

Abstract
Objective. To determine the prevalence of anti-RNA polymerase III autoantibodies in French patients with systemic sclerosis (SSc) and to identify the associated clinical manifestations.
Methods. Consecutive patients with SSc seen in 3 tertiary centers in Paris were included. Sera samples were collected together with the relevant clinical and immunological data. Anti-RNA polymerase III antibodies were detected by ELISA at a central laboratory. Data on other antibodies were abstracted from the medical records.
Results. We included 319 patients: 84% women, 36% with a diffuse cutaneous subtype, 44% with pulmonary fibrosis, 5% with pulmonary hypertension, 4% with renal crisis, among whom 29 (9.4%) had anti-RNA polymerase III antibodies. These antibodies were more prevalent in patients with diffuse than with limited cutaneous disease (14.3% vs 6.0%; OR 2.6, 95% CI 1.2–5.48, p = 0.016). Renal crisis was more prevalent in patients with than in those without anti-RNA polymerase III antibodies (14% vs 3%; OR 5.0, 95% CI 1.4–17.3, p = 0.012). Renal crisis occurred in 2.2% of patients with anti-topoisomerase I and 3.9% of patients with anticentromere antibodies. Of the patients with anti-RNA polymerase III antibodies, 24 (83%) had no other systemic sclerosis-specific autoantibodies.
Conclusion. The prevalence of anti-RNA polymerase III antibodies in French patients appeared to be lower than in the United States and similar to that in continental Europe. These antibodies were consistently associated with diffuse cutaneous disease and were the most common immunological marker for renal crisis. Anti-RNA polymerase III determination can help to risk-stratify SSc patients at high risk for this severe manifestation.
Systemic sclerosis (SSc) is a chronic connective tissue disease of unknown origin characterized by microvascular alterations, immunological disturbances, and deposits of collagen and other matrix substances within the connective tissue.
Although the mechanisms underlying these abnormalities remain unclear, immunological disturbances may play a key pathogenic role. Various antinuclear autoantibodies (ANA) are found in the serum of patients with SSc. The specificity of these autoantibodies is associated with the disease phenotype. Thus, anticentromere antibodies (ACA) are usually found in patients with limited cutaneous disease1 and anti-topoisomerase (Scl-70) antibodies in patients with diffuse cutaneous disease in association with fibrosing alveolitis and heart involvement1. Other specific ANA such as anti-U1-RNP, anti-RNA polymerase III (anti-RNA pol III), anti-U3-RNP (fibrillarin)2, anti-Th/To3, anti-Ku, and anti-PmScl4 are less common.
Anti-RNA pol III are usually found in patients with diffuse cutaneous disease and correlate strongly with renal crisis, a condition of malignant hypertension and rapidly progressive ischemic renal failure mainly described in North American cohorts5. Renal crisis occurred in 10% of patients with SSc in British and US cohorts overall and in 25% of patients with diffuse cutaneous involvement6. However, lower rates were reported in Mediterranean countries, where the prevalence of anti-RNA pol III was also very low7–9. This brings into question the usefulness of such an autoantibody in these populations.
In a previous study, we observed a striking difference in overall SSc-related serum autoantibody between French and American patients with SSc, but the scarcity of anti-RNA pol III and the limited sample size did not allow strong conclusions regarding this specific autoantibody in the French population of patients with SSc9. The aims of the present study were to determine the prevalence of anti-RNA pol III in a large population of patients with SSc in France and to assess associations between anti-RNA pol III and the disease phenotype.
MATERIALS AND METHODS
Patients
We included 319 patients with SSc managed at 3 tertiary centers in Paris, France: 116 from Bichat Hospital, 153 from Cochin Hospital, and 50 from St. Antoine Hospital.
Disease duration was defined as the first symptom other than Raynaud’s phenomenon, and the variables used to reflect systemic involvement as described9.
Definition of clinical findings
SSc clinical features were considered to be present if predefined criteria were met during the course of the illness and were not attributable to other diseases. All centers adhered strictly to these criteria for cross-sectional patient evaluation.
A global evaluation of these patients was carried out. Age, sex, disease duration (first non-Raynaud’s symptom), and cutaneous SSc subtype were collected. Patients were classified into disease subsets based on the maximum extent of skin thickness at any time during the course of the disease. Patients with diffuse cutaneous involvement must have had skin thickening proximal to the elbows or knees (affecting upper arms, thighs, or trunk) at some time during their illness. In contrast, individuals with limited cutaneous involvement either had no skin thickening (SSc sine scleroderma) or skin thickening distal only to the elbows and knees throughout their course. Facial skin thickening was permitted in patients classified as limited cutaneous SSc.
