

Abstract
Objective. There is controversy whether older-onset systemic lupus erythematosus (SLE) is associated with a different, more benign disease course than in younger-onset SLE. Our objective was to characterize the clinical features and prognosis of late-onset SLE in a large, multicenter cohort.
Methods. We studied adult-onset lupus in the 1000 Canadian Faces of Lupus cohort (n = 1528) of whom 10.5% had onset at age ≥ 50 years versus a control group with onset at < 50 years.
Results. Disease duration was different in early- and late-onset groups (15 yrs in early vs 9.3 yrs in late; p < 0.001). Caucasians were represented more in the later-onset SLE group (55.6% vs 74.5%), while Asians and Blacks were more prevalent in the younger group. Younger-onset SLE subjects fulfilled more American College of Rheumatology criteria for SLE (< 50 yrs: 5.98 ± 1.68; ≥ 50 yrs: 5.24 ± 1.44; p < 0.0001). Despite an equal prevalence of anti-dsDNA, the younger-onset group more often had positive anti-Smith autoantibody, ribonucleoprotein, and hypocomplementemia, and more nephritis, rash, and cytopenias than the older-onset group. However, disease activity and damage accrual were higher in the older-onset group. The older patients received less prednisone and immunosuppressives (current and ever-use). As expected, comorbidity was higher in the older-onset SLE group.
Conclusion. This study suggests that older age-onset SLE is not benign. There may be an interaction between lupus and age in which, although there is less lupus nephritis in the elderly, more disease activity and damage are present.
Systemic lupus erythematosus (SLE) is a chronic, multisystemic, autoimmune disease with a broad range of clinical and laboratory manifestations. It predominantly affects young women and the incidence declines after menopause. Compared to SLE studies conducted in children and women of childbearing age, studies conducted in subjects with a later age of onset are uncommon, but there may be differences between late-onset SLE and younger-onset SLE.
Late-onset lupus has been defined in the literature by most studies as onset at age ≥ 50 years and is uncommon (found in 12%–18% of SLE)1. There is less clinical awareness of late-onset lupus, leading to a delay between onset and diagnosis2–4. Font, et al observed that the interval between disease onset and diagnosis was 5 years in the late-onset group and 3 years in the early-onset group, mainly because of an insidious onset of disease and fewer classic SLE manifestations in the older-onset group2. Mak, et al also showed that there was a longer duration of symptoms prior to diagnosis in late-onset compared to younger-onset3. Formiga, et al related the prolonged diagnosis of SLE in the elderly to more frequent insidious onset of disease (75%) compared to young patients (27%)4.
Some explanations for differences in SLE between younger and older onset are not related to SLE (comorbidity), true SLE differences in autoantibody formation, or even treatment differences. As an increasing number of people survive longer, there will be more cases of late-onset SLE and thus physicians need to become more aware of this possibility. Often, late-onset lupus has an insidious onset, presents atypically, and is masked by other conditions2.
There is controversy whether late-onset SLE has differences in disease manifestations, autoantibodies, and damage accrual compared to early-onset lupus. Studies have shown differences, but the findings were not always consistent across studies1–29. Further, although each of those studies contributes to the worldwide profile of late-onset lupus, it is not possible to generalize among contemporary and multiethnic cohorts. We examined late-onset SLE (onset after or at 50 years of age) compared to early-onset SLE (onset before 50 years of age) using the 1000 Canadian Faces of Lupus database, which is a large, multiethnic, pan-Canadian lupus registry without age restrictions for patients.
