

Abstract
Objective. This post-hoc analysis studied the effect of baseline glucocorticoid dose on the 18-month bone mineral density (BMD) response to teriparatide 20 μg/day or alendronate 10 mg/day in 387 patients with glucocorticoid-induced osteoporosis (GIO) from a randomized, double-blind trial.
Methods. Lumbar spine (LS), femoral neck (FN), and total hip (TH) BMD were measured at baseline and 18 months. Mean baseline glucocorticoid dose was categorized as low (≤ 5 mg/day), medium (> 5 and < 15 mg/day), or high (≥ 15 mg/day).
Results. Baseline LS, FN, and TH BMD were similar between groups, and between glucocorticoid dose categories within each group. LS BMD increases at the low, medium, and high glucocorticoid doses were 8.1%, 6.6%, and 4.6%, respectively, with teriparatide, and 3.6%, 2.8%, and 2.3% with alendronate. Analyzed as a continuous variable, higher glucocorticoid doses had a negative, but non-significant, effect on the percentage increase in LS BMD in both groups. Glucocorticoid dose did not significantly affect FN or TH BMD increases in either group. Across the 3 glucocorticoid dose categories, the overall LS BMD increases were different for both treatments combined (p = 0.033), but the relative differences between the treatment groups were not different (interaction, p = 0.52).
Conclusion. Teriparatide and alendronate increased LS and hip BMD across a range of baseline glucocorticoid doses. LS BMD increases with teriparatide were greater in the low-dose category than in the high-dose category. Overall LS BMD increases were significantly greater with teriparatide compared with alendronate, which may reflect the respective anabolic and antiresorptive mechanisms of action. Clinical Trial Registry Number: NCT00051558.
Glucocorticoids effectively treat inflammatory conditions but are associated with an array of side effects1, including secondary osteoporosis2. The pathophysiology of glucocorticoid-induced osteoporosis (GIO) involves multiple mechanistic pathways, including early increases in bone resorption along with decreased bone formation, and alterations in bone microarchitecture3. Daily or cumulative oral glucocorticoid doses are related to decreased bone mass and the occurrence of fractures2,4. However, patients treated with oral glucocorticoids experience fractures at a higher bone mineral density (BMD) than patients with postmenopausal osteoporosis5, and the fracture risk is greater than predicted by decreased bone mass alone6, suggesting that glucocorticoids can also negatively affect bone quality1,2,5. Other mechanisms of bone fragility, such as osteocyte apoptosis and reduced repair of local defects, may contribute to the increased fracture risk observed in patients treated with chronic glucocorticoids7.
Current guidelines for management of GIO include assessment of patients for osteoporosis risk factors prior to initiating glucocorticoid therapy, concomitant use of calcium and vitamin D supplements, and for prolonged treatment of the underlying disease, minimizing the glucocorticoid dose and/or tapering the glucocorticoid dose in low disease activity or remission2,5,8. In addition, several pharmacological therapies are currently available to offset the decreased bone density in patients taking oral glucocorticoids2,5. The bisphosphonates alendronate and risedronate are commonly used for management of patients with GIO3.
Alternatively, use of a bone anabolic agent such as parathyroid hormone (PTH), which decreases fracture risk by promoting bone formation9,10 leading to increased bone mass, is biologically reasonable since the pathophysiology of GIO mostly involves deleterious effects on osteoblasts3, resulting in decreased bone formation11. Synthetic human PTH [hPTH (1–34)] was found to increase bone mass in postmenopausal women with GIO who were also taking hormone replacement12,13. In patients with GIO treated with either teriparatide or alendronate for 18 months, patients in both groups were found to have significantly increased lumbar spine (LS) and femoral neck (FN) BMD from baseline, with significantly greater increases in the teriparatide group compared with the alendronate group14. In the same study, one patient in the teriparatide group and 10 patients in the alendronate group had incident vertebral fractures at 18 months14. Recently, teriparatide [recombinant human PTH (1–34)] was approved in Europe, Canada, and the US for treatment of osteoporosis associated with sustained systemic glucocorticoid therapy in women and men at increased risk of fracture15.
Because bisphosphonates and PTH increase BMD through different mechanisms of action, the objective of this post-hoc analysis was to examine the effects of baseline glucocorticoid dose on the changes in BMD after 18 months of treatment with either the anabolic agent, teriparatide 20 μg/day (TPTD), or the antiresorptive agent, alendronate 10 mg/day (ALN), in patients with GIO.
