

Abstract
Objective. This randomized controlled study addressed whether sonographic needle guidance affected clinical outcomes of intraarticular (IA) joint injections.
Methods. In total, 148 painful joints were randomized to IA triamcinolone acetonide injection by conventional palpation-guided anatomic injection or sonographic image-guided injection enhanced with a one-handed control syringe (the reciprocating device). A one-needle, 2-syringe technique was used, where the first syringe was used to introduce the needle, aspirate any effusion, and anesthetize and dilate the IA space with lidocaine. After IA placement and synovial space dilation were confirmed, a syringe exchange was performed, and corticosteroid was injected with the second syringe through the indwelling IA needle. Baseline pain, procedural pain, pain at outcome (2 weeks), and changes in pain scores were measured with a 0–10 cm visual analog pain scale (VAS).
Results. Relative to conventional palpation-guided methods, sonographic guidance resulted in 43.0% reduction in procedural pain (p < 0.001), 58.5% reduction in absolute pain scores at the 2 week outcome (p < 0.001), 75% reduction in significant pain (VAS pain score ≥ 5 cm; p < 0.001), 25.6% increase in the responder rate (reduction in VAS score ≥ 50% from baseline; p < 0.01), and 62.0% reduction in the nonresponder rate (reduction in VAS score < 50% from baseline; p < 0.01). Sonography also increased detection of effusion by 200% and volume of aspirated fluid by 337%.
Conclusion. Sonographic needle guidance significantly improves the performance and outcomes of outpatient IA injections in a clinically significant manner.
Ultrasound as an imaging technology in musculoskeletal medicine is increasingly used as a routine diagnostic modality in the clinic, and is often used as an extension of the physical examination1–5. Sonographic needle guidance is also becoming increasingly popular in routine office injection procedures by clinical musculoskeletal experts6–10. In terms of accuracy of intraarticular (IA) placement of the needle by palpating surface anatomy by skilled orthopedic surgeons and rheumatologists, the results are generally dismal, with an unintended non-IA injection rates as high as 50%–60%10–26. In contrast, sonographic image guidance routinely improves the accuracy of IA positioning of the needle tip, and permits IA injections with 96%–100% accuracy27–41. However, there is limited evidence that routine use of sonographic needle guidance actually causes a clinically significant improvement in the outcome relative to traditional palpation-guided methods42–45. This paucity of outcome data has resulted in challenges to sonography and has provoked skepticism and resistance to fully integrating image-guided procedures into the musculoskeletal clinic42–48.
Thus, there is great need for outcome studies to address the role of sonographic needle guidance in routine IA injection procedures42,47,48. Our randomized controlled study addressed whether routine use of sonographic needle guidance with enhanced needle control affected the clinical outcomes of joint injections in a typical outpatient musculoskeletal office practice.
MATERIALS AND METHODS
Subjects
This project was in compliance with the Helsinki Declaration and was approved by the institutional review board (IRB). This study is registered at ClinicalTrials.gov (NCT00651625) and is a concerted research effort to evaluate and integrate safety technologies into procedural medicine. Patient confidentiality and privacy were protected according to the Health Insurance Portability and Accountability Act (HIPAA). All products used in these procedures were commercially available, FDA-approved, CE-marked, and used on-label.
Inclusion criteria included (1) focal joint pain attributed to arthritis unresponsive to conventional modalities (analgesics, antiinflammatory medications, exercise, or splinting as appropriate); (2) pain with passive range of motion of the joint; (3) impairment of the activities of daily living related to pain; (4) significant pain by the 0–10 cm visual analogue pain scale (VAS pain scale) in the involved joint, where VAS ≥ 5 cm; and (5) the wish of the patient to have IA corticosteroid injection49–51.
Exclusion criteria included (1) obvious tendon-ligamentous pathology or internal derangement; (2) superficial bursitis; (3) endstage joint by radiography; (4) confounding neuropathy; (5) hemorrhagic diathesis; (6) use of warfarin or antiplatelet drugs; or (7) the presence of infection.
Altogether, 150 subjects that fulfilled these criteria entered the study and were randomized to conventional injection by anatomic palpation or to sonographic needle guidance with enhanced needle control. Patient groups were equivalent in terms of sex, age, underlying condition, joints, and baseline pain (Table 1). All palpation-guided injections were performed directly by experienced expert physicians; all sonographically guided injections were performed by rheumatology fellows-in-training directly supervised by experienced expert physicians. The sonographically guided injection technique utilizing a control syringe was developed by the interventional radiologist in the group (RRS). Only 148 subjects completed the protocol, with 2 (1 in each group) who did not complete and were excluded from the study. Of the 148 subjects, 100 had rheumatoid arthritis and 48 had osteoarthritis, and they were equally distributed between the 2 treatment groups (Table 1). The joints consisted of 94.6% large joints (knee, hip, shoulder, elbow, wrist, ankle) and 5.4% small joints (interphalangeal and metacarpophalangeal joints) in the following proportions: 41.9% knee (n = 62), 18.9% wrist (28), 14.9% shoulder (22), 10.8% hip (16), 5.4% elbow (8), 2.7% ankle (4), and 5.4% interphalangeal or metacarpophalangeal joints (8), equally divided between the 2 treatment groups. Three subjects in each group had palpable effusions.
Patient characteristics. Values are mean ± SD unless otherwise indicated.
Sonographic needle guidance with enhanced needle control
The sonographic-guided injection procedure was also performed in a standardized manner using a one-needle 2-syringe technique (Figures 1–3). First, relevant anatomic landmarks and the intended needle target were palpated and marked with ink prior to applying ultrasound gel, as ultrasound gel wets the skin and interferes with subsequent marking (Figures 1 and 2). Although not standard to the art, during sonographic examination, these surface markings permit facile correlation of the deeper 2-D sonographically visible anatomy to surface anatomy and the position of the ultrasound transducer, all of great utility for precise sonographic direction of the needle. Standard approaches were used for all joints: noneffusive knee (lateral 90° bent knee approach), effusive knee (straight leg, lateral suprapatellar bursal-subpatellar approach), shoulder (anterior approach), wrist (dorsal distal radial tubercle approach), ankle (lateral subtibial approach), elbow (lateral superior olecranon approach), and small finger joint (lateral dorsal sub-extensor tendon approach). A portable ultrasound unit with 2 high frequency linear array transducers and one low frequency curvilinear array transducer was used for all procedures (Sonosite M-Turbo; SonoSite, Inc., Bothell, WA, USA). A 60-mm 5–2 MHz curved array transducer was used for hips, a 10–5 MHz 38 mm broadband linear array transducer was used for other large joints (shoulder, knee, wrist, ankle, and elbow), and a 13–6 MHz 38 mm 25 broadband linear array probe was used for small joints of the fingers. After marking the surface anatomy with ink, the deeper anatomy was interrogated with sonography, confirming or adjusting anatomic landmarks that had been marked previously by palpation. If a joint effusion was present by sonography, the effusion rather than the cartilage surface became the new target for the needle. Because it is most efficient during a sonographic procedure for the operator to simultaneously control both the needle and the ultrasound probe in order to readily direct the ultrasound beam, a one-hand control syringe, the reciprocating procedure device (RPD), was used for all sonographically guided procedures (Avanca Medical Devices, Albuquerque, NM, USA; Figures 2 and 3). Clinical trials have demonstrated that control syringes provide improved safety and enhanced needle control during joint procedures52–57. If an effusion was present sonographically the larger 10 ml or 25 ml RPD control syringe was used; if the joint was dry with no sonographically visible effusion, the smaller 3 ml or 5 ml RPD was selected.