MATERIALS AND METHODS
The 1000 Canadian Faces of Lupus Registry
The 1000 Canadian Faces of Lupus is a prospective multicenter cohort study of patients with a clinical diagnosis of SLE meeting the American College of Rheumatology (ACR) criteria30. The goal of the cohort is to establish a longterm national database to research lupus in a Canadian context. Recruitment began in July 2005 and included both incident and prevalent cases presenting at the 14 participating centers across Canada. Annual study visits consisted of an interview, a physical examination, laboratory tests, autoantibodies, the Charlson Comorbidity Index34, the SLE Activity Measure 2 (SLAM-2)31, SLE Disease Activity Index 2000 (SLEDAI-2K)32, and the Systemic Lupus International Collaborating Clinics/ACR damage index (SLICC/ACR DI)33 to measure cumulative end organ damage. Patients also answered the SLE Activity Questionnaire (SLAQ), a self-administered questionnaire asking about the presence of lupus symptoms over the prior 3 months, and self-reported whether they have been diagnosed with fibromyalgia (FM).
Study population and protocol
We assessed the average age of onset in the early-onset and late-onset groups, male to female ratio, ethnic diversity, and time to diagnosis from the date of the first symptom. Date of first onset of each criterion was recorded at the initial 1000 Faces study visit for each patient, and dates are therefore cumulative throughout the course of each patient’s disease. If first disease manifestation occurred at or after the age of 50 years, the subject was considered late-onset, and if it occurred before the age of 50, the subject was entered as early-onset. Patients with pediatric lupus were excluded, but we included adult patients who had onset in childhood.
Subjects were included if they met at least 4 ACR criteria for classification of SLE. We recorded the mean number of ACR criteria in both groups and the percentage of each group that had a specific criterion (such as malar rash, discoid rash, photosensitivity, or major organ involvement including renal, hepatic, and vascular organs, and central and peripheral nervous systems). We calculated the percentage of patients in the early- versus late-onset groups who presented with clinical manifestations at their first 1000 Faces study visit including fever, nephrotic syndrome, alopecia, arthralgias, weight loss, fatigue, arthritis, sicca complex, FM, Raynaud’s phenomenon, and myositis.
Laboratory features were recorded [antinuclear antibody pattern, anticentromere, anti-double-stranded DNA (anti-dsDNA), anti-Sm antibodies, anti-Ro/SSA, antiribonucleoprotein (RNP), anti-La/SSB, etc.]. The mean Charlson Comorbidity Index score was calculated for each group and the percentage of patients with specific items was calculated in early-onset versus late-onset groups. We recorded the mean SLAM and SLEDAI scores, lupus flares (“Did this patient have any major lupus flares since last annual visit?”), disease activity level on an investigator-reported visual analog scale (VAS), unusual fatigue on a patient-reported VAS, SLAQ score, and SLICC damage score. Finally, we compared treatments (hydroxychloroquine, azathioprine, cyclophosphamide, methotrexate, mycophenolate, and prednisone) between the 2 groups.
Statistical analyses
All analyses were done using SPSS Version 15 (SPSS Inc., Chicago, IL, USA). We used chi-square and Fisher exact tests to analyze qualitative differences between younger- and older-onset SLE; t tests were used to compare means. A p value ≤ 0.05 for a 2-tailed test was considered significant. Subset analyses were done to determine whether the data were similar to the overall results in the most common ethnicity (Caucasians) and logistic regressions were done using the 4 most common ethnicities and adjusting for ethnicity to verify that the results were not confounded by race, where age at onset was the dependent variable and ethnicity was used in the regression models. Multiple comparisons were not adjusted for because we wanted to determine differences in older-onset versus younger-onset SLE (with respect to disease activity, manifestations including autoantibodies, symptoms, organ involvement, treatment, and damage).
RESULTS
The 1000 Faces of Lupus database had 1528 patients eligible for this analysis; overall, the mean current age of patients was 44.31 ± 16.43 years, of whom 89.7% were women. In 161 patients (10.5%), SLE was diagnosed at or after the age of 50 years. The overall mean disease duration was 14.4 ± 10.2 years (< 50: 15.0 ± 10.5 yrs; ≥ 50: 9.3 ± 6.1 yrs; p < 0.001). The ratio of female to male patients did not differ significantly between early- and late-onset patients with SLE (p = 0.5) but was greater in early-onset patients (Table 1, Figure 1). The Middle Eastern (3/24), Caucasian (120/880), and Jewish (4/26) ethnicities had the highest percentage of patients with late-onset lupus. Demographics of the cohort are given in Table 1. On average, for those diagnosed before age 50, it took 2.82 years from the patient’s first lupus symptom to being diagnosed with lupus, and 4.83 years for those who were diagnosed after the age of 50. The difference was significant (p = 0.006).