MATERIALS AND METHODS
Study design and population
Details of the design of this double-blind, double-dummy clinical trial (Clinical Trial Registry Number NCT00051558) conducted in 428 patients with GIO randomly assigned to TPTD (20 μg/day, Forteo™, Eli Lilly and Company, Indianapolis, IN, USA) or ALN (10 mg/day, Fosamax®, Merck & Co., Whitehouse Station, NJ, USA) were published14. This trial was a 36-month study, with a start date of November 2002 and completion date January 2008. The primary endpoint was LS BMD at 18 months.
This analysis reports 18-month data. TPTD or its corresponding placebo was self-administered by subcutaneous injection with a pre-filled pen. Encapsulated tablets of ALN or its corresponding placebo were taken orally according to the prescribed regimen16. Patients were instructed to take 1 tablet and 1 injection each day. All patients received daily supplements of calcium carbonate (1000 mg calcium) and vitamin D (800 IU).
The study was conducted in accord with the Declaration of Helsinki and the protocol was approved by the institutional review board at each study site. All patients provided written informed consent.
Patients were ≥ 21 years of age and had taken a mean dose of ≥ 5 mg/day prednisone equivalent for ≥ 3 months prior to screening. Osteoporosis was defined as a baseline spine or hip BMD T-score of ≤ −2.0, or ≤ −1.0 with 1 or more fragility fractures while taking glucocorticoids. The BMD was measured using dual-energy x-ray absorptiometry at baseline; at 3, 6, 12, and 18 months in the LS; and at 12 and 18 months in the FN and total hip (TH). Quality assurance, cross-calibration of densitometers, and data analysis were performed by a central reader, as described14. This post-hoc analysis examined the effect of baseline glucocorticoid dose on changes in BMD from baseline to 18 months in response to TPTD or ALN, and included patients with a baseline and at least 1 post-baseline BMD measurement (LS, n = 387; FN, n = 356; TH, n = 356). Baseline glucocorticoid doses were used in these analyses because glucocorticoid use data were collected at study entry. During the study, changes to the prescribed daily glucocorticoid dose and intermittent use of glucocorticoids were permitted, and changes were recorded at study visits. Additional analyses examined the effects of average dose of glucocorticoids during the study on percentage changes in LS BMD.
Statistical analyses
Analyses were conducted on randomized patients who received at least 1 dose of study medication and had a known glucocorticoid dose at baseline, using data from baseline to 18 months of therapy, or to early discontinuation (last observation carried forward). The mean percentage change in BMD from baseline to the last post-baseline measurement was determined by analysis of variance (ANOVA) and analysis of covariance (ANCOVA) with no adjustment for multiple comparisons. The model included fixed effects for the stratification terms, treatment (group), baseline glucocorticoid dose (category), and the treatment-by-dose interaction as covariates.
Because the statistical model used in this post-hoc analysis included an additional term for baseline glucocorticoid dose, these 18-month BMD results differ slightly from those previously reported14. In our analyses, glucocorticoid dose was analyzed as a categorical variable, with baseline glucocorticoid doses (mean over 30 days before randomization) defined as low (≤ 5 mg/day), medium (> 5 and < 15 mg/day), or high (≥ 15 mg/day). This categorization of glucocorticoid doses is approximate to that used in other studies4,8. When baseline glucocorticoid dose was analyzed as a continuous variable, simple linear regression analysis between LS BMD and baseline glucocorticoid dose was applied for each treatment group (TPTD or ALN) in order to study the relationship between the baseline glucocorticoid dose and BMD changes.
RESULTS
Baseline characteristics
There were no statistically significant differences in any of the baseline characteristics between the TPTD and ALN treatment groups in the overall analysis population, and within each baseline glucocorticoid dose category (Table 1). However, there were some differences in age between glucocorticoid dose categories. Irrespective of treatment group, patients who had a high glucocorticoid dose at baseline were younger than patients with a low or medium dose (p < 0.001 for each comparison). No other baseline characteristics were significantly different between the glucocorticoid dose categories.
Baseline characteristics of analysis population. All values are mean ± standard error (SE) unless otherwise indicated. Data from 387 patients with baseline and ≥ 1 post-baseline BMD measurement and baseline glucocorticoid (GC) dose data.
Increases in BMD in the overall analysis population and between treatment groups
In the overall analysis population, patients in both the TPTD and ALN treatment groups had statistically significant increases from baseline to 18 months in LS (Figure 1), FN (Figure 2), and TH BMD (Figure 3). The increase in LS BMD was 3.6% higher in the overall TPTD group, compared with the overall ALN group (p < 0.001; Figure 1, Table 2). The overall BMD increases at the FN and TH were not significantly different between treatment groups (Table 2). Patients in the low glucocorticoid dose category had greater increases in BMD at the LS (p < 0.001) with TPTD compared with ALN. In the medium glucocorticoid dose category, patients treated with TPTD had significantly greater increases in BMD at all sites than patients treated with ALN (Table 2). For patients in the high glucocorticoid dose category, the BMD changes were not significantly different between the TPTD and ALN treatment groups (Table 2). The interactions were not significantly different (Table 2), suggesting that the relative differences in BMD changes between treatment groups were similar across the 3 baseline glucocorticoid dose categories.