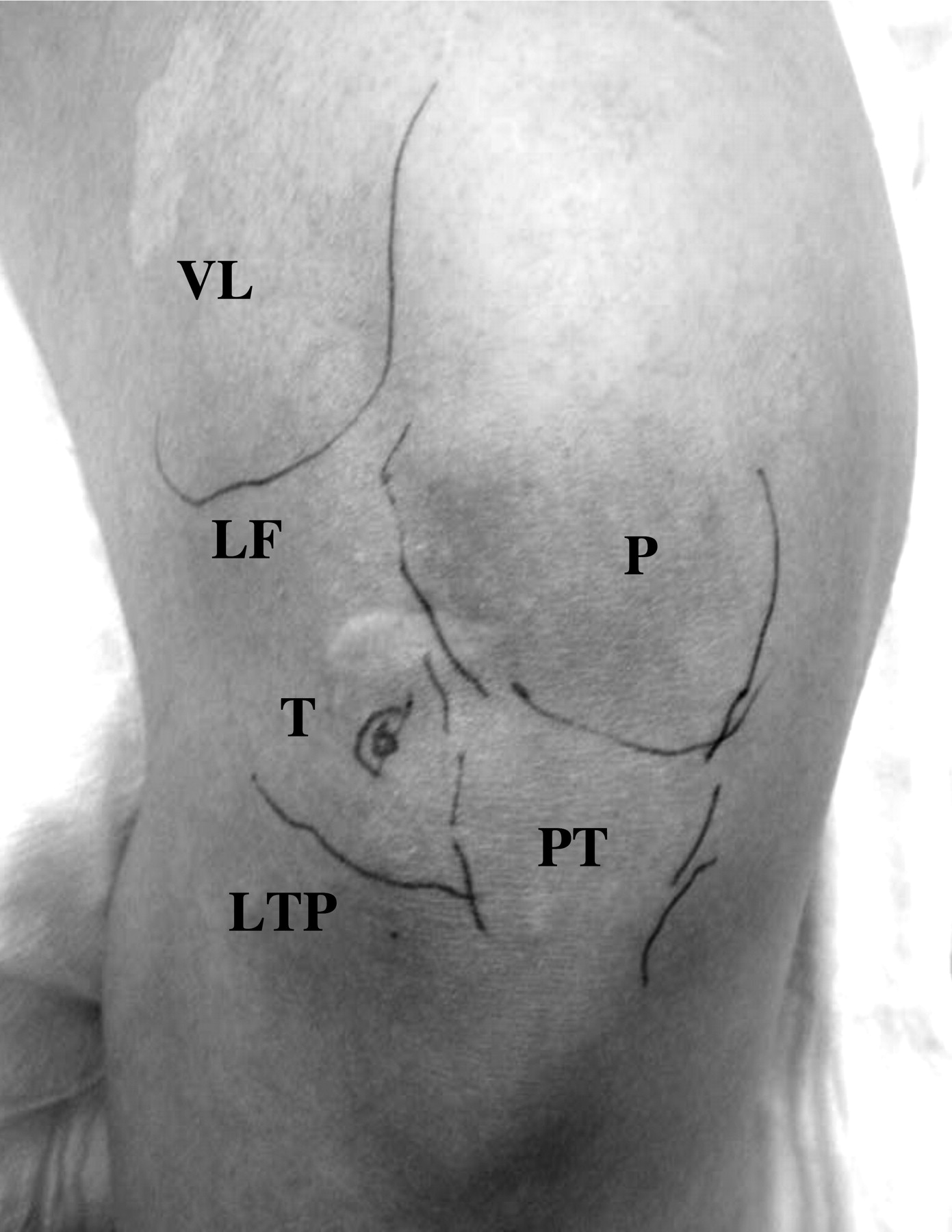
Palpation-guided anatomic markers. Anatomic landmarks are first identified by palpation and marked with ink prior to the procedure for both palpationguided and sonography-guided intraarticular procedures. VL: vastus lateralis, LF: lateral femoral condyle, LTP: lateral tibial plateau, PT: patellar tendon, P: patella, T: target for lateral inferopatellar bent knee approach.

Introduction of the needle. The reciprocating procedure device (RPD) control syringe is used with 2 hands to carefully introduce the needle and administer lidocaine. Depressing one plunger causes the RPD control syringe to aspirate and depressing the other causes the device to inject. After partially introducing the needle, the RPD is operated with one hand and the ultrasound transducer is operated with the other hand.

Sonographically guided intraarticular needle introduction with enhanced needle control. Under sonographic guidance, the needle is introduced further intraarticularly. The ultrasound transducer is operated with one hand and the RPD control syringe with the other, providing enhanced control of both transducer and needle by a single operator.
For large joints a 22-gauge 1.5 inch safety needle and for small joints a 25-gauge 1 inch safety needle were used (305761-25 g 1” and 305783-22 g 1.5” BD Eclipse™ Needle; Becton Dickinson, Franklin Lakes, NJ, USA). Prior to the procedure the RPD control syringe was filled with 2% lidocaine (3 ml for large joints, 1.0 ml for small joints; Xylocaine® 2%; AstraZeneca Pharmaceuticals LP, Wilmington, DE, USA). To penetrate the skin, the ultrasound transducer was set down, and 2 hands were used to precisely manipulate the RPD control syringe while introducing the needle through the skin and subcutaneous tissues deeper towards the IA target, alternatively aspirating for blood and synovial fluid on return and, if not present, then injecting lidocaine (Figure 2). Once the needle was partially introduced into the tissues and thus directionally stable the ultrasound transducer was taken up again with the free hand and the RPD control syringe was operated with the other hand, keeping the plane of the transducer and ultrasound beam in the same plane as the long axis of the needle (Figure 3). Once the needle was visualized, the needle was sonographically guided to synovial fluid pockets in the effusive joint and joint cartilage in the dry joint (Figure 4). Any synovial fluid was fully aspirated with the control syringe prior to injecting corticosteroid. In the dry noneffusive joint, the needle tip was directed sonographically until it penetrated the synovial membrane and was directly adjacent to the cartilage surface (Figure 4). If the needle was too short to reach the cartilage surface, it was extracted and a longer 2 or 3 inch needle was used. With the needle tip against the cartilage surface, lidocaine was then injected intraarticularly with true IA positioning optimized by (1) visualizing the needle tip directly adjacent to cartilage (Figure 4); (2) easy injection of lidocaine without resistance (Figure 3); (3) synovial fluid return into the control syringe; (4) the lack of sonographic visualization of “back-flow” of lidocaine away from the needle tip into periarticular tissues (Figure 5); and (5) sonographically visualized expansion of the IA synovial space as the lidocaine was injected (Figure 6). After the lidocaine was completely injected intraarticularly as above, the ultrasound transducer was temporarily set down, and using one hand to hold the RPD and the other hand the needle hub, the RPD control syringe was rotated off the IA needle, and a 3 ml conventional syringe prefilled with triamcinolone acetonide suspension [80 mg for the knee, shoulder, and hip, 60 mg for wrist and ankle, and 20 mg for small joints of the fingers; Kenalog® 40, Westwood-Squibb Pharmaceuticals (Bristol-Myers Squibb), New York, NY, USA] was attached to the IA needle. The ultrasound transducer was taken up again, the needle tip positioning was again visualized directly adjacent to cartilage, and a small amount of triamcinolone was then injected. If there was backflow (Figure 5) the needle was advanced toward the cartilage surface until the backflow subsided and the IA space was seen to expand. If there was no sonographically visible backflow away from the needle tip into periarticular tissues and the IA space could be seen to expand further with the test injection, the remainder of the corticosteroid was injected (Figure 6). Needle removal was always visualized sonographically, and then firm pressure was applied to the puncture site.