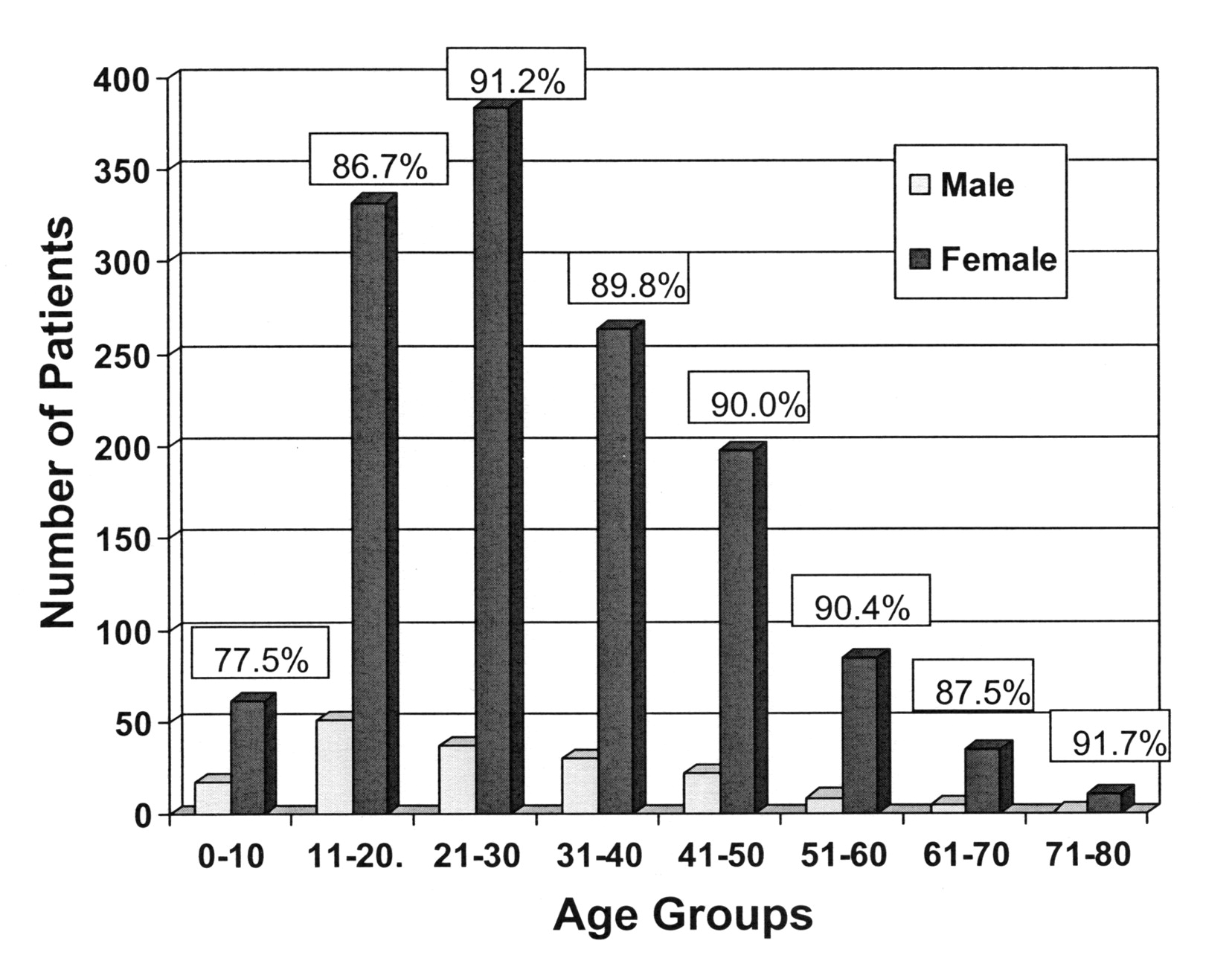
Percentage of women at different ages of SLE onset for the overall 1000 Faces of Lupus cohort. Pediatric patients were excluded from analyses in this study.