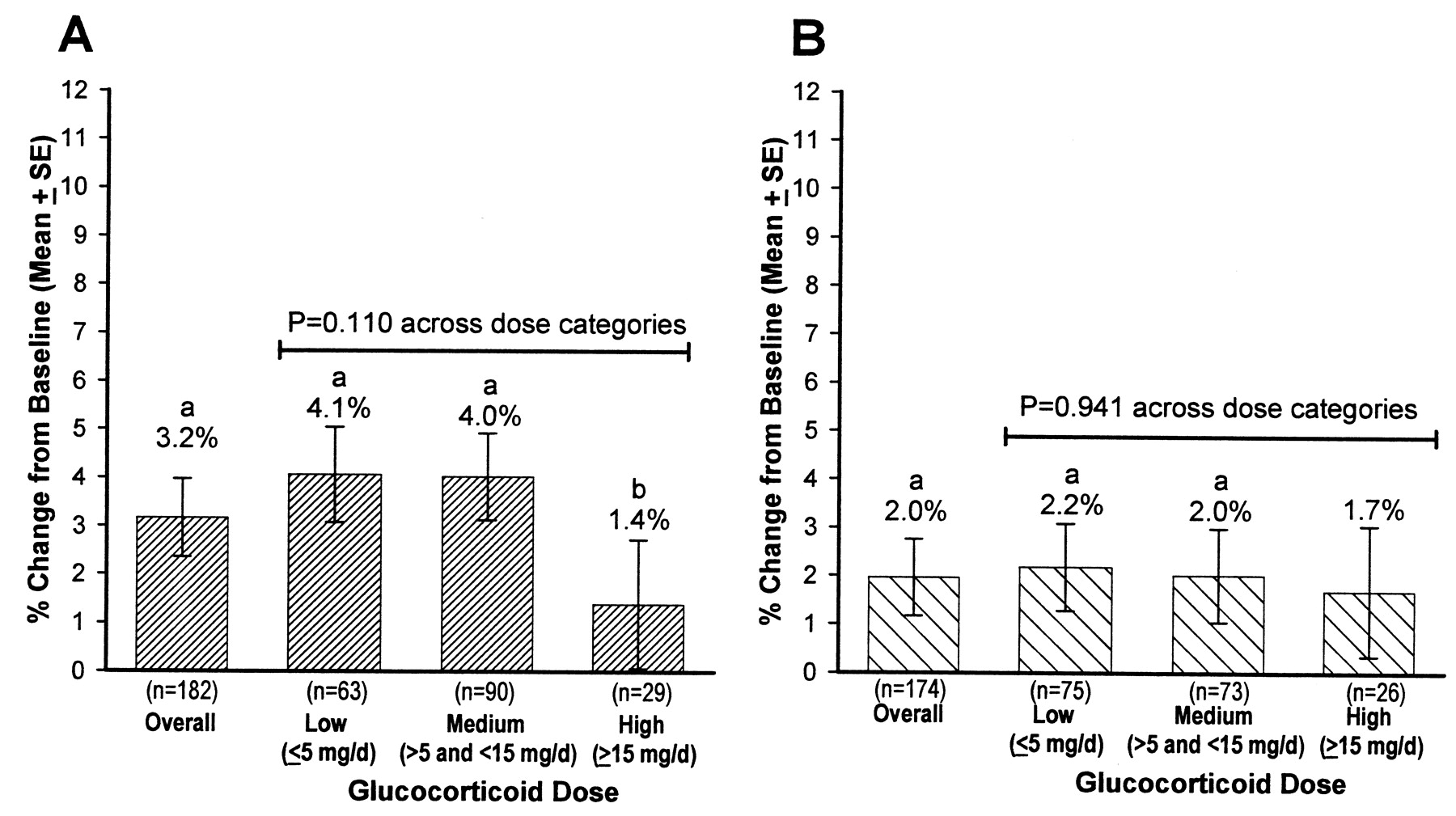
Mean percentage increases in lumbar spine bone mineral density from baseline to 18 months. A. teriparatide; B. alendronate. ap < 0.05 from baseline. bp = 0.012 between low and high dose categories.
