

Abstract
Objective. To investigate the response to therapy of entheseal abnormalities assessed with power Doppler (PD) ultrasound (US) in spondyloarthropathies (SpA).
Methods. A total of 327 patients with active SpA who were starting anti-tumor necrosis factor (TNF) therapy were prospectively recruited at 35 Spanish centers. A PDUS examination of 14 peripheral entheses was performed by the same investigator in each center at baseline and at 6 months. The following elementary lesions were assessed at each enthesis (presence/absence): morphologic abnormalities (hypoechogenicity and/or thickening), entheseal calcific deposits, cortical abnormalities (bone erosion and/or proliferation), adjacent bursitis and intraenthesis and perienthesis (tendon body and/or bursa) PD signal. Response to therapy of each elementary lesion was assessed by calculating change in the cumulative presence from baseline to 6 months. Intraobserver reliability of PDUS was evaluated by blindly assessing the stored baseline images 3 months after the real-time examination.
Results. Complete data were obtained on 197 patients who received anti-TNF therapy for 6 months. In 91.4% of the patients there were gray-scale or PD elementary lesions at baseline and at 6 months. Cumulative entheseal morphologic abnormalities, intraenthesis PD, perienthesis PD, and bursitis showed a significant decrease from baseline to 6 months (p < 0.05). There was high intraobserver reliability for all elementary lesions (interclass correlation coefficient > 0.90, p < 0.0005).
Conclusion. Entheseal morphologic abnormalities, PD signal, and bursitis were US abnormalities that were responsive to anti-TNF therapy in SpA. PDUS can be a reproducible method for multicenter monitoring of therapeutic response in enthesitis of SpA.
Entheses are the sites where tendons, ligaments, muscle, fascia, or joint capsules are attached to the bone1. Inflammation of entheses or enthesitis is a pathological feature of spondyloarthropathies (SpA)2,3. Histological studies on enthesitis have described local inflammation, fibrosis, erosion, and ossification. Inflammation of adjacent bursae may also occur in enthesitis1.
Enthesitis has been classically diagnosed by physical examination for the presence of subjective tenderness at entheseal areas. Conventional radiography shows chronic bone changes in enthesitis such as proliferation or erosions. Both magnetic resonance imaging (MRI) and ultrasound (US) allow us to objectively detect a spectrum of early and late changes in enthesitis4,5. MRI is limited for clinical use because of its limited availability and high cost. US with Doppler technique is a sensitive and reliable imaging modality for assessing morphological changes and abnormal blood flow at the peripheral entheses6,7,8,9,10,11,12,13. US has been shown to detect subclinical enthesitis, mainly in lower limbs of patients with SpA8,9,10,14,15. In addition, this technique is noninvasive, more widely available, relatively inexpensive, and patient-friendly in clinical practice.
Studies have described a number of gray-scale US abnormalities in peripheral entheses in SpA6,7,8,9,10,11,12,13,14,15. These have consisted of a loss of normal fibrillar echotexture, a decrease in enthesis echogenicity, an increase in enthesis thickness, calcific deposits at the insertion of the tendon, adjacent bursitis, periosteal formation, and bone erosions. In some studies, enthesis thickening, hypoechogenicity, echotexture abnormality, and bursitis have been considered signs of inflammation, whereas calcific deposits and bone abnormalities have been considered signs of consequent structural damage10,12,13. However, this classification of entheseal lesions has not been validated in any study.
The power Doppler (PD) technique has demonstrated its capacity to detect abnormal vascularization at the enthesis and adjacent to the enthesis in SpA9,11,12,13,16. The presence of PD signal at the cortical bone insertion has not been found in healthy controls17 and has been shown to be specific for peripheral SpA enthesitis9.
In 2005, the Outcome Measures in Rheumatology (OMERACT) group for musculoskeletal US defined enthesopathy as abnormally hypoechoic (loss of normal fibrillar architecture) and/or thickened tendon or ligament at its bony attachment (may occasionally contain hyperechoic foci consistent with calcification), seen in 2 perpendicular planes that may exhibit Doppler signal and/or bony changes including enthesophytes, erosions, or irregularity18. Various cross-sectional studies have proposed reliable US scoring systems of enthesitis, which have consisted of a variable sum of presence or grading of elementary lesions found in SpA entheses8,9,10,11,12,13,16. These scoring systems have been developed mainly for diagnostic purposes9,10,11. However, there are few longitudinal studies on the response to therapy of gray-scale or PD entheseal abnormalities in SpA19,20. Our multicenter study was undertaken to investigate the response to therapy and reproducibility of PDUS abnormalities in entheses of patients with active SpA who began anti-tumor necrosis factor (TNF) therapy.
