

To the Editor:
An 11-year-old boy presented with a restriction of rotation of the forearm. He did not complain of any pain, and there was no swelling, redness, or tenderness on local examination. His family history was insignificant and he could not recall any history of injury. Pronation of the forearm was restricted to 60 degrees and supination to 20 degrees. Flexion and extension of the elbow along with the motion of the wrist was not restricted. The results of the remainder of the clinical examination were unremarkable.
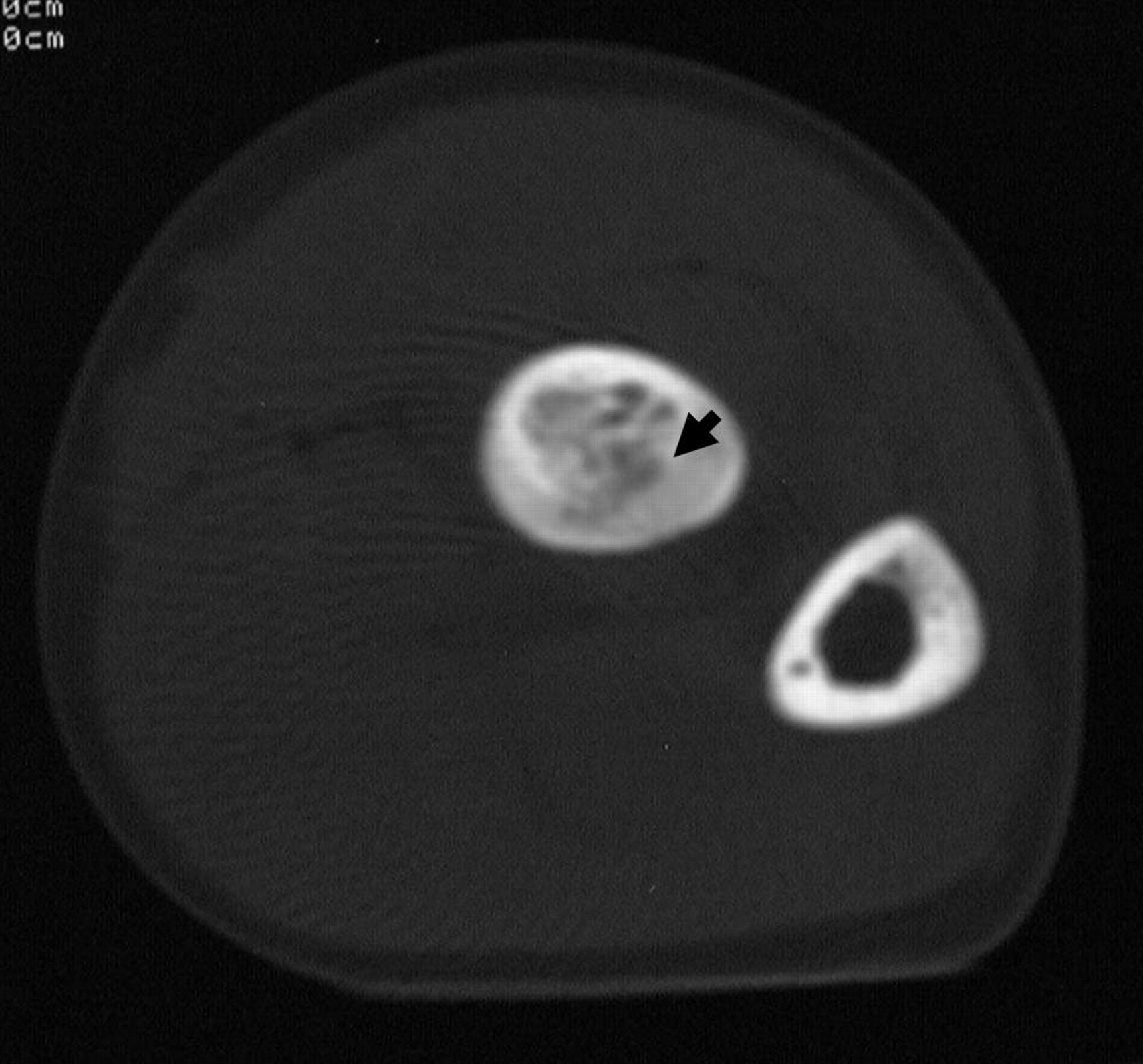
Although plain radiography was insignificant, clinical symptoms suggested an intraarticular lesion. Since lesions of the elbow often go unrecognized, further imaging studies were performed. Computer tomography (CT) scan showed a lucent area surrounded by a sclerotic rim in the proximal diaphysis of the radius (Figure 1). The position of the lesion was intramedullar. T2 weighted image depicted a small intermediate intensity area surrounded by a low intensity ring on magnetic resonance imaging (MRI). The lesion showed low intensity on T1 weighted image (Figure 2).
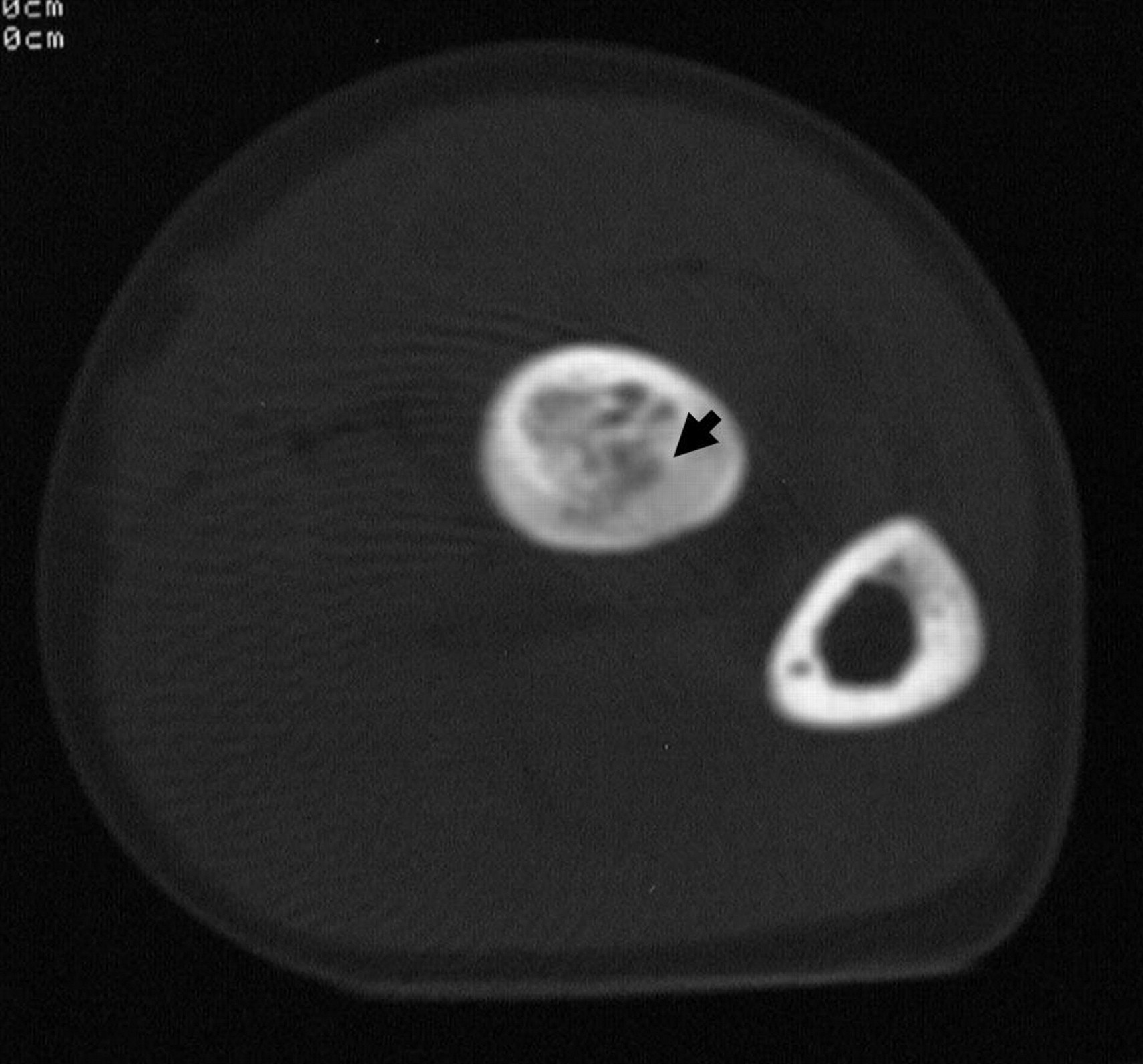
CT scan of the proximal forearm. A lucent area surrounded by a sclerotic rim in the proximal diaphysis of the radius was observed (arrow).