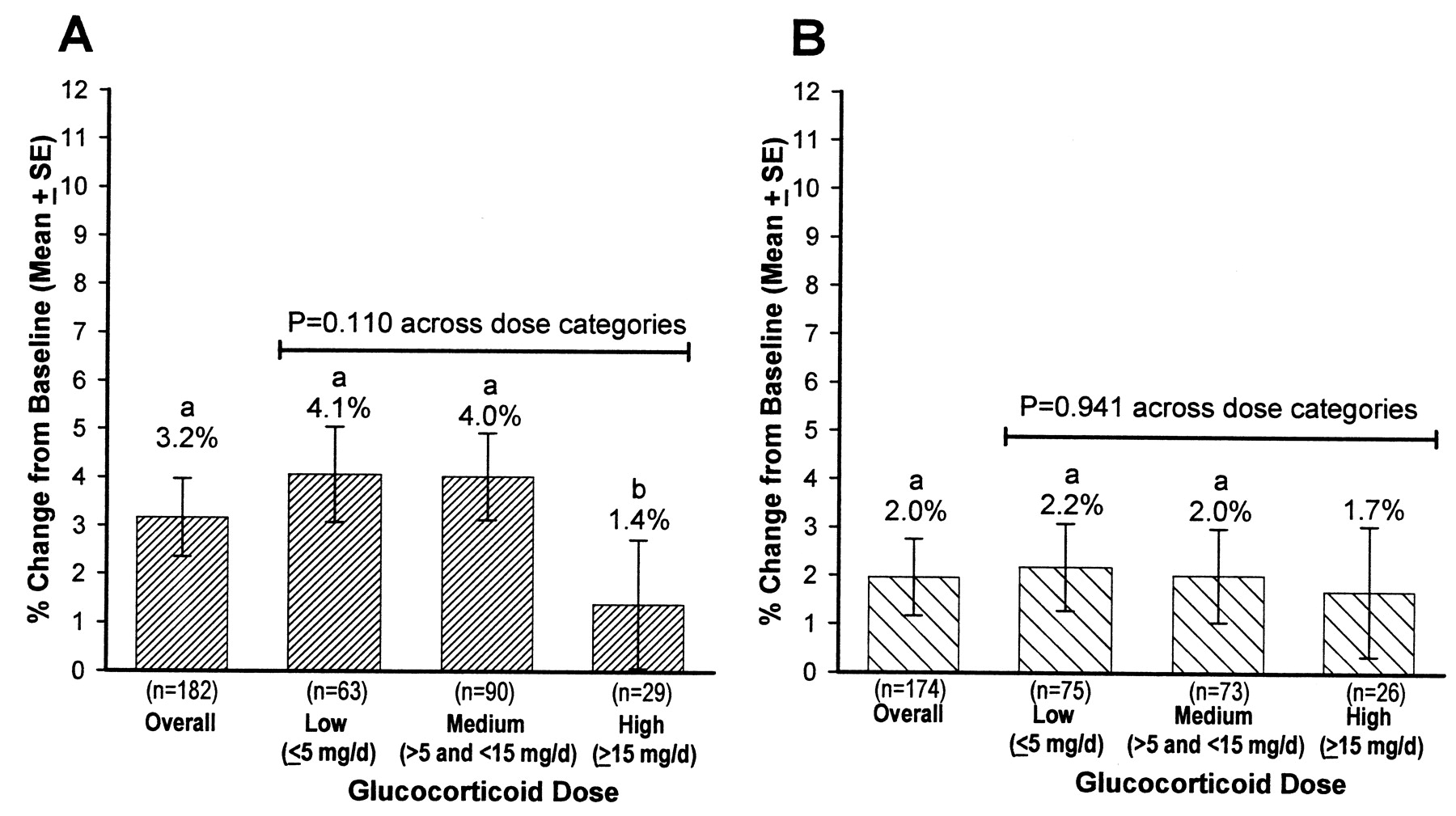
Mean percentage increases in femoral neck bone mineral density from baseline to 18 months. A. teriparatide; B. alendronate. ap < 0.05 from baseline. bp < 0.05 between medium and high dose categories.
