

Abstract
The Patient Perspective Workshop included over 100 researchers and 18 patient participants from 8 countries. Following preconference reading and short plenary presentations, breakout groups considered work undertaken on measurement of sleep, assessing interventions to develop the effective consumer, and assessing psychological and educational interventions. The workshop explored the best way to identify other outcome domains (and instruments) that should be measured in observational or interventional studies with broader intentions than simply altering outcomes captured in the traditional “core set” plus fatigue. Four sleep questionnaires showed promise and will be the subject of further study. The Effective Consumer scale (EC-17) was reviewed and the concept Effective Consumer was well received. Participants thought it worthwhile to measure the skills and attributes of an effective consumer and develop an intervention that would include education in all of the scale’s categories. Assessment of educational and psychological interventions requires a wider set of instruments than is currently used; these should relate to the purpose of the intervention. This principle was extended to include wider measures of the impact of disease on life, as indicated in the International Classification of Functioning, Disability and Health. Life impact measure sets covering domains appropriate to different rheumatic conditions and focused on different interventions might be defined by future OMERACT consensus. Measurement instruments within these domains that are valid for use in rheumatic conditions can then be identified and, in the case of psychological and educational interventions, chosen to fit with the purpose of the intervention.
In 2006, following presentations by members of the OMERACT 8 Patient Perspective Workshop1 fatigue was added2 to the “core set” of 7 outcomes3 to be assessed in clinical trials of treatment for rheumatoid arthritis (RA). In preparation for the Patient Perspective Workshop at OMERACT 9, a position paper4 reviewed the inclusion of patient participants at OMERACT meetings and illustrated how this had resulted in direct incorporation of the patient perspective in the development of outcome assessments in rheumatology. It also drew together work in 3 other fields that were identified at previous OMERACT meetings as important patient-oriented measures of outcome: sleep, effective health consumers, and educational or psychological interventions. The position paper also introduced the concept that other core outcomes relevant to patients might be required in assessing interventions designed to help patients in living with their disease. This reflected the design of the workshop, which included over 100 researchers drawn from across the disciplines attending OMERACT 9. There were also 18 patient participants with a variety of rheumatological conditions [RA 8, fibromyalgia (FM) 4, gout 3, psoriatic arthritis 2, vasculitis 1] and from 8 countries (Australia 1, Canada 6, France 1, New Zealand 1, Sweden 1, The Netherlands 1, UK 2, USA 5). The workshop was cochaired by G. Wells, J. Kirwan, and P. Richards (PR is Chair of the OMERACT Patient Partners.) In addition to the preconference position paper4, there were brief introductory sessions first on the notion of a “core set” of patient oriented outcome measures (J. Kirwan), then on each of the other 3 topics (sleep: G. Wells; effective consumer: P. Tugwell; psychological and educational interventions: S Newman). Breakout discussion groups all included at least one patient. All groups considered the “core set” issue, and one-third of groups each dealt with one of the other 3 topics, as reported below. After report back sessions between participating groups on sleep, effective consumer, and psychological or educational interventions, the workshop ended with a plenary discussion on the best way to identify other outcome domains (and instruments to measure those domains) that should be measured in observational or interventional studies with broader intentions than simply altering the outcomes captured in the core set plus fatigue. Following the workshop, organizers met to synthesize a broad set of proposals arising from the introductory presentations, the group discussions, and the feedback, which are presented below. These proposals were presented in outline and voted on at the final OMERACT plenary session.
ASSESSING SLEEP DISTURBANCE
During the plenary voting at OMERACT 6 a research agenda was identified that incorporated the need for adequate measuring tools for sleep disturbance. The focus here is on sleep quality in patients with RA. For properly assessing sleep for patients with RA, the availability, applicability, and responsiveness of measures of sleep quality in RA patients need to be evaluated. Work described in the OMERACT position paper4 was presented in more detail (G. Wells). This included an overview of all sleep assessment instruments found during a literature review, a listing and description of all the domains identified from within these sleep questionnaires, and an initial assessment of their suitability for use in RA. Various characteristics of the instruments were summarized including: the psychometric properties of reliability, validity, and responsiveness; applicability of feasibility and interpretability; and measurement model properties such as number of items, response format (most of the instruments had a Likert or visual analog scale), scoring system, timeline, and complexity that varied from a single domain to multifactorial.