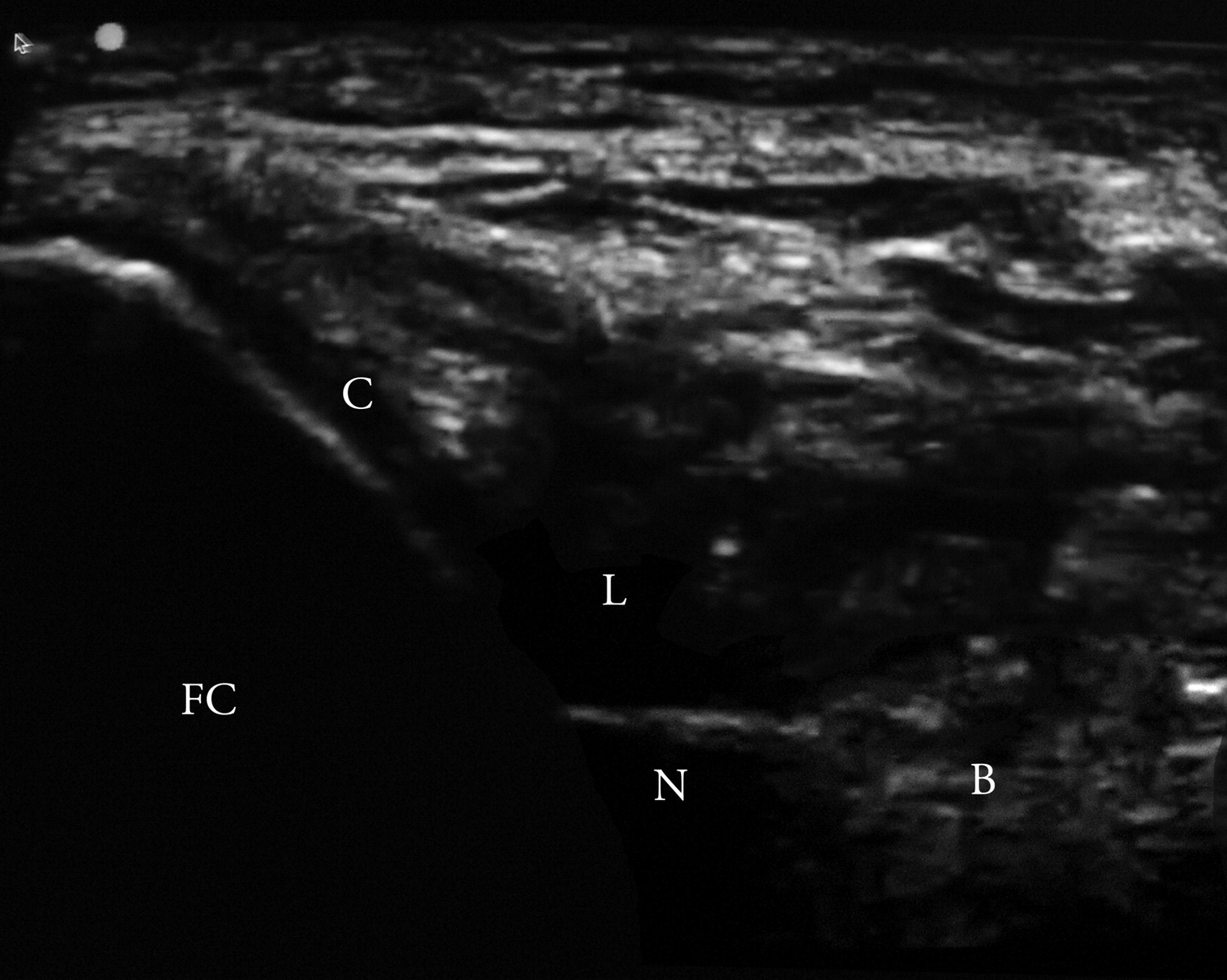
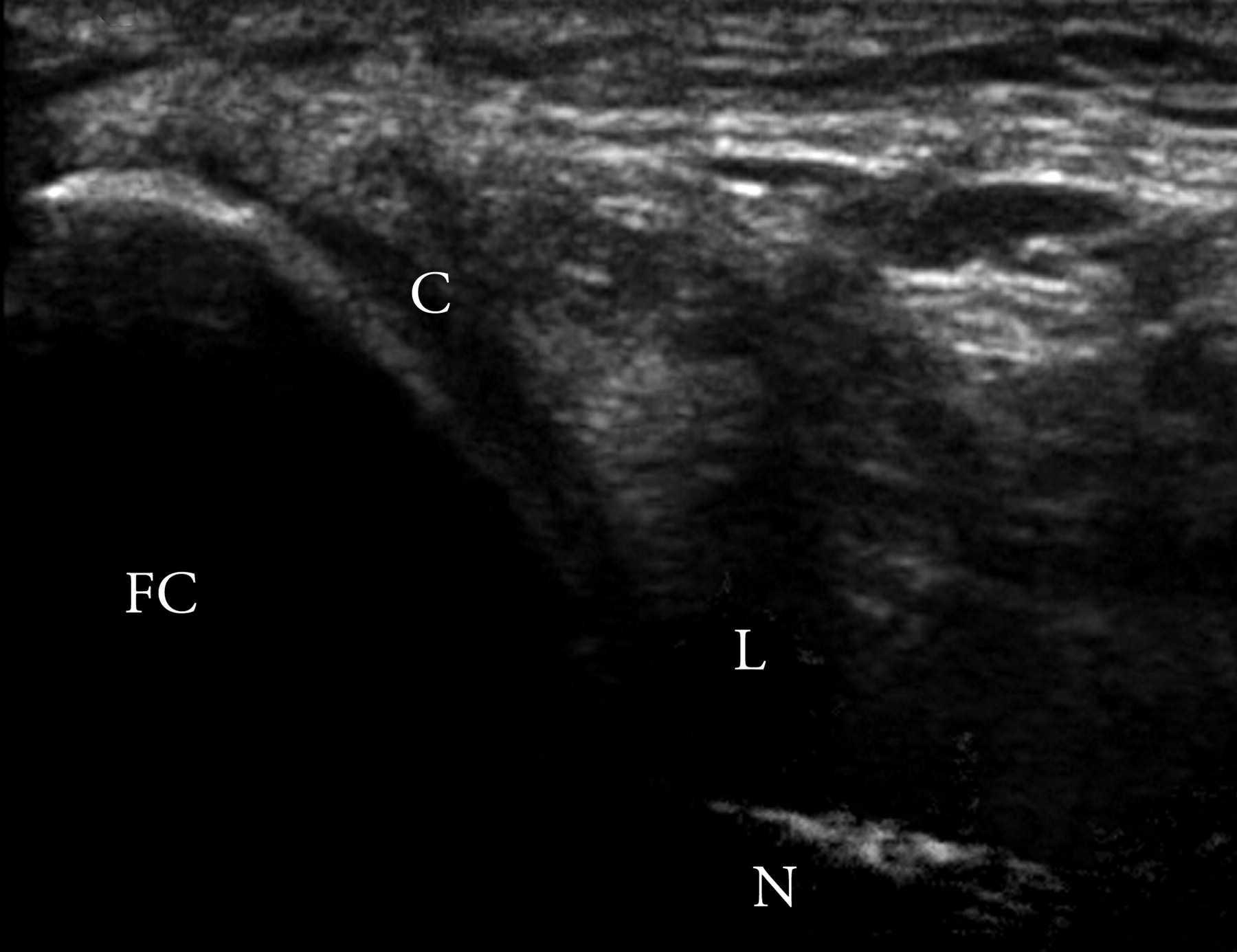
The needle is advanced under direct sonographic guidance until the needle tip (N) is directly adjacent to the medial femoral condyle (FC). Extraarticular lidocaine (L) can be seen outside the joint, as well as intraarticularly next to the articular cartilage (C). The ultrasound (US) probe is resting horizontally over the medial compartment of the bent knee, with the needle inserted from the lateral infrapatellar side, the needle tip directed toward the medial femoral condyle. The long axis of the US probe is parallel to the needle.
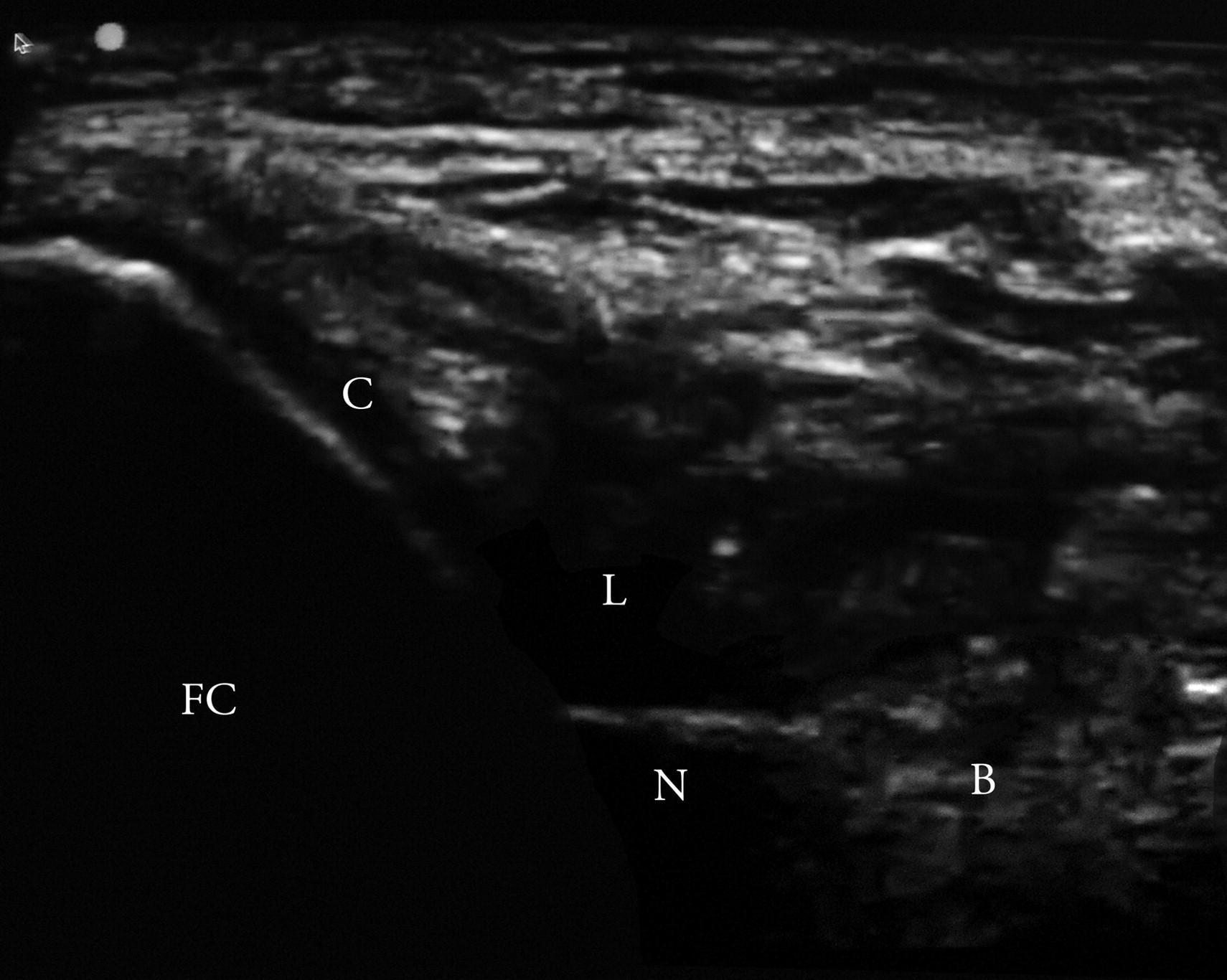
Sonographic visualization of backflow from the needle. With the needle tip (N) directly adjacent to the articular cartilage (C) of the femoral condyle (FC), a test dose of lidocaine (L) is injected. The needle tip is not in a completely intraarticular position as shown by the visible backflow (B) of lidocaine along the needle shaft into the extraarticular tissues. The US probe is resting horizontally over the medial compartment of the bent knee, with the needle inserted from the lateral infrapatellar side, the needle tip directed toward the medial femoral condyle. The long axis of the US probe is parallel to the needle.