MATERIALS AND METHODS
This study was conducted by the Ultrasound Group of the Spanish Society of Rheumatology. Three hundred twenty-seven patients (230 men, 97 women) with SpA according to the European Spondylarthropathy Study Group criteria21 or the criteria of Amor, et al22 were prospectively recruited at 35 Spanish centers, from March 2007 to October 2008.
Patients were additionally classified as having ankylosing spondylitis (AS), according to the modified New York criteria23; reactive arthritis (ReA), according to the criteria of Willkens, et al24; psoriatic arthritis (PsA) or arthritis-associated inflammatory bowel disease (IBD) if psoriasis or IBD, respectively, was present; and undifferentiated SpA if the SpA criteria were fulfilled, but no diagnosis of AS, PsA, ReA, or arthritis-associated IBD could be established.
All patients were beginning therapy with a TNF-blocking agent, according to Spanish and international consensus on the use of biologic agents for the treatment of SpA25,26. The study was conducted in accord with the Declaration of Helsinki and was approved by the local ethics committees. Informed consent was obtained from all patients before study enrollment.
The patients underwent a clinical, laboratory, and PDUS evaluation at baseline and at 6 months. Therapeutic decisions were made throughout the followup period depending on the SpA clinical course without knowledge of the PDUS findings.
Clinical and laboratory assessment
Clinical data were obtained by a rheumatologist at each center who was blinded to the PDUS findings. The following data were recorded for each patient at study entry: age; sex; symptom duration; use of nonsteroidal antiinflammatory drugs (NSAID), corticosteroids, disease-modifying antirheumatic drugs (DMARD), and anti-TNF agents received for SpA; and HLA-B27 status. At each visit, the Spanish versions of the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and the Bath Ankylosing Spondylitis Functional Index (BASFI) were recorded using visual analog scales. In addition, tenderness at 13 entheses [Maastricht Ankylosing Spondylitis Enthesitis Score (MASES)27] was investigated. Data on serum markers of inflammation, C-reactive protein (CRP) level (normal 0–10 mg/l), and erythrocyte sedimentation rate (ESR; normal 10–20 mm/h) were obtained from laboratory tests performed within 48 hours of each clinical visit.
PDUS assessment
Patients underwent a PDUS assessment within 4 hours of each clinical evaluation by the same rheumatologist experienced in this technique at each center. These rheumatologists were unaware of the clinical and laboratory findings and were not involved in the treatment decisions. To reduce the possibility of bias, the patients were asked not to discuss their clinical symptoms with the US examiner, and the PDUS examination was carried out in a darkened room.
Systematic longitudinal and transverse multiplanar PDUS examination of 14 peripheral entheses was carried out with the same real-time scanner in all centers (Logiq 5 PRO; General Electric Healthcare, Kyunnggi-do, Korea) using multifrequency linear array transducers (7–12 MHz). PDUS assessment included the following bilateral entheses: lateral epicondyle; medial epicondyle; quadriceps tendon; proximal patellar tendon; distal patellar tendon; Achilles tendon; and plantar fascia. US scanning technique, gray-scale and PD machine settings, and definitions of abnormality were standardized among investigators prior to the study. The PDUS scanning method is described in Table 1. The same gray-scale and PD settings were used at baseline and at followup for each entheseal site. The entheses at anatomic areas that had undergone surgical procedures were not evaluated.
Power doppler ultrasound (PDUS) scanning method of the entheses.
PD assessment was performed by selecting a region of interest that included the bony margins, entheseal site, and a variable view of surrounding tissues. Pulse repetition frequency was adjusted to the lowest permissible value to maximize sensitivity. This setting resulted in pulse repetition frequency of 500 Hz. Low-wall filters were used. The dynamic range was 40 dB. Color gain was set just below the level at which color noise appeared underlying bone (no flow should be visualized at bony surfaces). This setting resulted in gains of 30 dB. Flow was additionally demonstrated in 2 planes and confirmed by pulse wave Doppler spectrum to exclude artefacts.