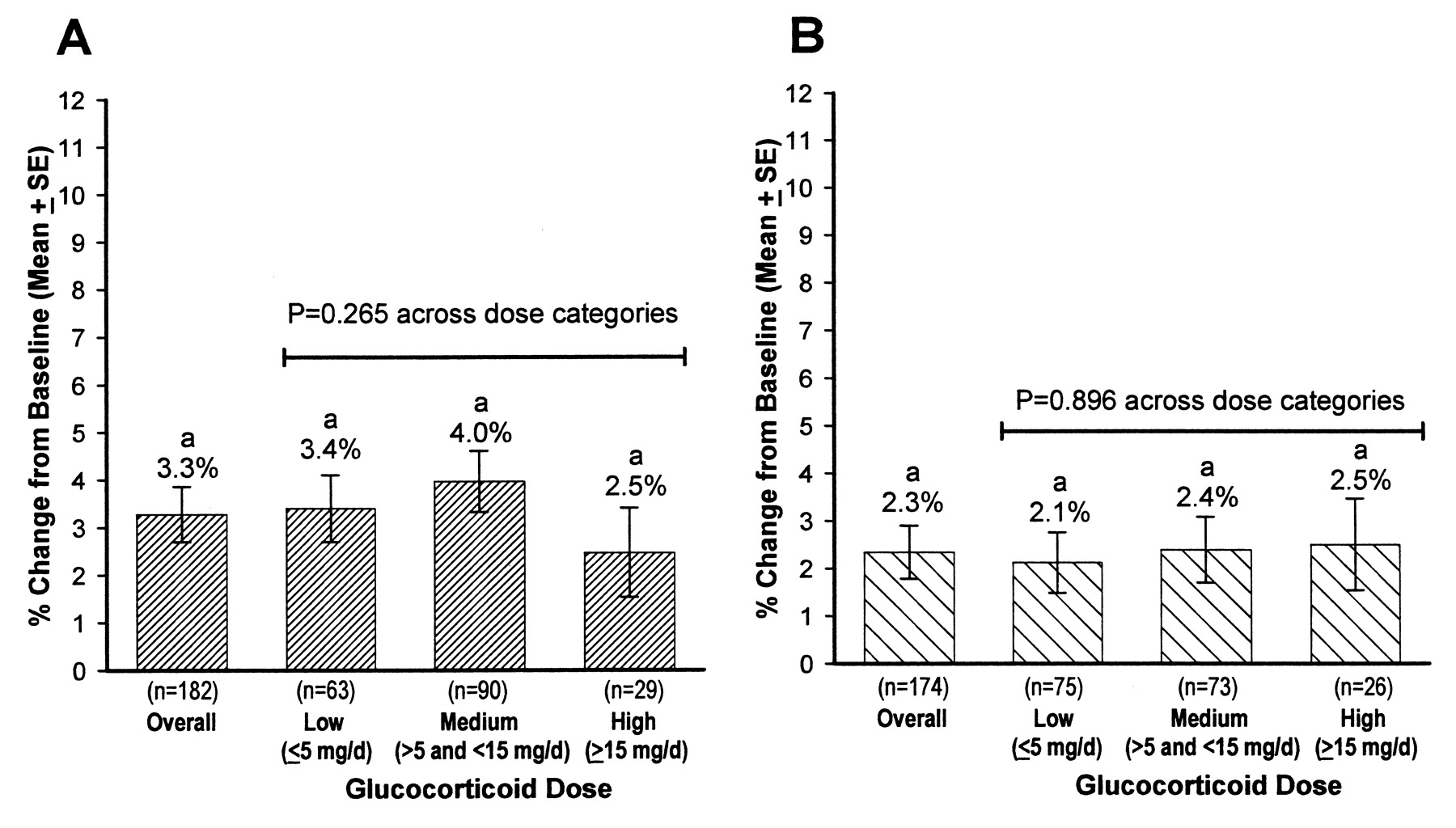
Mean percentage increases in total hip bone mineral density from baseline to 18 months. A. teriparatide; B. alendronate. ap < 0.01 from baseline.
Differences between the teriparatide (TPTD) and alendronate (ALN) treatment groups in the mean percentage increase in bone mineral density (BMD) from baseline to 18 months.
Increases in BMD with baseline glucocorticoid dose categories
LS BMD was significantly increased from baseline in all 3 glucocorticoid dose categories in the TPTD treatment group, and in the low and medium dose categories in the ALN group (Figure 1). However, the LS BMD increase with TPTD was significantly different among the glucocorticoid dose categories (p = 0.036), with the increase in BMD in the low glucocorticoid dose category being 3.5% greater than that in the high glucocorticoid dose category (p = 0.012). With ALN treatment, the BMD increases were not significantly different among the baseline glucocorticoid dose categories (p = 0.507).