Patients underwent pulmonary function tests including forced vital capacity (FVC) and diffusion capacity for carbon monoxide (DLCO). Chest high-resolution computed tomography (HRCT) was used as recommended to measure SSc-associated interstitial lung disease (SSc-ILD). An echocardiography was performed: left ventricular dimension was recorded, systolic function was assessed by Simpson’s method, diastolic dysfunction was assessed by pulsed tissue Doppler imaging (lateral annulus early diastolic velocity < 10 cm/second was considered as abnormal) and systolic pulmonary artery pressure (sPAP) was approximated by continuous-wave Doppler measurement of the trans-tricuspid or trans-pulmonary pressure gradient, after the addition of an estimated 10 mm Hg right atrial pressure.
When sPAP at rest on Doppler echocardiography exceeded 40 mm Hg, right-heart catheterization was performed; pulmonary arterial hypertension (PAH) was confirmed for mean PAP > 25 mm Hg and was considered as SSc-associated precapillary PAH when associated with a pulmonary artery wedge pressure below 15 mm Hg10. The presence of active or healed digital ulcers, the previous use of prostacyclin, and the presence of acroosteolysis and calcinosis on hand and wrist radiographs were considered.
Patients with dyspnea (New York Heart Association Grade II and higher) often showed isolated impairments of carbon monoxide transfer factor, with < 75% of the predictive values with forced vital capacity < 80%.
Pulmonary interstitial fibrosis was defined as SSc-associated, when other possible causes of lung fibrosis were excluded and bilateral fibrosis was confirmed by chest radiograph, HRCT scan, and/or restrictive pulmonary abnormalities on pulmonary function tests (total lung capacity < 80%).
Renal crisis was defined as the abrupt onset of accelerated arterial hypertension or rapidly progressive oliguric renal failure11.
All patients gave informed consent for all procedures, which were carried out with local ethics committee approval. The study was conducted in accord with the recommendations of the Helsinki Declaration and all investigations were those routinely required to evaluate the patients.
Autoantibodies
Stored (−20°C) serum samples were used for autoantibody determinations. Anti-RNA pol III were assayed in all 319 serum samples during the same run, using an enzyme-linked immunosorbent assay (ELISA) with recombinant protein based on a human RPC155 immunodominant subunit of anti-RNA pol III, according to the manufacturer’s recommendations (MBL, Clinisciences, Montrouge, France). Briefly, diluted sera were incubated for 60 min on the coated plate, which was then washed before the addition of horseradish peroxidase-conjugated goat anti-human IgG for 60 min. The reaction was revealed by addition of TMB (3.3’.5’-tetramethylbenzidine dihydrochloride) and color intensity was measured at 450/620 nm. Results were expressed as units/ml (U/ml) and values ≥ 28 U/ml were considered positive, according to the manufacturer’s instructions.
Anti-RNA pol III were assayed with another ELISA (Quantalite RNA PIII Elisa, Inova, San Diego, CA, USA) with a recombinant peptide of anti-RNA pol III. The cutoff was 20 U/ml, according to the manufacturer’s instructions. Other ANA specificities including anti-topoisomerase I and anti-U1-RNP were evaluated using local commercial ELISA. ACA were identified from the ANA pattern by indirect immunofluorescence on HEp-2 cells with an initial serum dilution of 1:80 (Kallestadt, Bio-Rad Laboratories, Redmond, WA, USA). All ELISA analyses were conducted using blinded data. Some data from local analysis and clinical manifestations are missing, and for 6 patients, classification between limited and diffuse scleroderma was not reported in the computed data.
Statistical analysis
Statistical analysis involved use of SAS release 9.1 (SAS Institute, Cary, NC, USA). Continuous values are reported as mean ± standard deviation. Categorical variables are reported as absolute number or percentage. We identified the factors associated with anti-RNA pol III by both univariate and multivariate analysis (logistic regression model). Factors included in the multivariate model were clinical issues [i.e., cutaneous SSc subtype (diffuse or limited), PAH, renal crisis and pulmonary fibrosis]. Interactions between these factors were not significant. p < 0.05 was considered statistically significant.
RESULTS
Demographic features
Of the 319 patients, 84% were women. Disease duration (mean ± SD) was 11.4 ± 9.3 years. About two-thirds of the patients had limited cutaneous involvement (201/313, 64%) and one-third diffuse cutaneous involvement (112/313, 36%). Main organ involvement according to the definitions above were pulmonary fibrosis in 131/298 (44%) patients, pulmonary hypertension in 14/289 (5%), and renal crisis in 13/318 (4.1%; Table 1).