Breakout groups took on several specific tasks related to this information, including ranking of the importance of different domains, judgments about the suitability of the wording of different questions, and assessments about the likely applicability of 15 instruments preselected because of their characteristics in the literature. Drawing these 3 different approaches to reviewing instruments that might be suitable for measuring sleep in RA, a “local plenary” of the 3 groups ranked the potential of each of the instruments. Four show enough promise to explore with confidence: the Athens Insomnia Scale; the Medical Outcomes Study — Sleep; the Pittsburg Sleep Diary; and the Women’s Health Initiative Insomnia Scale. A more detailed report of this work is provided in the accompanying article9.
EVALUATING PROGRAMS TO CREATE EFFECTIVE HEALTH CARE CONSUMERS
An update on the Effective Consumer project was presented (P. Tugwell and colleagues). This included the developmental history of the scale5 leading to the present version (EC-17) and its detailed performance when used before and after patients had taken part in an Arthritis Self-Management Program6. Participants at OMERACT 9 contributed to the continuing development of the Effective Consumer scale after these presentations in 2 ways: (a) by discussing the content of the questionnaire and the results from the intervention study6, and (b) considering whether a proposed intervention based on the Ottawa Decision Support Framework and international standards for patient decision aids7,8 would likely improve performance in the domains included in EC-17. (The proposed intervention explains treatment options, how to clarify the patient’s values, provides structured guidance or coaching in deliberation and communication, summarizes the patient’s values and preferences, identifies gaps in knowledge, and indicates the person’s readiness to make a decision or take other action regarding his or her chronic condition. A printed summary of the session is produced for the patient upon completion to help the patient reflect on the options and to aid communication with a physician.)
Participants in this section of the workshop, 10 patients and 25 clinicians and other researchers, raised the following concerns: (a) The tone of some items, which could be perceived as aggressive, for example, the word “negotiate” was problematic for some participants because it seemed adversarial. (b) The general reading level required for responding to items: Some participants did not understand the meaning of specific items. Further, some items represented a particular cultural outlook, which might not be appropriate for some patients completing the questionnaire. Suggestions were made for rewording a number of items. (c) The items seem to imply that effective consumers needed to be independent. Some participants recommended changing the wording to reflect a more collaborative intention. (d) Include time since diagnosis in the demographic information. Many participants felt people may answer items differently depending on whether they were recently diagnosed or had been living with their condition for some time.
Participants also discussed the deficits in patients’ effective consumer abilities before and after the Arthritis Self-Management Program, as detected in the analyses presented6. There was debate over whether some cultures or populations would appear to show deficits in items about communication and negotiation, since it might be unusual or even inappropriate in certain cultures to be assertive in a healthcare encounter. In these contexts, deficits might not be modifiable by an intervention external to the culture. Could the culture of the researchers developing the questionnaire have added a hidden set of value judgments? Similarly, if a person is part of a healthcare system that does not allow for extensive discussion or shared decision making, he or she may be restricted in how much improvement can be made.
Participants next discussed the need for a tailored intervention to be developed in response to the identified deficits. Opinion about this intervention was favorable. Participants felt that an interactive educational session in the form of a self-directed, online decision aid would be helpful in guiding people to communicate effectively and enabling them to feel confident during encounters with the health system. Most felt that such an intervention would be an effective tool to find common ground when discussing issues with healthcare professionals, and that it could help to reduce patient anxiety about healthcare choices.
Overall, the concept of an Effective Consumer was well received. Most participants thought it was worthwhile to measure the skills and attributes of an effective consumer and were enthusiastic about development of an intervention (such as the proposed online decision aid) that would include education in all of the categories presently found in the scale. A more detailed report of this work is provided in the accompanying article6.