At each enthesis, the following elementary lesions were assessed (presence/absence): (1) entheseal morphologic abnormalities (i.e., hypoechogenicity and/or thickening); (2) entheseal calcific deposits; (3) entheseal cortical abnormalities (i.e., bone erosion and/or enthesophytes); (4) adjacent bursitis; (5) intraenthesis PD signal at the cortical bone insertion; and (6) perienthesis PD signal at tendon body and/or bursa. A cumulative score for each elementary lesion was calculated by summing separately the entheses that showed each of them.
Enthesis thickening and hypoechogenicity were evaluated relative to the body of the tendon. Calcific deposit at the enthesis was defined as hyperechoic spots or lines at the preinsertional area of the tendons, with or without acoustic shadowing, seen in 2 perpendicular planes. Bone erosion was defined as a discontinuity of the entheseal bone surface, seen in 2 perpendicular planes. Enthesophyte was defined as a hyperechoic prominence at the end of the entheseal bone contour, seen in 2 perpendicular planes. Bursitis was defined as a well circumscribed hypoechoic or anechoic collection at the site of an anatomic bursa.
Intraobserver reliability of PDUS
Intraobserver reliability of the PDUS assessment was evaluated by recording representative images from the full baseline examination of the patients included in the study. The stored images from each patient were evaluated under blinded conditions by the same investigator who performed the corresponding real-time PDUS examination a minimum of 3 months later.
Statistical analysis
Statistical analysis was performed using SPSS, version 13.0 (SPSS, Chicago, IL, USA). Quantitative variables were presented as the mean ± SD and range. Paired-samples t test was used for comparing baseline and 6 month followup mean values for quantitative variables. McNemar’s test was used for comparing baseline and 6 month percentages of entheseal abnormalities. Correlations between clinical, laboratory, and PDUS parameters were analyzed by Pearson’s correlation coefficient.
Intraobserver reliability for each elementary lesion score was evaluated by calculating the intraclass correlation coefficient (ICC; 2-way mixed effects). An ICC value < 0.40 was considered poor, 0.40–0.50 moderate, 0.50–0.70 good, and 0.70–1.0 excellent.
RESULTS
Patient characteristics
Three hundred twenty-seven patients with SpA (230 men, 97 women; mean ± SD age 44.5 ± 11.3 yrs) who were starting therapy with adalimumab [264 (80.7%) patients], infliximab [33 (10.1%) patients], or etanercept [30 (9.2%) patients] were prospectively included in the study. Twenty-three patients (7%) had received 1 previous anti-TNF agent and 2 (0.6%) had received 2 previous biologic agents. These patients had been switched to another TNF-blocking agent because of inefficacy (21 patients) or adverse effects (4 patients).
To homogenize the cohort, we analyzed data from only those patients who had received uninterrupted anti-TNF therapy for the 6 month followup period. Seventy (21.4%) patients were switched to another TNF-blocking agent during the study because of inefficacy [56 (17.1%) patients] or adverse effects [14 (4.3%) patients]. Sixty (18.3%) patients missed the followup visit. Complete clinical, laboratory, and PDUS data were obtained on 197 SpA patients (139 men, 58 women). The mean age of these patients was 44.5 ± 11.1 years (range 18–74), and the mean disease duration was 10 ± 8.9 years (range 0.2–50.3). One hundred thirty-five (68.5%) patients had been classified as having AS; 34 (17.3%) PsA; 16 (8.1%) undifferentiated SpA; 11 (5.6%) arthritis-associated IBD; and 1 (0.5%) ReA. One hundred thirty-three (67.5%) patients were HLA-B27-positive.
At inclusion to study, 39 patients (19.8%) were taking methotrexate, 25 (12.7%) were taking sulfasalazine, and 14 (7.2%) were taking other DMARD. One hundred eighty (91.4%) patients were taking NSAID, and 35 (17.8%) were taking prednisone. Three patients had undergone previous knee surgery.
Disease activity and functional course
A significant decrease in the mean BASDAI, BASFI, and MASES was found at the followup assessment (p < 0.0005). At study entry, the mean BASDAI was 5.83 ± 1.48 (range 2.1–9.2) and the mean BASFI was 5.43 ± 2.17 (range 0–9.6). At 6 months, the mean BASDAI was 3.22 ± 2.16 (range 0–9.4) and the mean BASFI was 3.61 ± 2.60 (range 0–9.9). MASES decreased from 3.96 ± 3.22 (range 0–12) at baseline to 2.52 ± 2.80 (range 0–13) at 6 months (Table 2).