Demographic features in the French systemic sclerosis cohort (n = 319).
SSc-related ANA
ACA were found in 76/313 (24.3%) patients, anti-topoisomerase I in 91/312 (29.2%), anti-U1-RNP in 21/217 (9.7%). Regarding anti-RNA pol III, antibodies could be detected in 29/319 (9.1%) with the MBL ELISA test. Among the 29 patients with anti-RNA pol III, 5 (17%) had another SSc-related ANA (ACA, n = 1; anti-topoisomerase I, n = 2; or anti-U1-RNP, n = 2).
In order to validate the MBL ELISA anti-RNA pol III test, 97 sera from the entire cohort were tested using a protein immunoprecipitation test (IP) as described9. Five sera were positive using IP and all were strongly positive by the ELISA test (from 85 to 205 U/ml); 4 sera from patients with limited SSc were ELISA-positive (29 to 44 U/ml), but were not positive using the IP technique. Other associated specificities were detected for these 4 sera: 1 patient with overlap disease (mixed connective tissue disease) had anti-U1-RNP, 1 with overlap had Sjögren-SSc SSA, and 2 with limited SSc had anti-topo-I isomerase. No sera positive with the IP test for anti-RNA pol III were negative using the MBL ELISA test. The concordance rate was 93/97 (96%) between the 2 methods.
A comparison was done between our ELISA anti-RNA pol III test and another commercial ELISA test (Inova)12 in order to test the validity of our data. The 29 sera from various patients with a positive MBL anti-RNA pol III ELISA were compared with the second kit: 27/29 gave a positive result (93%). Conversely, the 290 sera that were negative using our MBL ELISA were tested with the Inova ELISA kit: 4/290 gave a positive signal (1.4%). The concordance rate between the 2 ELISA tests was 309/319 (96.8%).
Features of patients with SSc with anti-RNA polymerase III antibodies
Patients with anti-RNA pol III (n = 29) did not differ from the remaining patients regarding the sex ratio (women, 90% vs 84%) or mean disease duration (13.8 ± 12.8 vs 11.2 ± 8.9 years). Two features were significantly more common in the group with anti-RNA pol III than in the group without anti-RNA pol III: diffuse cutaneous involvement (57% vs 34%, respectively; OR 2.6, 95% CI 1.2–5.48, p = 0.016) and renal crisis (14% vs 3%; OR 5.0, 95% CI 1.4–17.3, p = 0.012). Positive predictive value of anti-RNA pol III for renal crisis was 13.8% and negative predictive value was 96.9%. No significant differences were found for pulmonary fibrosis (39% vs 44%) or pulmonary hypertension (3.7% vs 5%; Table 2). ACA and anti-topoisomerase I antibodies were significantly less prevalent in patients with than in patients without anti-RNA pol III. No difference was seen for anti-U1-RNP antibodies. Multivariate analysis confirmed an independent association of the diffuse cutaneous type of SSc and the scleroderma renal crisis with antibodies to anti-RNA pol III (Table 3). Among patients with anti-RNA pol III, serum concentrations of the antibody did not differ between patients with limited and those with diffuse cutaneous involvement (Figure 1). No difference was seen between patients with or without renal crisis for median levels of anti-RNA pol III: 116 U/ml vs 88 U/ml, respectively (25th–75th interquartile range: 69.75–165 U/ml vs 46–143 U/ml).