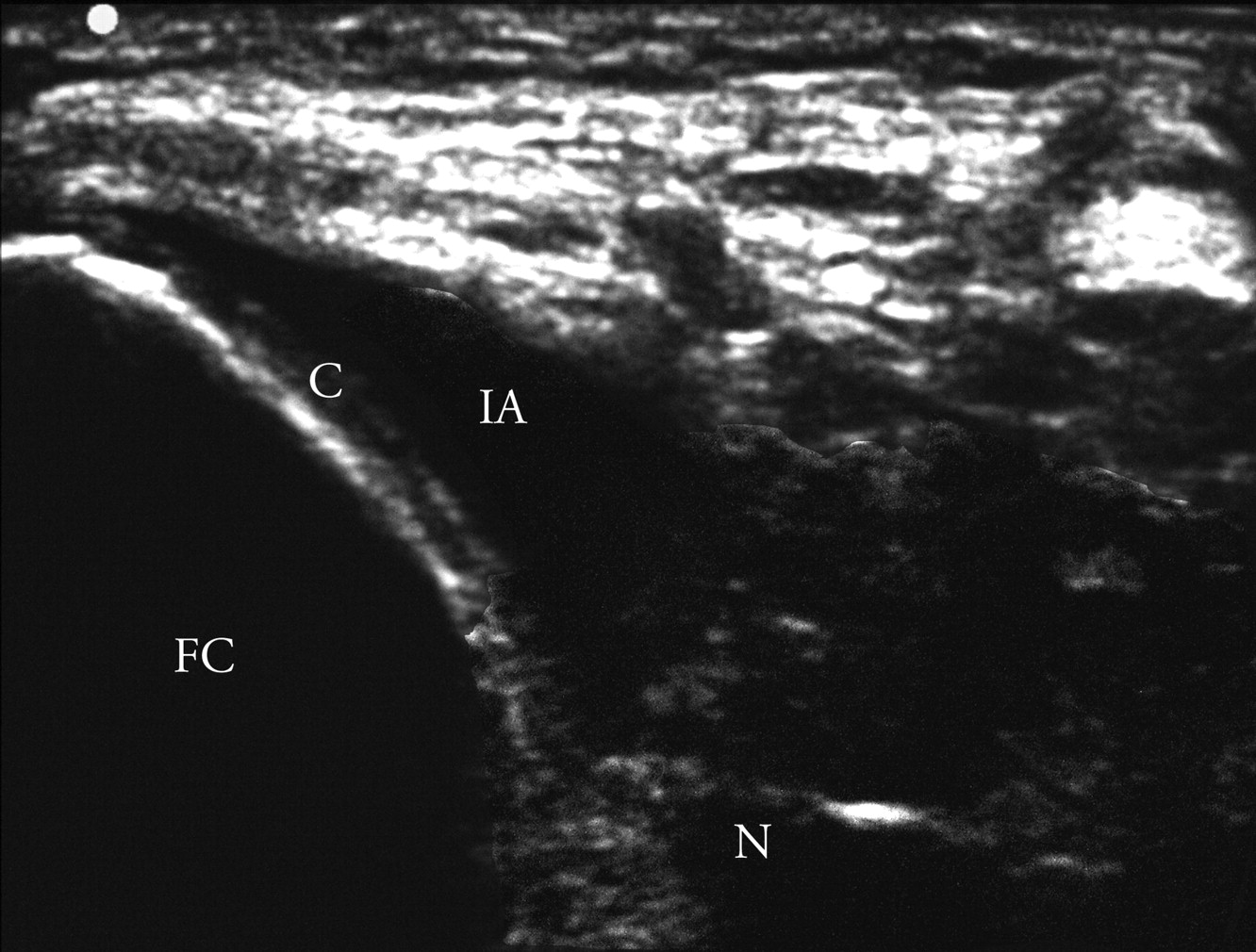
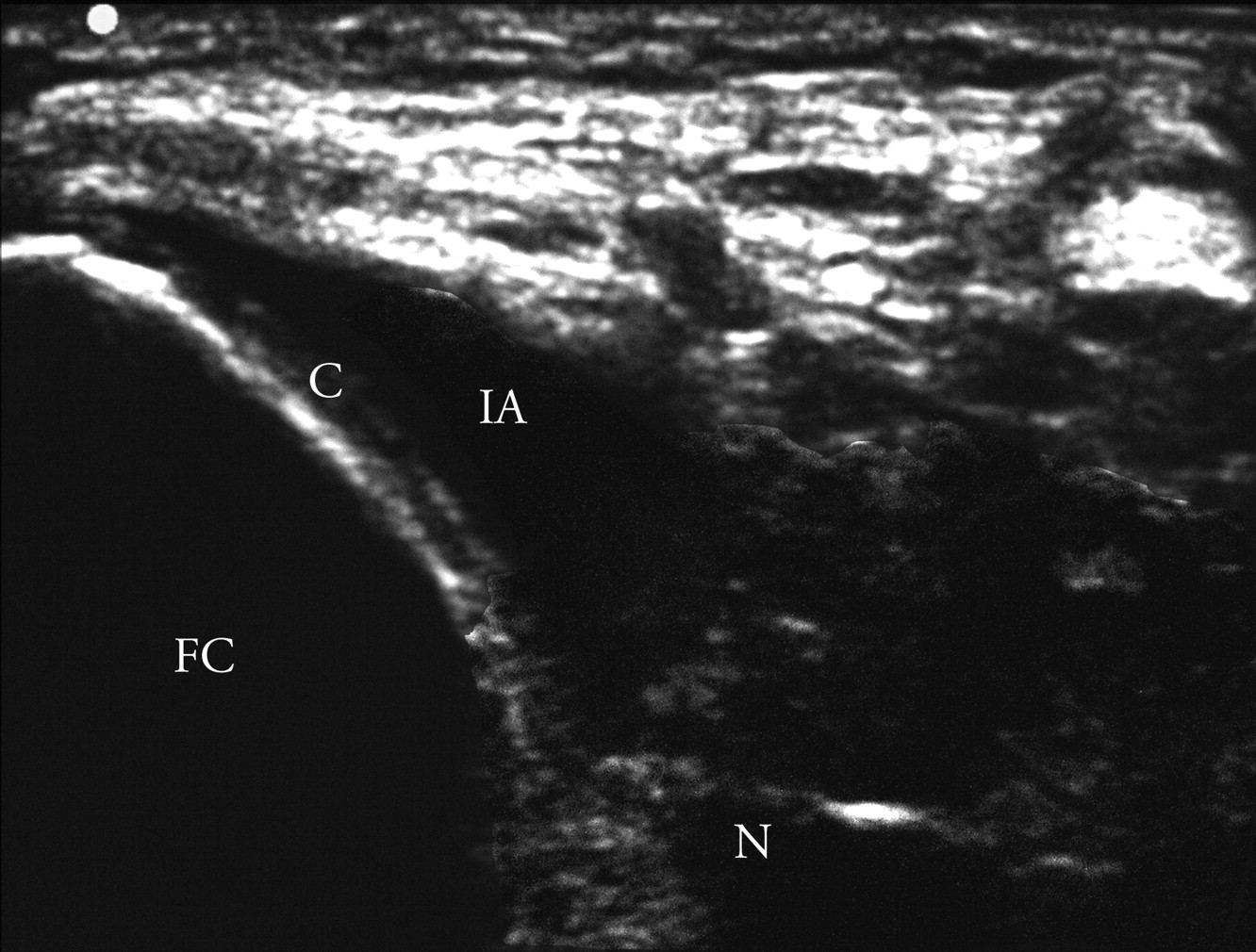
Sonographic visualization of direct intraarticular injection. After manipulation and rotation of the bevel, the needle tip (N) is in a completely intraarticular position as shown by the visible mass of intraarticularly injected lidocaine (IA) over the articular cartilage (C) of the medial femoral condyle (FC). Backflow of lidocaine into extraarticular tissues is no longer present. The US probe is resting horizontally over the medial compartment of the bent knee, with the needle inserted from the lateral infrapatellar side, the needle tip directed toward the medial femoral condyle. The long axis of the US probe is parallel to the needle.