EVALUATING EDUCATIONAL AND PSYCHOLOGICAL INTERVENTIONS
A presentation (S. Newman) summarized the issues from the previous Special Interest Group10 and those in the position paper4. This contrasted the design and evaluation of educational and psychological interventions with those of pharmacological treatments, the latter being more commonly considered at OMERACT. The important differences were highlighted: (a) That blinding participants in educational and psychological interventions to the nature of the intervention was not possible, in contrast to the placebo used in pharmacological interventions. (b) Related to the lack of concealment of the intervention was that participants in educational and psychological interventions may have a clear preference for one intervention over another. Not receiving their preference could have an impact on their attitude and outcome of the trial. (c) While the placebo in pharmacological studies is designed to appear identical to the active intervention this is not feasible in educational and psychological interventions where it is often difficult to design a credible control condition. (d) Most pharmacological interventions generally have a known mechanism of action. In contrast, in order to understand the mechanism of action of the multi-component nature of most educational and psychological interventions, there is a need to assess process variables along with outcomes. (e) The fifth difference served to focus the discussion groups and considered the appropriateness of the core outcome measures in the assessment of educational and psychological interventions. Educational and psychological interventions are very diverse and for example might be directed at changing the mechanisms for dealing with symptoms of disease (such as coping) or be focussed on improving psychological well being or designed to improve participants’ confidence in dealing with their arthritis (self-efficacy) while others may be directed to changing symptoms. Importantly these outcomes are likely to be related to each other e.g., any reduction in symptoms may lead to improved psychological well being.
Breakout groups next considered specific questions related to outcome assessment in psychological and educational interventions and reported back to a “local plenary” session where the different views were integrated. The first question considered was whether outcomes of psychological and educational interventions should be defined by the different rheumatological conditions. This would result in, for example, osteoarthritis (OA), RA, and FM each having a core set of outcomes with which psychological and educational interventions would be evaluated. The breakout groups considered that the condition should influence the nature of the outcomes but that issues such as the nature of the intervention and the chronicity of the condition were more important.
There was a clear recognition that the current “core set” of outcomes plus fatigue is far from adequate for detecting the consequences of psychological and educational interventions. The outcomes of potential interest in these interventions may cover those in the core set but also include: impact on quality of life, coping, maintaining independence, pain, self-image, anxiety, depression, physical function, relationships, performing a work role, and sleep. In some cases process variables (e.g., self-efficacy, illness cognitions, locus of control) may also be the focus of psychological and educational interventions.
Deciding which outcomes would be appropriate for specific interventions would depend on the intention or purpose of the intervention. There will be circumstances in which the broader, “life-impact” outcomes will be the primary outcome of a study, while the disease-related measures will be secondary or control variables. An example might be an educational intervention helping patients to schedule their daily physical workload to avoid times of fatigue. The primary outcome may be the continued maintenance of employment and/or achievement of work aims, while the secondary outcome of fatigue in this type of intervention might be expected to remain unchanged.
Discussion emphasized the need to define a reduced number of outcome variables in psychological and educational interventions and identify those that had good psychometric properties. It recognized the difficulty of comparing across studies where different measures were made of the same underlying construct. It was suggested that specifying appropriate outcome variables that could be common to certain types of intervention should be a major research goal along with a clear understanding of what constitutes a good measure.
OUTCOMES FROM A BROADER PATIENT PERSPECTIVE — LIFE IMPACT MEASURES (LIM)
From the broad collection of topics identified at the OMERACT workshops has emerged the concept that there might be a “patient core set,” to complement the traditional clinical core set of outcomes (particularly in relation to RA, where most of the OMERACT related work has been undertaken). The position paper4 postulated 3 possible relationships between this notion and the existing core set (plus fatigue) used to describe outcomes in RA3: that they might be 2 sides of the same coin; that they may overlap to some extent in the way they capture the nature of RA; or that there may be very little relationship between them. In the latter case patients may not be trying to measure RA as the consequence of a disease process, but rather be seeking information about, for instance, the effects of RA on their life in general. The introductory presentation (J. Kirwan) drew particular attention to the latter possibility and related it to the International Classification of Functioning, Disability and Health (ICF) (Figure 1). Could it be that the current core set concentrates on body functions and structures, while patients seek outcome measures related to activities and participation? If so, is there a need for another well defined set of measures to be used in this area? The main purpose for this part of the workshop was to seek consensus on the way forward and to develop a research agenda.