FN BMD was significantly increased from baseline with TPTD and ALN treatment in patients with low or medium baseline glucocorticoid dose, but not in patients in the high dose category (Figure 2). The FN BMD increases were not significantly different among glucocorticoid dose categories in either treatment group (TPTD, p = 0.110; ALN, p = 0.941). TH BMD was significantly increased from baseline with TPTD and ALN at all baseline glucocorticoid dose categories, and these increases were not significantly different among the glucocorticoid dose categories (Figure 3). Fewer patients (< 30 in each treatment group) were in the high baseline glucocorticoid category, compared with patients with low or medium dose categories, which led to greater variability in the BMD responses, particularly at the FN.
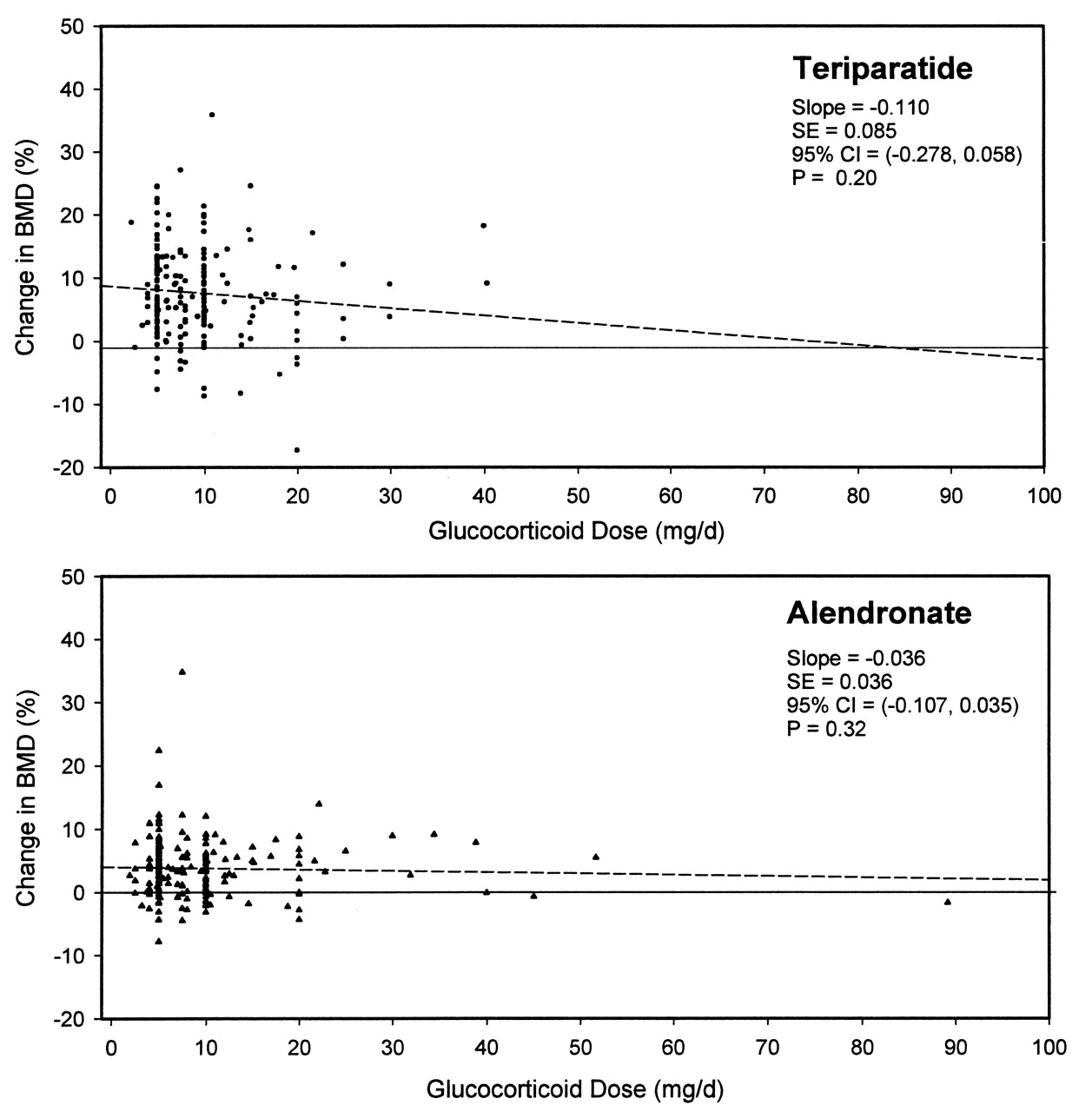
Because of the difference in the LS BMD response with TPTD across the glucocorticoid dose categories (Figure 1A), additional analyses were performed with glucocorticoid doses as a continuous variable (Figure 4). Higher glucocorticoid doses decreased the effect of both TPTD and ALN on the change in LS BMD, as indicated by the negative slopes. The slopes, however, were not statistically significant in either treatment group. In both treatment groups, most patients had baseline glucocorticoid doses between 5 and 20 mg/day, with distinct clusters of patients taking 5 and 10 mg/day doses at baseline (Figure 4).