Demographics of early onset (< 50 years) vs late onset (≥ 50 years) SLE.
The mean number of ACR criteria differed significantly between patients with early- and late-onset SLE and was greater in patients diagnosed with SLE before the age of 50 years (< 50: 5.98 ± 1.68; ≥ 50: 5.24 ± 1.44; p = 0.007). The prevalence of the following ACR criteria was significantly greater in the early-onset group: malar rash (p = 0.002), renal (p < 0.0001), proteinuria (p < 0.0001), neurologic (p = 0.01), hematologic (p = 0.006), and immunologic (p = 0.006). ACR criteria that were slightly more prevalent (but did not differ significantly) in diagnosis for those at least 50 years old included discoid rash, photosensitivity, arthritis, pericarditis, cellular casts, oral and nasal ulcerations, lupus anticoagulant, false-positive VDRL, thrombocytopenia, and lymphopenia (Table 2).
American College of Rheumatology criteria in early onset (< 50 yrs) vs late onset (≥ 50 yrs) SLE.
Clinical manifestations of lupus that were significantly more prevalent at the first study visit in the group with onset age < 50 years were fever (p = 0.009) and nephrotic syndrome (p = 0.001); while alopecia was significantly more prevalent in the late-onset group (p = 0.016). FM was more prevalent in early-onset SLE, but this was not statistically significant. The following manifestations did not differ significantly but were found to be present more often in the late-onset group: arthralgias, weight loss, fatigue, inflammatory arthritis, deforming arthritis, sicca complex, Raynaud’s phenomenon, and myositis (Table 3).
Clinical manifestations of SLE (early vs late onset) at first database visit.
Examining laboratory measures, anti-RNP antibodies (p < 0.0001), anti-Smith antibodies (p < 0.0001), and low serum levels of complements (ever; p < 0.0001) were significantly more common in early-onset SLE. All other laboratory measures were nonsignificant, with anti-Scl70 antibodies, perinuclear ANCA, and cytoplasmic ANCA being slightly more prevalent in the late-onset group (Table 4).
Laboratory measures of SLE (early vs late onset).
The Charlson Comorbidity Index score was slightly worse in the older-onset SLE group (< 50: 1.25 ± 0.75, ≥ 50: 1.43 ± 1.12; p = 0.01). Categories that were significantly more prevalent in the late-onset group were congestive heart failure and peptic ulcer disease (p = 0.02 and 0.006, respectively). Moderate to severe renal disease was significantly greater in the early-onset group, however (p = 0.02). All other comorbidities were not significantly different between the early- and late-onset groups (Table 5).
Charlson Comorbidity Index.
Overall, the mean SLAM was 5.4 ± 4.0, the mean SLEDAI score 4.3 ± 4.3, and the mean SLICC score 1.5 ± 1.9. Mean disease activity (measured on a VAS) was significantly different between the early and late-onset groups and was greater in the late-onset group (< 50: 3.43 ± 2.81, ≥ 50: 4.11 ± 2.63; p = 0.04). SLAM was significantly greater in the late-onset group (< 50: 5.19 ± 3.86, ≥ 50: 7.07 ± 4.41; p < 0.0001), while there were no differences in SLEDAI (p = 0.8; Table 6). Mean lupus flares and fatigue also did not differ significantly between the 2 groups. Comparing results from the SLAQ, some conditions were all significantly more prevalent in the late-onset group: rash and nausea after sun exposure, shortness of breath, numbness and tingling in the limbs, and muscle weakness (p = 0.05, 0.02, 0.002, and 0.0008, respectively). Examining the extent of damage in the 2 groups, we found that the mean SLICC score did not differ significantly (< 50: 1.50 ± 1.94, ≥ 50:1.80 ± 1.67; p = 0.09; Table 6).