Changes in clinical measures and ultrasonography elementary lesion scores from baseline to 6 months.
PDUS abnormalities
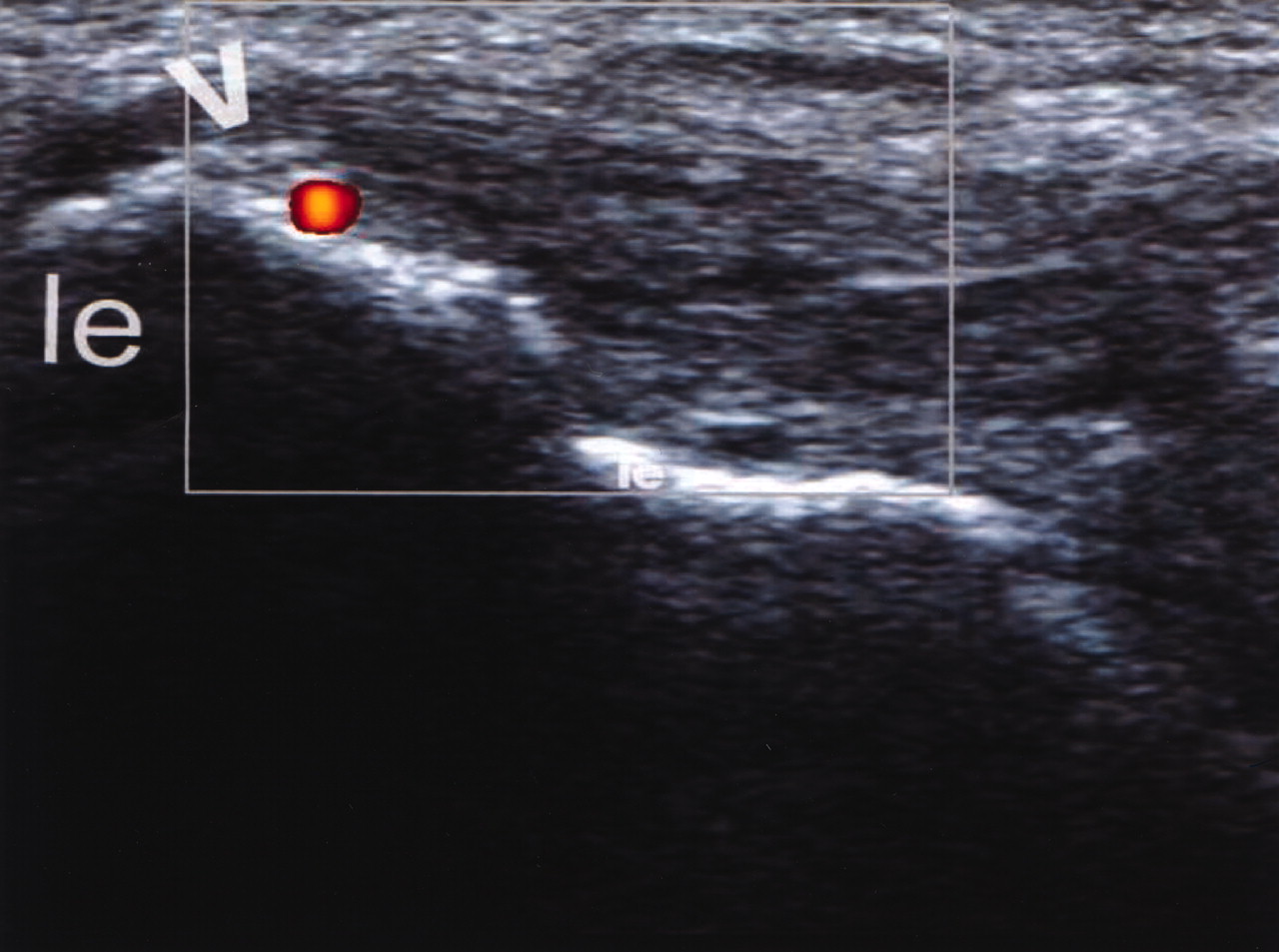
In 91.4% of the patients there were gray-scale or PD abnormalities at baseline and 6 months. These abnormalities were detected in a mean of 5.7 ± 3.8 (range 0–14) entheses at baseline and in a mean of 5.5 ± 3.8 (range 0–14) entheses at 6 months. The percentages of patients who showed each elementary lesion at any enthesis at baseline and 6 months are shown in Table 3. The overall frequency of each elementary lesion at each bilateral enthesis at baseline and 6 months is shown in Table 4. A representative PDUS image of entheseal abnormalities in SpA is shown in Figure 1.