Relationships between baseline glucocorticoid doses, analyzed as a continuous variable, and changes in lumbar spine bone mineral density (BMD) from baseline to 18-month endpoint. BMD changes were attenuated with an increasing dose, as indicated by regression lines (broken lines), although the slopes of the regression lines were not statistically significant with either treatment. Most patients took 5 or 10 mg/day glucocorticoid doses at baseline, as shown by the distinct clusters.
Similar regression analyses were performed using average glucocorticoid dose during the study as a continuous variable. The estimated slopes of the curves for percentage changes in LS BMD as a function of average glucocorticoid dose were −0.078 (95% CI −0.179, 0.023, p = 0.13) in the ALN treatment group, and −0.174 (95% CI −0.356, 0.008, p = 0.06) in the TPTD treatment group.
DISCUSSION
Patients with low and medium baseline glucocorticoid doses, treated with either TPTD or ALN, had significant increases from baseline in LS, FN, and TH BMD at 18 months. Increases in LS BMD were significantly greater in the TPTD group compared with the ALN group in the overall analysis population, and in patients in the low and medium baseline glucocorticoid dose categories. With TPTD treatment, increases in LS BMD were significantly smaller in patients in the high baseline glucocorticoid dose category compared with patients in the low glucocorticoid dose category, but this relationship was not seen with ALN treatment. However, there was no significant relationship between changes in LS BMD and baseline glucocorticoid dose, when analyzed as a continuous variable.
In the primary clinical trial analysis, the TPTD group had significantly higher BMD increases than the ALN group at all measurement sites14. However, in the present overall analysis population, increases in FN and TH BMD were not significantly different between the TPTD and ALN groups. This result may be attributed to the additional term used in the statistical model for the 3 baseline glucocorticoid dose categories in our analysis. Increases in FN and TH BMD with either TPTD or ALN therapy were not significantly diminished with increasing baseline glucocorticoid doses, and may reflect the lower level of bone turnover at these sites, which are predominantly cortical bone. In a trial of 28 postmenopausal women with GIO treated with synthetic PTH (1–34) along with estrogen, LS BMD was significantly increased by 11% from baseline to 12 months, while the 2.9% and 1.9% increases in FN and TH BMD, respectively, were not statistically significant12. In a 12-month followup after discontinuation of synthetic PTH (1–34) and with continuation of estrogen, LS BMD remained significantly increased from baseline by 12.6% at 24 months, while FN and TH BMD further increased to 5.2% and 4.7% from baseline, respectively13, suggesting that the maximal anabolic effects of PTH at the hip in the presence of estrogen may be reached at a later timepoint.
The BMD increases of the ALN-treated patients in the clinical trial14 are consistent with those observed in other GIO trials with antiresorptive therapies. In patients treated with ALN 10 mg/day, LS BMD increased from baseline by 2.9% at 1 year17, and by 3.9% at 2 years18, while FN BMD was maintained at both timepoints. Glucocorticoid dose and LS BMD at baseline did not affect the LS BMD increases with ALN17. Another bisphosphonate, risedronate 5 mg/day, prevented BMD loss in patients initiating glucocorticoid therapy19,20, and increased BMD in patients taking longterm (≥ 6 months) glucocorticoid therapy, as well as decreasing the vertebral fracture risk compared with placebo21,22. For both ALN23 and risedronate20, patients who continued glucocorticoid therapy but discontinued the bisphosphonate experienced bone loss, while BMD was maintained in patients who took concomitant bisphosphonate therapy.
