years of followup was 3738 (men 1924 and women 1814). The median age at recruitment to the cohort was 49 years. The median age at onset of psoriasis was 29 years. Onset of PsA occurred at a median age of 38 years. Median age of death was 74 years (interquartile range 64–82 years). The patients who died appeared to be older at recruitment to the cohort than those who remained alive. Also, the patients who died were older at onset both of psoriasis and PsA. However, the overall number of deaths in the cohort was small, so any differences between the characteristics of the living and the dead patients must be interpreted with caution. The characteristics of our cohort are described in Tables 1 and 2.
Cohort demographics.
Median ages of cohort.
Table 3 shows the sex-specific and overall SMR in our PsA cohort compared with the general UK population for the study period 1985–2007.
Standardized mortality ratios (SMR) in the psoriatic arthritis cohort compared with the general UK population.
The ratio of observed to expected deaths did not show an increased risk of death in our PsA cohort, with an SMR of 67.87% for men and 97.01% for women. The combined SMR for men and women was 81.82%. Due to the low number of deaths in the cohort, the CI were wide. Because the 95% CI spanned 100, there was no evidence of an increased risk of death in this cohort at the 5% significance level.
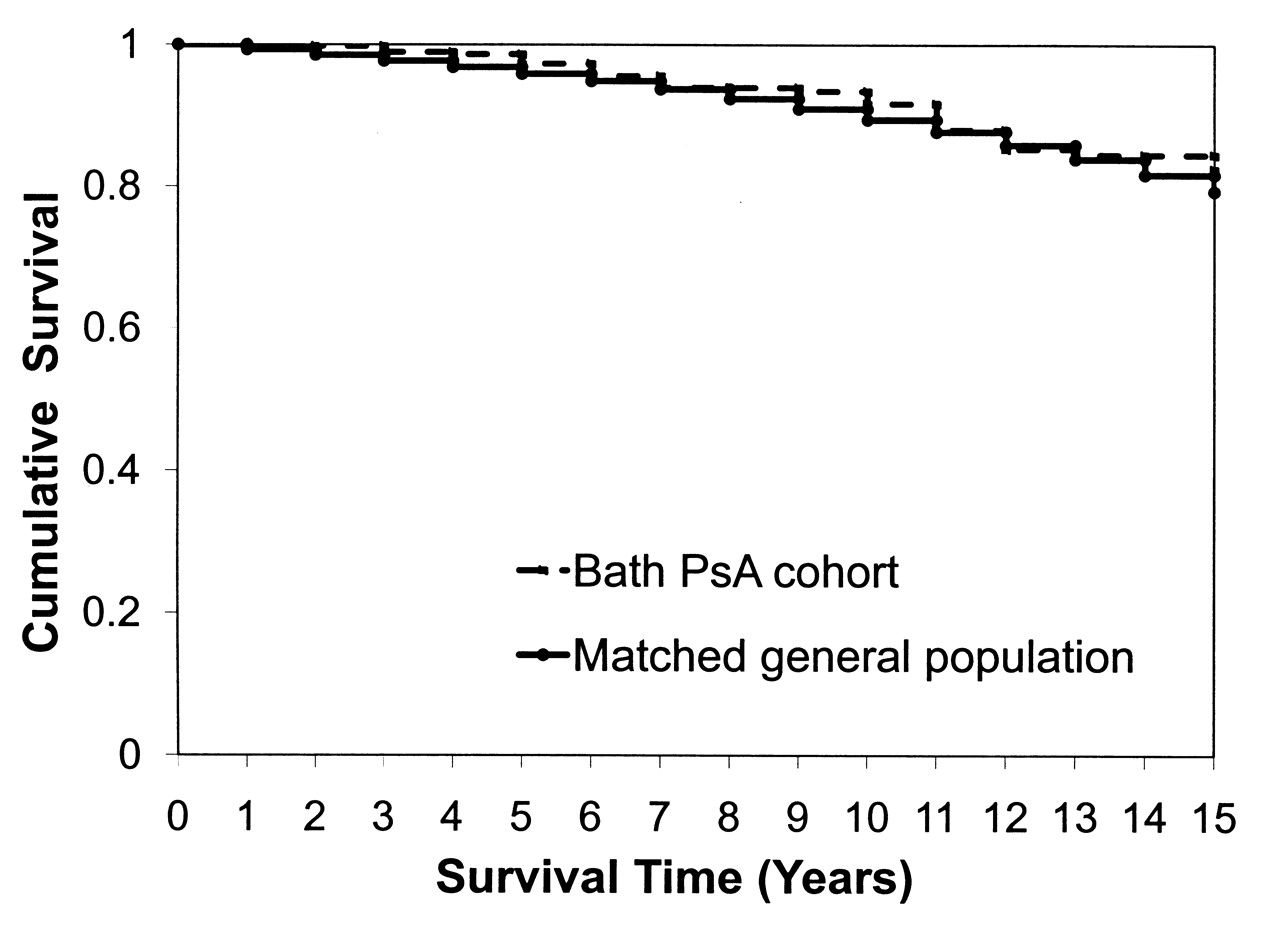
Survival for patients in our PsA cohort was not significantly different from the general UK population (Figure 1).