Disease activity and damage in early onset (< 50 yrs) vs late onset (≥ 50 yrs) SLE.
Assessing treatment differences, we found that generally the younger-onset group received more treatment. Current use of mycophenolate and prednisone differed: the late-onset group was receiving less of the respective drug (p = 0.001 and 0.006, respectively). All other treatment (current and ever) with hydroxychloroquine, azathioprine, cyclophosphamide, methotrexate, mycophenolate, and prednisone was similar (data not shown). Very few patients had rituximab (n = 4) and plasmapheresis (n = 9) and all were in the early-onset group.
The data were redone in the subset of Caucasians with SLE to determine whether ethnicity was actually altering the results, not age at onset (because Caucasians have less renal lupus than Asians, and Caucasians have lupus onset at an older age). The results did not differ substantially. The SLAM score was 5.4 at younger onset age and 7.0 at older onset (p = 0.002). The results were also not altered when using the data set containing the 4 most prevalent ethnicities (Caucasians, Asians, Aboriginals, Blacks) and redoing the data to adjust for ethnicity. SLAM was still significantly different and higher in older age onset SLE (p = 0.01).
DISCUSSION
Many studies have shown a decrease in female predominance in late-onset SLE3,12,20. Similarly, there was a greater ratio of women to men in the early-onset group in our study (and the percentage of female lupus patients was lowest in the prepubescent patients, looking at the overall Canadian lupus cohort; Figure 1). Disease duration was longer in the early-onset group (15 yrs in early- vs 9.3 yrs in older-onset). As found in other studies2–4, it took longer for patients with late-onset lupus to be diagnosed (from the date of their first symptom) than early-onset patients (4.83 vs 2.82 yrs).
Clinical manifestations in late-onset lupus have varied in past studies. Boddaert, et al compared 47 patients with late-onset SLE to 114 with early-onset SLE and observed a less frequent occurrence of arthritis, malar rash, and renal involvement; however, deaths occurred more frequently in the late-onset group5. Ward, et al conducted an analysis of the clinical manifestations of late-onset SLE6. This analysis showed that serositis, interstitial lung disease, and Sjögren’s syndrome were most strongly and consistently associated with late-onset SLE. Features that were less common compared to younger patients were alopecia, Raynaud’s phenomenon, fever, lymphadenopathy, hypocomplementemia, and neuropsychiatric illness.
Conversely, Bertoli, et al examined late-onset SLE in the LUMINA dataset and showed that the late-onset group was more likely to have neurological involvement, hypertension, cardiopulmonary involvement, and osteoporosis but less likely to have renal involvement, and found that late-onset lupus was an independent predictor of damage accrual7. The mean SLAM at baseline and with followup was lower in late-onset patients; however, the percentage of patients with any damage at last visit was higher in the late-onset group, especially cardiovascular and ocular damage. They concluded that late-onset lupus accrues more damage and has a higher rate of mortality. This could be biased because heart disease and eye changes (retinal and cataracts) increase in all people with age, which would increase the SLICC damage score. Maddison, et al also found that late-onset SLE had more damage at 1 and 5 years8.
In our cohort, some autoantibody differences (RNP, anti-Smith) were increased in younger patients, but otherwise differences were negligible. Laboratory results in past studies on late-onset SLE have also varied. Bertoli, et al showed a decrease in anti-Smith and anti-Ro antibodies in late-onset lupus7. Font, et al showed less anti-dsDNA and anti-Ro antibodies. Rheumatoid factor was frequently found to have a higher prevalence in late-onset SLE (but could occur due to concomitant Sjögren’s or even age)2.