The pathophysiologic processes of GIO2,3,5,11, relative to the respective mechanisms of action of TPTD and ALN, may partly explain the observed differences in BMD changes. As recently summarized3, the adverse skeletal effects of glucocorticoids primarily result from direct actions on bone cells, with indirect effects on synthesis and actions of bone-active cytokines and sex hormones, and to a lesser degree, alterations in calcium and vitamin D metabolism. A primary effect of glucocorticoids is to directly inhibit differentiation of new osteoblasts and promote apoptosis of existing osteoblasts, resulting in decreased bone formation3,5. Glucocorticoids also directly promote osteoclast formation, activity, and survival, which in turn increases bone resorption and leads to the rapid bone loss seen early in therapy3,5. The adverse effects of glucocorticoids on osteocyte function and increasing osteocyte apoptosis may lead to enhanced bone fragility independently of decreased bone mass3,11. For example, glucocorticoid-treated mice have localized demineralization around osteocytes, which may be associated with decreased biomechanical strength24. Osteocytes also act as mechanosensors to target local regions of bone formation and resorption, which in turn contribute to bone microarchitecture stability7,10. Disruption of osteocyte function by glucocorticoids may exacerbate fracture risk independently from loss of BMD alone5,11. Glucocorticoids have indirect adverse effects on bone-active cytokines, such as insulin-like growth factor, and on testosterone and estradiol, which are involved in maintaining bone health, and therefore, may contribute to bone fragility in a secondary manner2. Alterations in calcium and PTH metabolism with glucocorticoids play minor roles in the pathogenesis of GIO3. Although glucocorticoid use results in a negative calcium balance, which may lead to secondary hyperparathyroidism, intact PTH levels were not elevated in patients taking oral glucocorticoids2,5,25. Finally, chronic oral glucocorticoid use may also indirectly contribute to loss of bone and muscle mass26, which may increase the risks of falling and fractures1,5.
Studies have suggested that currently available osteoporosis therapies increase BMD in patients with GIO by opposing or reversing some of the same mechanisms by which oral glucocorticoids exert deleterious effects on bone5,7. Bisphosphonates, such as ALN, bind to bone mineral and inhibit osteoclast activity, to decrease bone resorption and fracture risk27. In contrast, bone anabolic agents such as PTH decrease fracture risk by increasing new bone formation through increasing osteoblast number and maturation of osteoblast precursors, and prolonging the lifespan of osteoblasts and osteocytes in preclinical models9,10,28. Therefore, it is biologically reasonable to use PTH to offset the direct actions of glucocorticoids on osteoblasts and osteocytes, the primary contributors to GIO3,10. Relative to lower doses, higher doses of glucocorticoids were found to blunt the LS BMD response to TPTD, which may be due to the primary opposing actions of TPTD and glucocorticoids directly on osteoblasts. The consistent BMD increases with ALN treatment at higher glucocorticoid doses may not directly reflect a greater bone mass, since prolonged secondary mineralization of bone matrix, which is not affected by glucocorticoids, also contributes to the BMD increases with ALN29. In patients treated with ALN, changes in LS BMD were similar between the baseline glucocorticoid doses, suggesting that higher glucocorticoid doses may have less influence on the osteoclast inhibitory effects of ALN, even though early bone loss with glucocorticoids is due to increased osteoclast activity2. Further studies on the interactions between osteoporosis therapies and glucocorticoid doses on bone turnover may help determine the underlying mechanisms for the observed BMD effects with these therapies in patients taking various glucocorticoid doses.
Strengths of this study include having data from a double-blind, randomized, comparator-controlled clinical trial, and performing categorical and continuous analyses of baseline glucocorticoid doses. Further, the glucocorticoid dose categories were clinically relevant, as supported by the observed clustering of patients at 5 and 10 mg/day doses in this study, and by similar categories defined in other studies4,8. However, these analyses were limited by using only the baseline glucocorticoid dose, defined as the average dose taken immediately after screening but before randomization for the study, which may underestimate the actual extent of glucocorticoid exposure, as patients had an average 5 years of glucocorticoid treatment prior to study entry. Changes in the prescribed daily glucocorticoid dose during the study were recorded only at study visits and intermittent use of glucocorticoids was not quantified. Finally, the small numbers of patients in the high glucocorticoid dose category resulted in a greater variation of BMD values, and may in part explain the lack of statistical significance in the BMD increases from baseline to the endpoint, and the differences in BMD between treatment groups. Patients in the high glucocorticoid dose category were also significantly younger and possibly had more severe underlying disease or different diseases than those in the low or medium dose categories.
In summary, both TPTD and ALN treatment increased BMD at the LS and hip sites across a range of baseline glucocorticoid doses. The increases in LS BMD were significantly greater with TPTD, an anabolic agent, compared with ALN, an antiresorptive agent, in the overall analysis population, and in patients in the low and medium glucocorticoid dose categories. The increase in LS BMD with TPTD, but not with ALN, was affected by the baseline glucocorticoid doses, which may reflect the different mechanisms of action of these agents.
Acknowledgments
The authors thank Yiwei Liu, MS, MD, of MedFocus, for assistance in statistical programming, and Susan Zeilinga, of Lilly Research Laboratories, for manuscript formatting and editing.
Footnotes
-
Lilly USA, LLC, sponsored this clinical trial.
- Accepted for publication August 7, 2009.








{kind=link}
{kind=link}
{kind=link}
{kind=link}