Longitudinal ultrasonography image of the common extensor tendon at the lateral epicondyle of the elbow. The enthesis shows abnormal thickening and hypoechogenicity, calcific deposits (arrowhead), and intraenthesis power Doppler signal. le: lateral epicondyle.
Percentage of patients who showed each elementary lesion at any enthesis.
Changes in bilateral enthesis involvement by each elementary lesion (EL) at baseline and at 6 months.
Course of PDUS elementary lesions
Mean changes in the cumulative elementary lesions from baseline to 6 months are shown in Table 2. The morphologic abnormality score, intraenthesis PD score, and perienthesis PD score showed a highly significant decrease from baseline to 6 months (p < 0.0005). The adjacent bursitis score also decreased significantly (p = 0.036), whereas the calcific deposit score and cortical abnormality score increased throughout the followup period. The total number of entheses that presented morphologic abnormalities, intraenthesis PD, and perienthesis PD decreased significantly from baseline to 6 months at most sites (p < 0.05; Table 4). The overall numbers of bursitis adjacent to the Achilles tendon were also significantly reduced after 6 months of therapy (p = 0.036; Table 4).
The elementary lesion scores and the clinical (BASDAI, BASFI, MASES) and laboratory (CRP, ESR) measures did not correlate at baseline and 6 months. There was no correlation between changes in the elementary lesion scores and changes in the clinical and laboratory variables throughout followup (data not shown).
Intraobserver reliability of the PDUS assessment
Table 5 shows the intraobserver ICC for each elementary lesion score. All ICC were significantly > 0.90, reflecting a high degree of intraobserver reliability.
Intraobserver reliability of the elementary lesion scores.
DISCUSSION
Peripheral enthesitis can be present in all SpA subtypes. It may be either a relevant clinical manifestation or it may be asymptomatic. Gray-scale US provides information on morphologic and structural involvement of enthesis, and PDUS detects abnormal vascularization in the inflamed enthesis6,7,8,9,10,11,12,13,14,15,16. In addition, asymptomatic enthesitis can be detected with US in SpA patients8,9,10,14,15. Consequently, US imaging of enthesis could be incorporated as a complementary procedure into the overall assessment of involvement and disease activity of SpA, as well as monitoring of response to therapy.
Investigators have proposed gray-scale and/or PD scoring systems for enthesitis based on cross-sectional studies in SpA8,9,10,11,12,13,16. These scoring systems have consisted of cumulative qualitative8,9,10,11,12,13 and/or semiquantitative grading11,12,13,16 of elementary lesions at selected entheses, most of them in the lower limbs in patients with SpA. They have been used to demonstrate diagnostic value for SpA9,10,11, reliability8,9,10,11,12,13,16, or correlation with clinical assessment of enthesitis16.
PDUS changes after anti-TNF therapy in heel entheses have been reported in a reduced number of patients with SpA20. However, to our knowledge, our study is the first that has separately evaluated response to therapy of different PDUS abnormalities in a large multicenter cohort of patients with active SpA who were beginning anti-TNF therapy. This treatment has been widely demonstrated to be effective in SpA28,29,30,31.
For this study, we selected 14 peripheral entheses easily accessible to US and frequently chosen in previous studies6,7,8,9,10,11,12,13,14,15. Our results were in accord with previous studies that reported a high prevalence of abnormal US entheseal findings in patients with SpA9.
We evaluated enthesis hypoechogenicity and thickening together, because both have been considered morphologic signs of acute inflammation13, and because both are essential elementary lesions in the OMERACT definition of enthesopathy18. We included bone erosions and enthesophytes in the same elementary lesions because both are chronic structural changes produced by inflammation, and because enthesophytes and erosions are easily misinterpreted when both are present at the enthesis.