Palpation-guided injections
The palpation-guided injection procedure was also performed in a standardized manner using the one-needle 2-syringe technique exactly as above but without sonographic guidance. A conventional syringe (Ref. 309604; Becton Dickinson) operated with 2 hands was used for all palpation-guided procedures.
Outcome measures
Patient pain was measured with the standardized and validated VAS pain scale, where 0 cm = no pain and 10 cm = unbearable pain53–61. Significant pain was defined as a VAS ≥ 5 cm. Pain by VAS was determined (1) prior to the procedure (baseline pain), (2) during the procedure (procedural pain), and (3) at 2 weeks post-procedure (pain at outcome). Two to 3 weeks has been demonstrated as the outcome measurement time most likely to reveal maximum clinical effect of injected corticosteroid based on clinical trials of IA corticosteroid injections that demonstrated a peak effect of the IA corticosteroids at 2 to 3 weeks, with a return to placebo levels by 4 weeks49–51,62–64. Specific outcome measure derivatives at 2 weeks were (1) absolute VAS pain scores; (2) percentage change in VAS pain scores from baseline to outcome; (3) significant pain at outcome (VAS ≥ 5 cm); (4) percentage of responders (defined as a decline in VAS from baseline to outcome ≥ 50%); (5) percentage of nonresponders (decline in VAS from baseline to outcome < 50%); and (6) significant pain in nonresponders (defined as percentage of individuals with significant pain, VAS ≥ 5 cm) at outcome52–58.
Statistical analysis
Data were entered into Excel (Version 5, Microsoft, Seattle, WA, USA) and analyzed in SAS (SAS/STAT Software, Release 6.11, Cary, NC, USA). Differences between parametric 2-group data were determined with the t test with significance reported at the p < 0.05 level. Differences in categorical data were determined with Fisher’s exact test, while differences between multiple parametric data sets were determined with Fisher’s least significant difference method. Corrections were made for multiple comparisons. Correlations between parametric data were determined with logistic regression and between nonparametric data with Spearman correlation and Kendall rank method.
RESULTS
Although 3 subjects in each group had palpable effusions prior to the procedure, 6 additional subjects in the ultrasound group were found to have significant effusions after sonographic interrogation (200% increase; p = 0.065). The mean aspirated fluid volume in the palpation group was 5.7 ± 8.1 ml (n = 3) and in the sonographic group was 25.8 ± 24.9 ml (337% increase in fluid volume, n = 9; p = 0.06). Thus, there was a strong trend for sonographic guidance to detect more effusions and permit greater mean fluid aspiration.
Outcome measures are shown in Tables 2 and 3 and Figures 7 and 8. As can be seen from these data, IA corticosteroid injections using anatomic palpation guidance was acceptably effective in relieving pain, resulting in a significant 4.66 ± 2.33 cm reduction in absolute VAS pain scores at 2 weeks (p < 0.001), corresponding to a clinically significant 60.9% ± 30.5% relative reduction from baseline pain (p < 0.001). Moreover, with conventional palpation-guided IA injections, responder rates (defined as percentage reduction in pain scores from baseline ≥ 50%) were high, at 71.6%, while absolute nonresponder rate (defined as reduction in pain scores < 50% at 2 weeks) and significant pain nonresponder rates (significant pain at outcome, defined as absolute VAS pain score ≥ 5 cm at outcome) were low, at 28.4% and 32.4%, respectively. Thus, as reported in the literature, needle guidance by anatomic palpation is acceptably effective for IA corticosteroid injections, with adequate responder rates, reasonably low nonresponder rates, and significant reductions in absolute and relative pain scores at outcome49–51,63–65. These acceptable results with conventional methods are an obvious barrier that sonographic image-guided needle procedures must overcome in order to demonstrate statistical superiority.

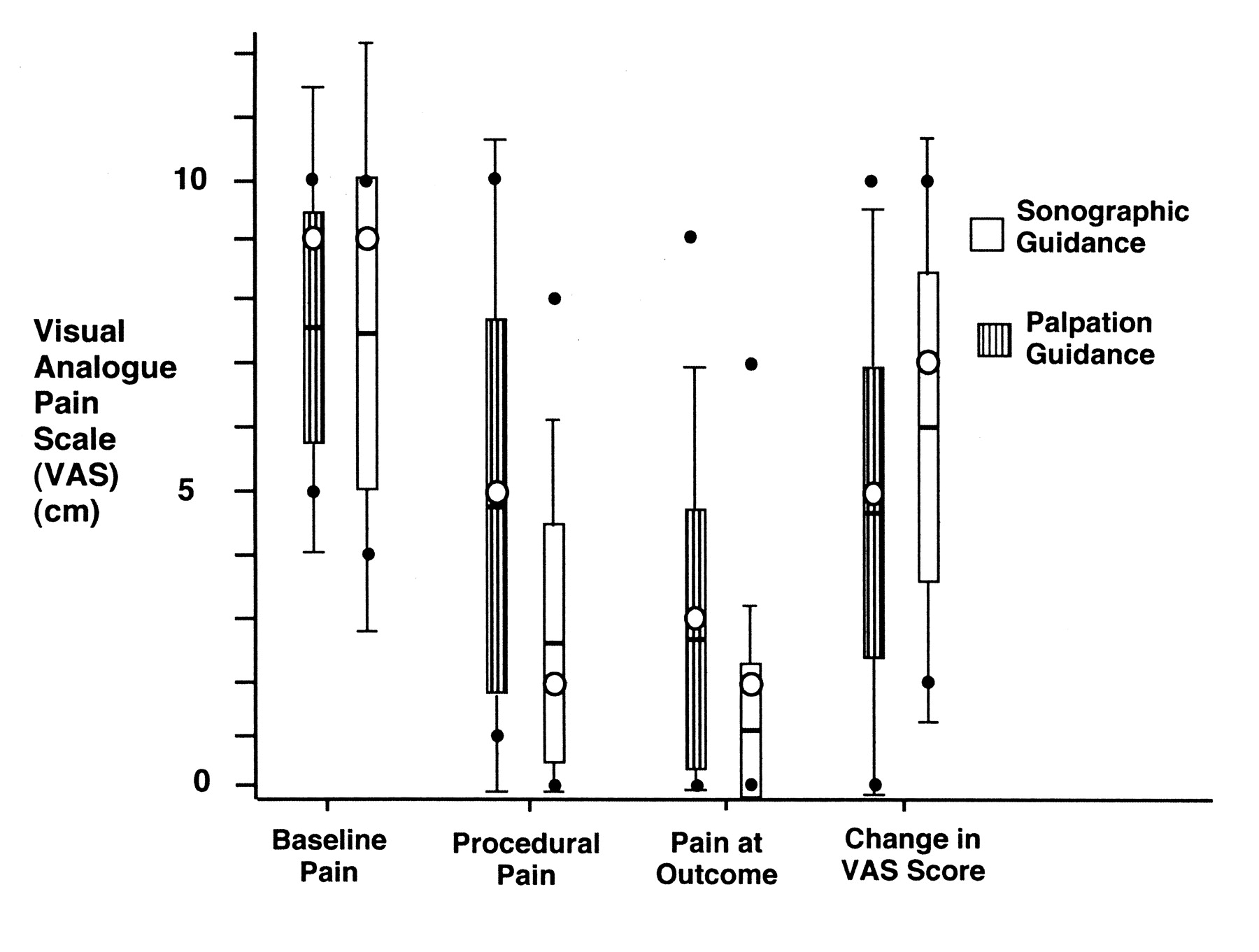
Effect of sonographic guidance on absolute pain scores at outcome. This modified plot shows the effect of sonographic needle guidance on the outcome of intraarticular injections. Bars represent the standard deviation, horizontal line in the bar the mean, the white dot the mode, the brackets the 95% confidence interval, and black dots the range (outliers). Shaded bars indicate conventional palpation-guided injection; white bars indicate sonographic-guided injection with enhanced needle control. Although pain scores at baseline were very similar, sonographic-guided injection with enhanced needle control provided significantly less procedural pain, further reduced pain scores at outcome, and total reduction in pain scores by VAS (all p < 0.01).