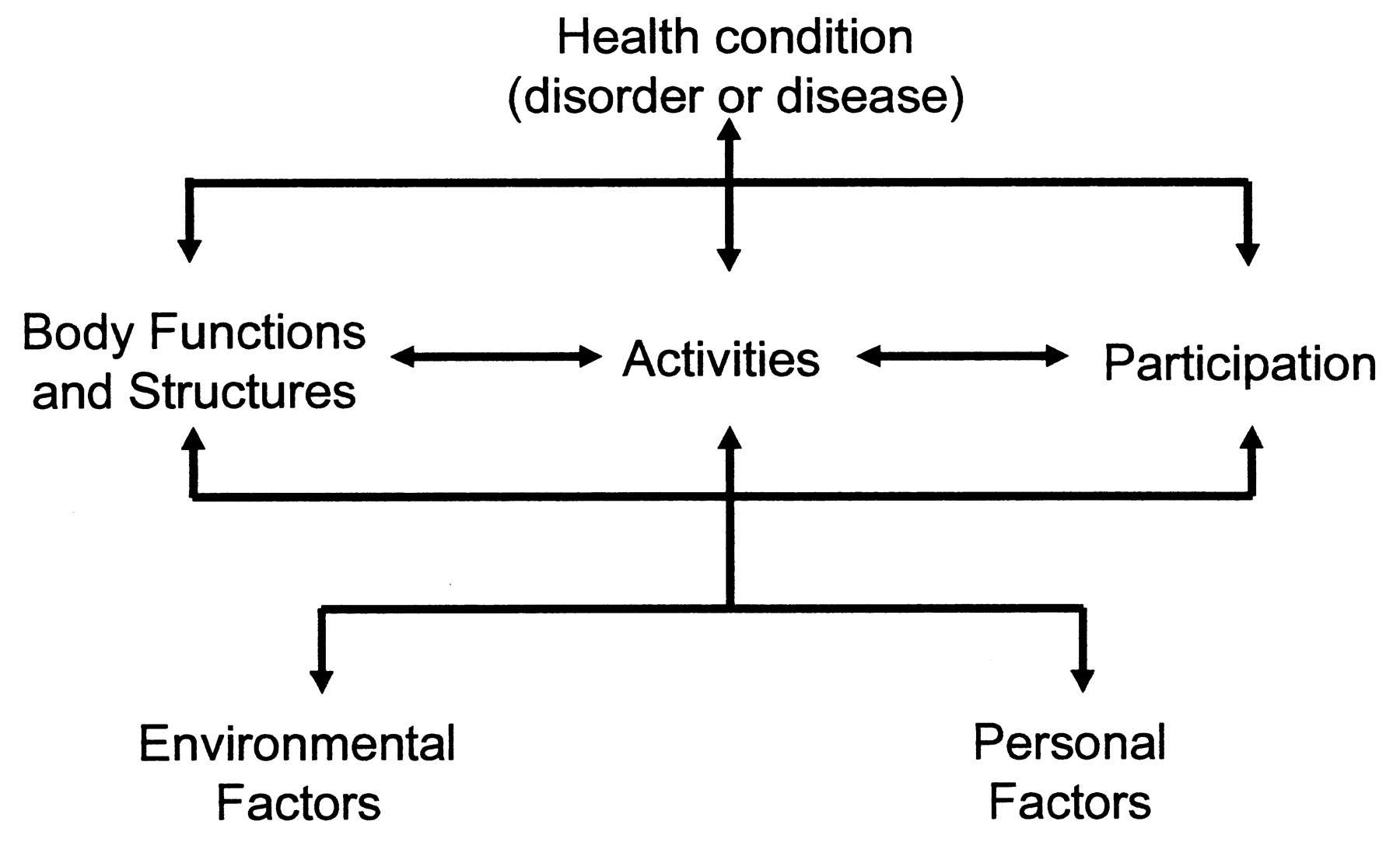
Representation of the International Classification of Functioning, Disability and Health11.