Morphologic abnormalities and PD signal demonstrated a highly significant improvement from baseline to 6 months of anti-TNF therapy. Bursitis adjacent to Achilles tendon also showed a significant improvement throughout followup. Calcific deposits and cortical abnormalities worsened throughout the followup period, in spite of the therapy. Our findings confirmed that morphologic abnormalities, PD signal, and bursitis can be considered active inflammatory lesions responsive to anti-TNF agents, whereas calcific deposits and cortical abnormalities should be considered structural damage not responsive to inflammation-targeted treatment.
Intraenthesis PD signal at the cortical bone insertion and perienthesis PD signal at tendon body and/or bursa were recorded independently in this study. The presence of PD signal at the cortical bone insertion has been shown to be a diagnostic hallmark of peripheral SpA enthesitis9. In the study by Morel, et al17, no vascularization was detected with contrast-enhanced US at the cortical bone insertion of normal heel enthesis, whereas some vascularization could be seen in proximity to these entheses. However, detection of flow at the cortical bone requires US machines with more sensitive Doppler technology than detection of perienthesis flow. In addition, the border of the true enthesis is not always easy to delimit with PDUS. Further studies should investigate if intraenthesis PD signal has an added prognostic value over perienthesis PD signal in the outcome of SpA.
In keeping with other reports8,9,10,11,12,13,16, we obtained excellent PDUS reproducibility in image interpretation for all elementary lesions. Most previous studies have tested intraobserver and/or interobserver reliability on recorded US images8,9,11,16. Other investigators obtained good image acquisition and interpretation reproducibility for detecting and scoring SpA enthesitis after standardization of the scanning technique, definition of abnormalities, and scoring system10,12,13.
Consistent with the previous findings8,10,15, we found no correlation between clinical and laboratory measures and PDUS abnormalities. As Lehtinen, et al19 described in a cohort of SpA patients treated with sulfasalazine, changes in entheseal abnormalities did not correlate with changes in clinical and laboratory measures. We did not take into account peripheral arthritis or axial involvement (e.g., sacroiliac joint) in the US assessment. Possibly due to this, there was no correlation between US entheseal findings and clinical (BASDAI, BASFI) and laboratory (CRP, ESR) measures. It is noteworthy that, despite evaluation of different entheses, there was no correlation between MASES and PDUS findings. Responsive PDUS abnormalities seemed to be markers of SpA activity independent of conventional clinical and laboratory indicators.
Some limitations of our study should be noted. The study was conducted in accord with daily clinical practice. In addition to anti-TNF therapy, patients were treated with NSAID and various DMARD at different dosage levels during the followup period. These differences in treatment could have introduced bias into the findings. However, since anti-TNF therapy was indicated because SpA remained active despite treatment with NSAID and DMARD, it may be accepted that changes in clinical and PDUS measures were due mainly to the anti-TNF treatment.
Intraobserver reliability was assessed on static images instead of on real-time US scanning. The absence of data on variability of US image acquisition may have overestimated our high reproducibility. In addition, interobserver reliability was not evaluated. However, the number of investigators involved in the study made it unfeasible to undertake real-time intraobserver-interobserver reliability assessment on SpA patients.
The objective of our study was to identify entheseal abnormalities that could be sensitive to change for monitoring response to therapy at the enthesis level in SpA. A semiquantitative score of responsive entheseal abnormalities would probably have improved the sensitivity to change of PDUS assessment. However, appropriate training and implementation of agreed rules for semiquantitative scoring of elementary entheseal lesions was not feasible. Further longitudinal studies using semiquantititive scores of the responsive entheseal lesions are warranted.
Entheseal morphologic abnormalities, PD signal, and adjacent bursitis in SpA seem to be responsive PDUS abnormalities. Good reproducibility of PDUS for assessing abnormalities in SpA entheses, as previously reported, was also demonstrated in this multicenter study. Our results may contribute to development of a cumulative scoring system of combined semiquantitative responsive elementary lesions at the patient level that could be used to monitor therapeutic responses in patients with SpA.
Acknowledgment
We thank the rheumatologists from the study centers who performed the clinical assessments. We gratefully acknowledge Dr. Jesús Garrido, Department of Methodology of the Universidad Autónoma de Madrid, for the statistical analysis.
Footnotes
-
Supported by a grant from Abbott Laboratories. Dr. Naredo has received an honorarium from Abbott Laboratories for coordinating this study.
- Accepted for publication June 3, 2010.








{kind=link}