Comparing causes of death, there was increased mortality in late-onset SLE, which was usually caused by cardiovascular disease or malignancies, while SLE was the cause of death for most deaths in early-onset SLE.
These results differ from other studies that have labeled late-onset lupus as more benign. Formiga, et al assessed the presentation of late-onset SLE using disease activity measured by SLEDAI and showed that compared to early-onset patients, late-onset patients had lower SLEDAI scores4. Formiga, et al related this finding of decreased disease activity to the findings of lower prevalence of high anti-dsDNA antibodies and hypocomplementemia.
Unlike the studies that have shown late-onset lupus to be more benign9–13, our data showed a slightly greater disease activity score, greater damage, and a higher Charlson Comorbidity Index score in late-onset patients. The latter is due to increased comorbidity, which should be related to increased age. All categories in the Charlson Comorbidity Index score were more prevalent in the late-onset group, including congestive heart failure, chronic obstructive pulmonary disease, and myocardial infarction; however, we also know that these are age-associated diseases. SLICC may also be increased because of comorbidity that was not related to SLE (there are some overlaps between the SLICC damage score and the Charlson Comorbidity Index). The SLAM score was significantly worse for the older patients but the SLEDAI and SLICC scores had no significant differences. This may be because these scores of disease activity ask different questions and the SLAM is more subjective, while the SLEDAI is more objective. For example, one scores fatigue (due to lupus) on the SLAM but not on SLEDAI, and the SLAM asks about anti-dsDNA, while the SLEDAI asks about complements.
Disease activity was also significantly greater in the late-onset group; however, examining which measures of disease activity were greater in the late-onset group using the SLAQ, we saw that these measures were also associated with older age (i.e., shortness of breath and muscle weakness). Perhaps treatment differences may account for some of the difference in disease activity, where older patients receive less treatment and thus have greater disease activity. There could be a reluctance to use cyclophosphamide in younger female patients because of fertility and premature menopause issues. However, the late-onset patients may have different treatment because of less severe renal involvement, generally less severe disease, and more comorbidity that could limit treatment. For most drugs (ever or current), exposure was not different between the age-onset lupus groups.
This study was cross-sectional, so there are no data on mortality. We can say that cross-sectionally in a disease with long prevalence it appears that there have been treatment differences. It is most likely that mycophenolate mofetil is used in younger women more than older women for renal lupus because of concerns about premature ovarian failure with cyclophosphamide. We can only speculate about reasons for treatment differences because the data were based on “past” and “current” criteria and treatment, and thus not collected in a way that answers some important questions.
Another limitation of the study was the potential for bias. The study was multicentered and all investigators were trained on interpretation and scoring of the SLAM, SLEDAI, and SLICC damage index. However, there was no training on global assessment and there could be a center effect causing bias in the results. This was a prevalent (in fact possibly a survival) cohort, and disease activity was collected only at current visit. But the type, number, and year of first appearance of ACR criteria were collected, as well as ever-use of immunosuppressives, so we have retrospective data on past involvement. Disease activity data were gathered by prevalent SLAM and SLEDAI, but the number of ACR criteria was determined from chart review of patients. Thus, activity is only what was seen by the definitions of the instruments (previous 10 days, previous month). However, SLICC damage and comorbidity and ACR criteria could reflect cumulative damage, but the damage could be due to pathophysiology that was not from lupus (such as aging and comorbidity, provided it occurred since onset of lupus — as per the SLICC damage index definition).
Perhaps the paradigm shift may be that in Canada, a country with universal healthcare, or for other reasons, younger onset of lupus may be less severe than in the past. It is impossible from this cross-sectional study to confirm this, but we do know that the mean age of onset in our cohort is older in Caucasians than in some other ethnicities, so the lupus could vary in severity by ethnicity as a confounder.








{kind=link}