Participants agreed on the definition of a core set as a group of outcomes that is to be measured in all clinical trials. We agreed that this core set needed to include (as it does) patient-reported outcomes such as fatigue and pain. However, there was a clear and unequivocal expression of the need to capture the wider aspects of chronic disease as highlighted by patient participation.
There was disagreement about whether a separate “patient core set” needed to be developed on other patient-reported outcomes that relate to impact on life, such as social functioning and participation. Advantages of developing a validated set of outcomes for these LIM were that different outcomes could be selected depending on the disease, context, and purpose of the intervention. In chronic disease, these outcomes could “raise the bar” for clinicians, by highlighting that there is more to managing rheumatologic conditions than disease control, and that other areas of social functioning need attention. They might provide a comprehensive patient-level description, and help manage patient expectations and understanding and so better inform clinical outcome. Such outcome measures might also contribute to better understanding of the entirety of the disease when utilized in combination with clinical/biological indicators, and shift the modern biological and technological focused physician back to the patient.
A disadvantage to separating these life impact outcomes from the core set was that patient-important outcomes might receive less attention if they were not included in the core set. It was also recognized that different measures may be required for different diseases or different types of intervention, although sometimes quite substantial overlap may exist. It was noted that current research on the views of patients in relation to a more global descriptive framework (at the European League Against Rheumatism and by Hewlett and colleagues) would provide data on what the patients would like measured to assess RA.
In a synthesis of these ideas, broadly supported by reporters from the discussion groups and including some of the observations from the sleep, effective health consumer, and psychological intervention discussions, an alternative representation of the ICF can be used as a backdrop to suggest how LIM might relate to the current core set (Figure 2).

A rearrangement of the International Classification of Functioning, Disability and Health diagram shows how different domains (circles) of life impact measures may be appropriate “core” requirements (in addition to the core set) for interventions addressing activities and participation, and how these are more likely to interact with environmental and personal factors, which may also need to be measured.
In this arrangement, appropriate instruments to measure the domains need to be identified and validated (as is being undertaken for sleep disturbance) or developed (as is being undertaken for effective health consumer assessment). The ICF approach provides an excellent backdrop with which to consider the different domains required to identify and/or develop LIM. However, it will be important to ensure the psychometric properties of such instruments are adequate for the circumstances of their intended use.
It also seems likely that domains more distant from body functions altered by a specific health condition are less likely to be disease specific. Thus the measures of environmental factors, personal factors, and participation will cross diseases and types of intervention, resembling the interleaving of the upper canopy of a forest, while disease specific measures of more immediate pathological consequences and of disease-related activities of daily living resemble individual tree trunks with their roots in particular disease pathologies.
In conclusion, from these discussions has emerged a clearer picture of progress, and a research agenda as shown in Table 1. For sleep measurement, 4 current scales show enough promise of validity for use in RA to explore with confidence: the Athens Insomnia Scale, the Medical Outcomes Study—Sleep, the Pittsburg Sleep Diary, and the Women’s Health Initiative Insomnia Scale. For evaluating programs to create effective healthcare consumers, the EC-17 scale currently under development (Tugwell and colleagues) is reaching maturity and is at a stage where it can be incorporated into appropriate randomized controlled trials to explore its responsiveness. For evaluating educational and psychological interventions, there was agreement that psychoeducational interventions may need disease specific outcome assessments, but that chronicity and type of intervention are also important. However, the type of intervention and its purpose were considered to be the most powerful determinants of the required outcomes to measure. The current “core set” does not capture these relevant outcomes. For the general concept of identifying wider outcomes of direct concern to patients, the notion of LIM has emerged. The voting in the final OMERACT plenary session supported these broad conclusions (Table 2). The research agenda should focus on determining which domains among LIM are appropriate for different types of intervention and which measuring instruments are valid for use in those domains. In this way, “LIM core sets” may emerge for specific interventions or situations, to be used in conjunction with the current core set.
A research agenda for investigating the use of life impact measures.
Voting results of the OMERACT 9 plenary session.








{kind=link}
{kind=link}