MRI of the forearm. T2 weighted image (below) depicted a small intermediate intensity area surrounded by a low intensity ring.
Our preoperative differential diagnosis included chronic inflammatory arthritis, osteomyelitis, and osteoid osteoma. The lesion was subsequently surgically removed. Intraoperatively, pronator teres showed fibrous degeneration and was therefore detached and elongated. Histological examination showed classic features of osteoid osteoma, consisting of osteoids and plump osteoblasts. At last followup examination, he showed no rotational limitation of the forearm.
The painless nature of the tumor in our patient is a rare phenomenon, and only 22 other cases are reported1–4. It is not feasible for very young patients to describe their symptoms accurately; and there were only 8 patients (36.3%) under the age of 5. Although it is unclear why the growth of the osteoid osteoma was painless, proposed hypotheses include absence of nerve fibers within the nidus5 and intramedullar location of the lesion6.
Osteoid osteoma arising in the elbow region often causes synovitis and leads to limitation of motion. Lesions occurring in the distal humerus and proximal ulna usually lead to loss of flexion and extension, whereas those that occur in the proximal aspect of the radius cause loss of pronation and supination. In our case, although there was no synovitis or joint effusion, there was a fibrous degeneration extending from the insertion of pronator teres, which led to impairment.
There are reports of spontaneous regression of symptoms after several years of treatment with oral medication7, but delay in the treatment of osteoid osteoma arising in the elbow could lead to permanent loss of motion since treatments for contracture of the elbow could be quite complex. Further, after a prolonged period of symptoms, cartilage destruction and osteoarthritis could develop8,9. It does not matter whether surgery is performed in a minimally invasive fashion using CT or by open surgery, but in cases involving the elbow we advocate removal over medical management.








{kind=link}
{kind=link}