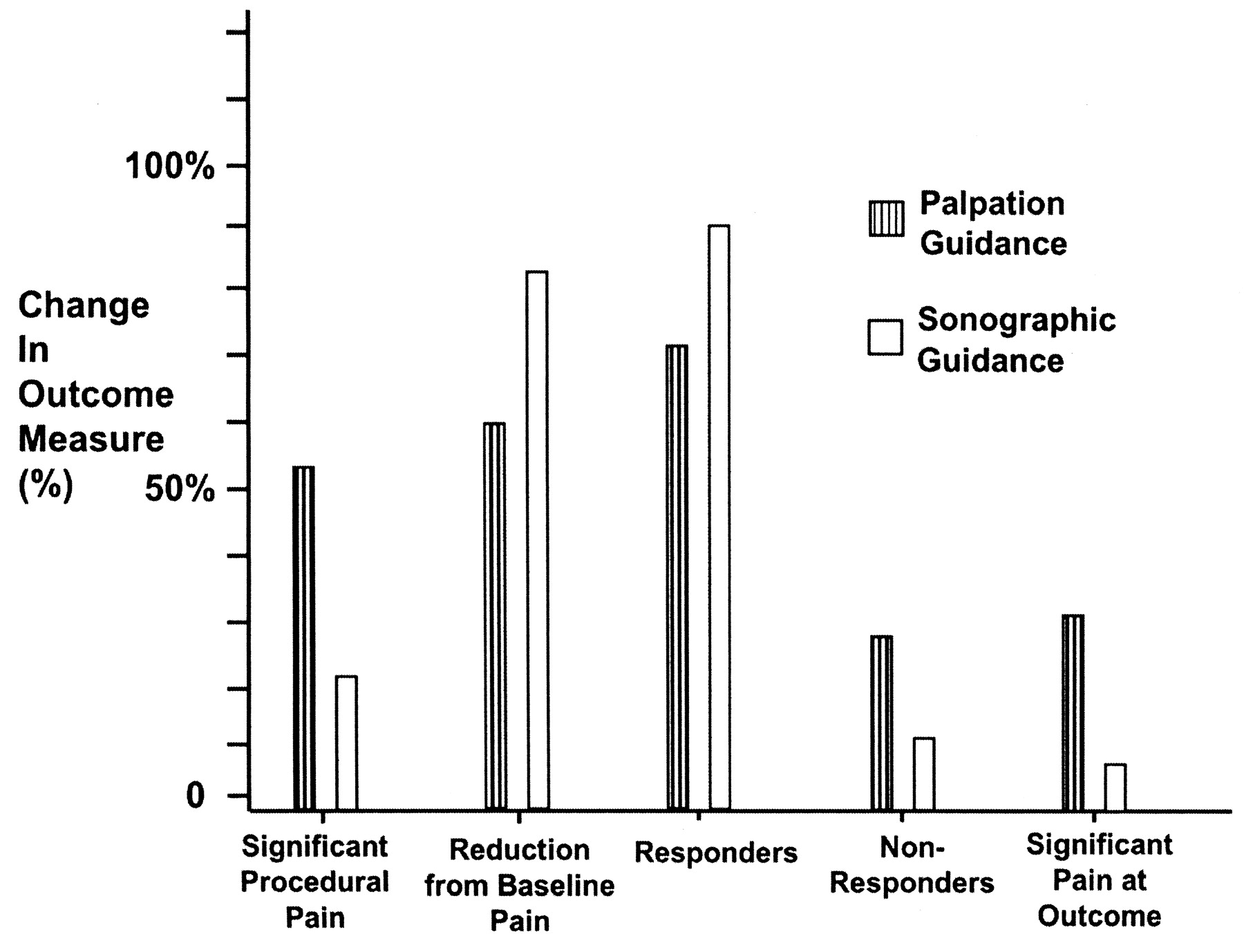
Effect of sonographic guidance on relative changes at outcome. This modified plot shows the effect of sonographic needle guidance on the relative outcome of intraarticular injections. Shaded bars represent relative changes in percentage for conventional palpation-guided injection; white bars represent sonographic-guided injection with enhanced needle control. Although pain scores at baseline were very similar, sonographic-guided injection with enhanced needle control provided significantly lower percentages of significant procedural pain, reduction in pain from baseline, increased percentage of responders (> 50% decrease in pain scores from baseline), significantly reduced percentage of nonresponders (< 50% decrease in pain scores from baseline), and markedly reduced number of subjects with significant pain at outcome (VAS score ≥ 5 cm) (all p < 0.01).
Outcomes by the visual analog pain scale (VAS).
Relative changes in outcomes with sonographic guidance.
Direct comparisons between conventional palpation-guided methods and ultrasound-guided methods are shown in Tables 2 and 3 and Figures 7 and 8. Although baseline VAS pain scores prior to the procedures were statistically similar between the 2 treatment groups (p = 0.422), sonographic image-guided IA injections were significantly less painful than conventional methods, causing 43.6% less absolute procedural pain by VAS pain scores and 59.0% fewer individuals with significant procedural pain (procedural VAS pain score ≥ 5 cm; both p < 0.005). Thus, sonographically directed IA injections are significantly less painful than conventional palpation-directed IA injection procedures.