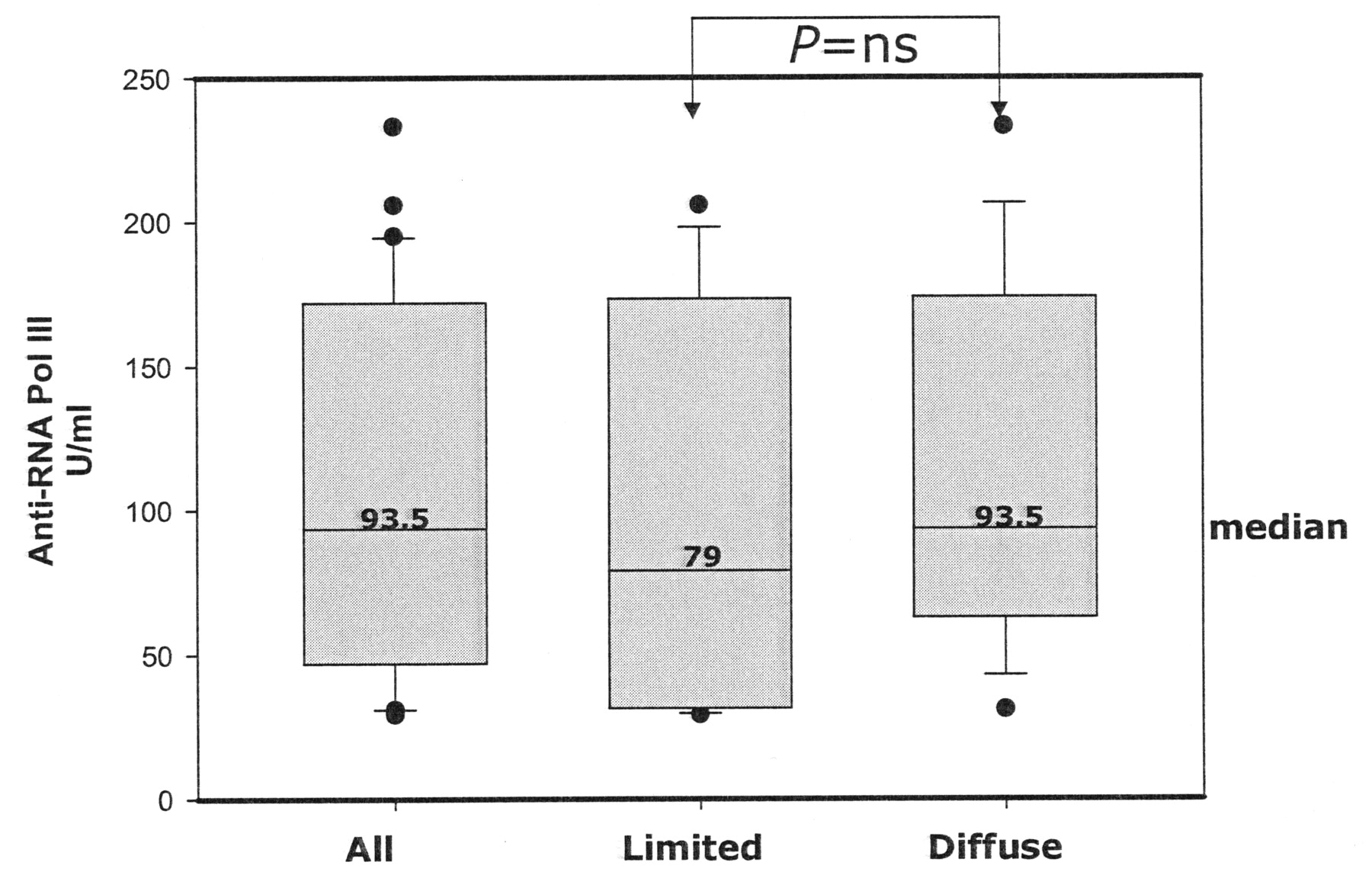
Median (IQR 25–75) anti-RNA polymerase III antibody levels in patients with limited (n = 13) or diffuse (n = 16) cutaneous systemic sclerosis (only positive sera were plotted). ns: not significant.
Clinical and laboratory characteristics of 319 patients with SSc, indicating the presence or absence of anti-RNA polymerase III antibodies (univariate analysis).
Clinical characteristics associated with anti-RNA pol III antibodies (multivariate analysis).
DISCUSSION
In our patients with SSc recruited at tertiary centers with extensive experience in diagnosing and treating this disease, the prevalence of anti-RNA pol III was 9.4% overall and it was significantly higher in the subgroup with diffuse cutaneous involvement and in patients who had already developed renal crisis.