15-year Kaplan-Meier survival curve. Observed survival in Bath psoriatic arthritis cohort compared to survival in a matched UK population.
Deaths and causes of death were verified by death certificate for all 37 deaths in our cohort. Cardiovascular disease was the commonest cause of death at 38%, followed by respiratory disease (27%) and malignancy (14%). The low total number of deaths in this cohort did not allow comparison of rates of deaths due to specific causes with death rates in the general UK population.
DISCUSSION
Over the past decade there has been more recognition of increased mortality associated with chronic inflammatory conditions. Increased mortality was initially noted in RA and was found to be largely due to increased cardiovascular mortality10. Mortality studies have also been carried out in other inflammatory arthritides, including PsA11,19,20.
To date, information on mortality in PsA is sparse and conflicting. Roberts, et al reported 18 deaths in a cohort of 168 patients with PsA in 197621, and Coulton reported no deaths in a followup study of a hospitalized cohort in 198922. Both these studies had unclear inclusion criteria and were not blinded or controlled. Shbeeb, et al, did not find a significant increase in mortality in patients with PsA in their analysis of a population- based cohort in Olmsted County, Minnesota, USA2. A later study by the same group confirmed this finding3. However, a mortality study from the University of Toronto Psoriatic Arthritis Clinic found patients with PsA to be at increased risk of death compared to the general Ontario population11. This study found a combined SMR for both men and women of 1.62 (95% CI 1.21, 2.12). A subsequent study in 2007 from the same cohort did, however, show a trend toward improved survival over the past 3 decades20.
Our study did not demonstrate any significant difference in mortality between our PsA cohort and that of the general UK population. The status of all 453 patients was ascertained using the NHS Strategic Tracing Service, so there was no loss to followup. Therefore we were able to generate a complete dataset that allowed us to calculate an accurate SMR. Even so, the total number of deaths in the cohort was small (16 men and 21 women) and no more than expected in the general population.
Further, our results represent a different trend to that seen in the original Toronto cohort. Our cohort was drawn mainly from primary care and may therefore have included a higher proportion of patients with milder disease. Earlier referral may also have allowed us to manage our patients with PsA aggressively at an early stage, a practice that may affect subsequent disease. Risk factors for mortality have been found to be related to severity19; and so earlier intervention with disease-modifying agents could lessen progression of disease and severity and could thereby explain the trend toward improved survival in our cohort. Also, it is possible that patients destined to have greater mortality may not have been referred to the clinic due to the severity of comorbid disease. Fewer sicker patients would potentially skew our population toward those with better overall health, which in turn could influence the mortality.
The cohort was entirely white, which may limit the degree to which the results can be applied to the general UK population. In comparison with the general population, deaths due to malignancy (14%) were reduced in our cohort23. It must, however, be borne in mind that the total number of deaths in our cohort was low, so it is difficult to draw reliable conclusions on differences in cause of death between our cohort and the general UK population.
Mortality studies in rheumatological disease have tended to focus on cardiovascular disease, and although the overall number of deaths in our cohort was low, the commonest cause of death was cardiovascular disease. In RA and systemic lupus erythematosus, there is an association between systemic inflammation and atherosclerosis, possibly through cytokine pathways common to both disorders24. Systemic inflammation with involvement of organs apart from the musculoskeletal system or skin is not such a prominent feature of PsA. However, an increased prevalence of cardiovascular disease has been reported in psoriasis25,26. Psoriasis is also associated with increased prevalence of the metabolic syndrome16, which is a risk factor for cardiovascular disease. Severity of skin disease has been shown to correlate with the prevalence of subclinical atherosclerosis26. In patients with PsA it is possible that skin disease and its strong association with the metabolic syndrome has a greater influence than joint inflammation on cardiovascular mortality. Indeed, in a recent study from the Toronto group, it is noteworthy that higher cardiovascular disease in PsA was associated with more extensive skin disease as well as diabetes and hyperlipidemia27. In our study, severity of skin disease was not recorded until more recently. However, our finding of reduced mortality compared with previous studies could potentially be explained by milder psoriatic skin disease.
Our study adds to the ongoing debate around the issue of mortality in PsA. We did not find a significant difference between mortality in our PsA cohort and that of the general population. However, given the low number of deaths in our cohort, ongoing research into mortality in PsA in a larger cohort is warranted, as is the issue of whether the metabolic syndrome is solely associated with psoriasis rather than with arthritis.
Footnotes
-
Partly supported by an unrestricted grant from Abbott Laboratories.
- Accepted for publication May 20, 2010.








{kind=link}