Therapeutic responses to the 2 injection methods are shown in Tables 2 and 3 and Figures 7 and 8. In all therapeutic measures, sonographically directed procedures were superior to palpation-guided methods: absolute VAS pain scores at 2 weeks were 58.0% lower (p < 0.001), absolute reductions in VAS pain scores were 30.5% greater (p < 0.001), percentage reductions from baseline VAS scores were 36.5% greater (p < 0.001), responder rates were increased by 25.6% (p < 0.035), nonresponder rates were reduced by 62.0% to only 10.1% (p < 0.035), and individuals with significant pain at the 2 week outcome were reduced by 75% to only 8.1% of treated patients (p < 0.001). Thus, although palpation-directed IA steroid injections are acceptably effective at 2 weeks postinjection, routine sonographic image guidance significantly improved outcomes, with further reductions in pain, significantly higher responder rates, and markedly reduced nonresponder rates. The only negative aspect of routine sonographically guided IA injections that was noted in this study was the increase in set-up and procedure time, requiring about 100% more time per procedure (8 scheduled sonographically directed procedures per half-day clinic versus 16 palpation-guided procedures per half-day clinic).
DISCUSSION
Although sonography is increasingly popular among physicians who treat musculoskeletal disease, doubts have remained about the wisdom and scientific justification for using this imaging technology for all IA injections9,10,42–48. Although the momentum for systemic introduction of ultrasound into outpatient musculoskeletal medicine is growing, justifiable skepticism remains among experts who know the scientific literature, are concerned about increased costs, and who are comfortable with the acceptable outcomes achievable by present conventional palpation-guided needle methods48. Because of these concerns, certain experts recommend conventional palpation-guided procedures for routine IA injections, with sonographically guided procedures reserved for nonresponders, difficult anatomy such as the tarsal-metatarsal joints, or deep joints such as the hip, facet joints and sacroiliac joints19,22,23,48. Our results provide some support for this conservative view, as conventional palpation-guided procedures in this study provided acceptable clinical response rates of 71.6%, with reductions in both absolute and relative pain scores (Tables 2 and 3, Figures 7 and 8).
In 1993, Jones, et al studied the accuracy of 109 injections into various joints and found that about one-third of knee and ankle injections were extraarticular, and only half the wrist injections were definitely intraarticular, with even less accuracy reported for shoulder injections12. Subsequent studies have demonstrated similar difficulties in placing the needle accurately, with a 12%–70% failure rate in the subacromial bursa, 58%–75% failure in the glenohumeral joint, 15%–30% failure in the knee, and similar high failure rates in the hip and facet joints10–26. However, inappropriate extraarticular placement frequently resulted in acceptable therapeutic responses, indicating that absolute accuracy of needle placement may not be essential12,23,43,48,49,54–62.
A number of studies support the belief that sonographic guidance provides greater accuracy and improved outcomes for both diagnostic and therapeutic needle procedures14,15,27–38. Balint, et al found that ultrasound improved the overall success of joint fluid aspiration from 32% to 97%20. Similarly, Raza, et al found that ultrasound-guided needle placement resulted in significantly greater accuracy than palpation-guided injection of small joints of the hand27. Kane, et al found that ultrasound was better than clinical examination in determining the presence of knee joint effusions in rheumatoid arthritis5. In an open study of 37 patients, Eustace, et al reported that patients whose injections had been accurately placed improved to a greater degree in the short term than those whose injections had been less accurately placed14. Naredo, et al studied 41 patients who were randomized to receive either a blind or sonographic-guided subacromial injection of depot steroid28. Significantly more improvements in both shoulder function and pain were observed in patients who had received sonographic-guided corticosteroid injection and this was accompanied by greater accuracy of needle placement. Thus, the literature suggests that sonographic guidance improves accuracy and may improve outcome of IA injections, but since palpation-guided injections are also quite effective, the need or justification for sonographic needle guidance does not seem compelling to certain experts12,23,43,48,49,54–62
Considering the results of prior studies and concerns of skeptics, the important question regarding sonographic guidance, therefore, is not whether palpation-guided IA injections are acceptably effective, but whether sonographically-guided IA injections are superior in terms of safety and clinical outcome42,44,47,48. We addressed the routine use of sonographic guidance for all IA injections in the outpatient clinic compared to conventional palpation-guided methods. In this 148-patient study, although conventional palpation-guided methods resulted in acceptable clinical outcomes, sonographically guided IA procedures were significantly superior in all outcome measures, including reduced procedure pain, absolute and relative reduction in VAS pain scores at outcome, increased responder rates, and reduced non-responder rates (Tables 2 and 3, Figures 7 and 8).
One remarkable finding was the significantly and markedly reduced levels of procedural pain (43.6% reduction in VAS pain scores, and 59.0% reduction in significant procedural pain) with sonographically guided IA injections, a benefit of sonographic needle guidance not emphasized in previous reports. Although the causes of this significant beneficial reduction in procedural pain are uncertain, better control and direction of the needle away from pain-sensitive structures during the needle introduction phase into the IA space are the most likely explanations52–57. An alternative explanation is that the cooling effect of ultrasound gel, the pressure from the ultrasound transducer, and the intense sonographic image may have a potent distracting effect on the patient at the neurocognitive level, significantly reducing anxiety and pain, as demonstrated with other distraction techniques66,67. These significant reductions in procedural pain are a benefit of sonographically guided injections that require further research into mechanisms and discussion with the patient.
Sonographic-directed needle procedures are generally considered safer than palpation-guided procedures. However, changes in safety are difficult to address in the setting of relatively safe IA needle procedures without thousands to hundreds of thousands of subjects in each treatment group, as shown in studies of needle safety68. In our study, with only 148 subjects, both palpation-guided and sonographically guided IA injections appeared to be equally safe with no serious complications in either group. However, the study did demonstrate reduced procedural pain, and recent studies have demonstrated that procedural pain during needle procedures is a surrogate measure for direct needle trauma to patient tissues, with better needle control being significantly associated with less IA bleeding, less tissue trauma, reduced pain, and less bruising69.
Typically, an ultrasound-guided procedure increases direct physician and technical costs to third-party payers by $160 to $200 US, and the use of the RPD control syringe also increases costs by $1.50 to $1.95 US per procedure (for comparison, a spinal needle costs $4.00 to $10.00 each). Although sonographically directed procedures were clearly superior in performance and outcome, our study did not address whether these clinical improvements justified the associated increased costs, including acquisition and maintenance of the ultrasound machine, image storage and sonographic supplies, the increased operator set-up and procedure time, and the increased physician and clinic costs to patients and third-party payers. It is also uncertain whether the 25.6% improvement in responder rate and the 62.0% reduction in the nonresponder rate translate into lower heathcare costs, including fewer future clinic visits, repeat procedures, telephone calls to physicians, delayed surgical and reconstructive procedures, less use of oral corticosteroids and pain medications, and fewer serious complications48. Certainly, longer outcome studies with extensive cost-benefit analysis are necessary to determine the true longterm benefit of sonographic guidance for IA procedures.
Our study demonstrates that IA injections performed with sonographic image guidance significantly reduce procedural pain, reduce pain scores at outcome, increase responder rates, and reduce nonresponder rates. The study provides strong support for the use of sonography for IA injections in typical outpatient musculoskeletal practices. Future research is required to address the effects of ultrasound-guided intraarticular procedures on longterm outcomes, functional measures, individual joints, serious complications, and overall healthcare costs.
Footnotes
- Accepted for publication April 28, 2009.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}