The prevalence of anti-RNA pol III among patients with SSc differed between Europe and North America in earlier studies1,12. In a subgroup of the present cohort recruited at a single center, the prevalence was 4%, compared to 25% in a cohort from Pittsburgh, USA9. In Europe there seems to be a decreasing north to south gradient, with prevalences of 22% in Sweden13, 12% in England14, and 8% in Italy8; however, the prevalence was only 5% in Poland9. The 9.4% prevalence in our multicenter study from Paris, France, is consistent with such a gradient. Low anti-RNA pol III prevalences were found in Japan (6%)15,16 and South Korea (3.4%)17. Among patients with SSc in Texas, USA, the prevalence of anti-RNA pol III was higher among Hispanics and African Americans than among Caucasians18. Caucasians contributed more than 98% of the patients in our study and in the studies from Sweden13, Poland, and Italy8. Thus, among patients with SSc, the prevalence of anti-RNA pol III in Caucasian residents of Europe may decrease slightly from north to south and may be lower than in US residents. Different techniques were used to detect anti-RNA pol III in the above studies and could explain part of the variability across countries. The results with the ELISA kit used at our laboratory correlate well with those of the IP test, which is considered to be the reference technique16. As ELISA is a quantitative test, we were able to compare the median levels of anti-RNA pol III in diffuse and limited cutaneous subgroups, and we found no difference. The median level of anti-RNA pol III did not differ among positive patients with or without renal crisis. Among the 29 patients with anti-RNA pol III, the proportion with diffuse scleroderma (57%) was quite low compared to North American studies, where 86%–90% of patients with this antibody have diffuse cutaneous SSc16. This discrepancy can be attributed to the detection method to characterize the anti-RNA pol III isomerase antibody since some borderline-positive sera were considered negative with the gold standard method (protein immunoprecipitation test) and the other ELISA method. The 4 discordant sera were all from patients with limited-type SSc. However, Harvey, et al19 reported 43% of diffuse cutaneous SSc among patients with anti-RNA pol I + II antibodies determined by a radio-immunoprecipitation technique. A 67% prevalence was reported by Bardoni, et al8 and 59.5% by Santiago, et al in Canadian patients12.
SSc-specific ANA are widely believed to be mutually exclusive. In our study, data on both ACA and anti-topoisomerase I antibodies were available for 312 patients, none of whom had both antibodies in combination. Similarly, the anti-U1-RNP status was known for 217 patients, none of whom had more than 1 SSc-specific ANA. However, 5 (17%) of the 29 patients with anti-RNA pol III also had another SSc-specific ANA. Therefore, a positive test for ACA or anti-topoisomerase I antibodies does not rule out the presence of anti-RNA pol III. This point is important since anti-RNA pol III is associated with severe clinical manifestations.
Anti-RNA pol III were associated with diffuse cutaneous involvement in our population, in keeping with earlier studies. Thus, in the United States, anti-RNA pol III were present in 45% of patients with diffuse disease compared to only 6% of those with limited disease5 in one study, and in 22% and 2%, respectively, in another20.
Pulmonary fibrosis, PAH, and renal crisis are associated with high morbidity and mortality rates in patients with SSc. We found no association between anti-RNA pol III and either pulmonary fibrosis or PAH. The prevalence of PAH was low (5%), but reflected SSc patients with “real” precapillary PAH, defined by right-heart catheterization as recommended. Anti-RNA pol III were significantly associated with renal crisis, with an OR of 4.8 (95% CI 1.4–16.5). Renal crisis occurred in 13 (4%) patients overall and in 4 (14%) of the 29 patients with anti-RNA pol III. The 9 patients with renal crisis and no anti-RNA pol III had either ACA (n = 3) or anti-topoisomerase I (n = 2) or no detectable (n = 4) antibodies. Anti-RNA pol III antibodies had a better positive predictive value for renal crisis than anti-topoisomerase I antibodies (13.3% vs 2%) in this cohort. The high prevalence of anti-RNA pol III among patients with renal crisis is in accord with most of the previous studies9,21–23. The prevalence of renal crisis among patients with anti-RNA pol III has varied from 015 to 43%1,5,13,19,24, with a mean of 21%. The prevalence in our study was only 14%, perhaps reflecting the potential efficacy of prevention with angiotensin-converting enzyme inhibitors, although this remains a matter of debate, and avoidance of high-dose corticosteroids25.
Anti-topoisomerase I antibodies were found in 65% of 46 patients with SSc with renal crisis residing in Italy23 compared to only 17% of 110 patients in the United Kingdom22 and 6% in the United States9. The 2 studies of renal crisis among SSc patients with ACA or anti-U1-RNP antibodies produced discordant results: the prevalence was only 1% in the United States11 and 25% in the United Kingdom19 among patients with ACA; corresponding figures were 7% and 12% among patients with anti-U1-RNP antibodies. These differences may explain variations in clinical features reported from different geographic regions26.
Anti-RNA pol III are the most common, but not the only, ANA associated with renal crisis among patients with SSc. Although French and European patients with SSc appear to have weak frequencies, we assume that ELISA determination of RNA pol III is a reliable test that can help to identify patients with SSc at high risk for this severe manifestation. This simple test can be substituted for the more sophisticated protein immunoprecipitation test, which remains the gold standard. Special care should be taken for early detection of renal crisis among French patients with ELISA-positive anti-RNA polymerase III antibodies.
Footnotes
-
Supported by grants from ARDIR (Association pour la Recherche et le Développement de l’Immuno-Rhumatologie).
- Accepted for publication July 15, 2009.








{kind=link}