

Abstract
Objective. Studies have suggested that early institution of tumor necrosis factor (TNF) inhibitors improves functional status and slows radiographic progression among patients with rheumatoid arthritis (RA). To determine whether these findings have altered practice patterns, we used the Consortium of Rheumatology Researchers of North America (CORRONA) registry to assess the pattern of TNF inhibitor utilization in the US over time.
Methods. Demographics and disease activity data were collected for patients with RA. The trend of TNF inhibitor use during 2002–06 was evaluated prospectively using linear and logistic regression models.
Results. Of the 11,397 patients with RA, 66% and 34% had established RA and early RA (disease duration < 3 yrs), respectively. The majority of patients were female and Caucasian. Despite comparable levels of disease activity, more of the patients with established RA were taking TNF inhibitors than those with early RA (40% vs 25%; p < 0.0001). The majority of patients (70%) taking TNF inhibitors were also receiving disease modifying antirheumatic drugs. The use of TNF inhibitors increased at a rate of 2.8% per year in established RA and 1.2% per year in early RA. The mean Clinical Disease Activity Index at the start of TNF inhibitors decreased at a rate of −0.233 per quarter (p = 0.006), while the mean Disease Activity Score decreased at a rate of −0.04 per quarter (p = 0.022).
Conclusion. Utilization of TNF inhibitors in this multicenter, observational US cohort is increasing in both early and established RA, although it is more prominent among patients with established RA. The level of disease activity at which TNF inhibitors were initiated decreased over time in patients with both established and early RA.
Rheumatoid arthritis (RA) is associated with significant functional disability and erosive joint damage even in the first few years of disease1,2. Combined with an appreciation that therapeutic agents are potentially more effective in patients with earlier disease, there has been a trend towards aggressive therapy with disease modifying antirheumatic drugs (DMARD) and biologic agents, particularly tumor necrosis factor (TNF) inhibitors.
Several recent studies, including a number focusing on early RA, have suggested that early institution of TNF inhibitors can improve functional status and slow radiographic progression. The extent of this response among patients with early RA may even be greater, compared to those patients with more established disease3–7. Therefore, the use of more aggressive therapeutic strategies with TNF inhibitors, either in addition to or in lieu of existing DMARD, has been recommended in patients with early RA with poor prognostic factors. However, issues such as cost and safety may affect the choice of first-line therapy in early RA. A recent online survey found that many rheumatologists waited until patients have failed at least 2 DMARD before using biological agents8.
Using data from the Consortium of Rheumatology Researchers of North America (CORRONA) registry, we sought to determine if the pattern of TNF inhibitor utilization among patients with early and established RA has changed over a 5-year period (2002 to 2006) in a large US cohort. We hypothesized that the use of TNF inhibitors has increased over time for patients with both early and established RA.
MATERIALS AND METHODS
The CORRONA registry is an independent registry of patients primarily with the diagnosis of RA and psoriatic arthritis. It was founded in 2000 and began data collection in 2002. As of September 1, 2006, 11,190 patients with RA were enrolled in the database from 76 sites across 23 states in the USA. Over 80% of the initial physicians continued to enroll patients over the studied 5-year period. Similar to many published data, established RA was defined as RA diagnosis > 3 years and early RA as RA diagnosis ≤ 3 years.
Demographic information including age, race, sex, and the highest level of education completed was obtained. Data on RA disease characteristics such as the duration of RA, medications for RA, the presence or the absence of rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibody were also collected. Disease activity was measured using 3 physician-reported measures — tender joint count (TJC), swollen joint count (SJC), and physician global assessment; 2 laboratory tests of the acute-phase response — erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP); and 3 self-reported patient measures — one for functional disability measured using the modified Health Assessment Questionnaire (mHAQ), visual analog scale (VAS) for pain, and VAS for patient global assessment of arthritis. In addition, the level of disease activity was measured using the Disease Activity Score using 28 joints (DAS28) and Clinical Disease Activity Index (CDAI). While both the DAS28 and CDAI incorporate TJC, SJC, and patient and physician (in CDAI) global assessment of function, the DAS28 also incorporates a laboratory marker of inflammation, ESR.
The percentage of patients receiving TNF inhibitors was calculated for patients with both established and early RA. In order to look for time trends in the use of TNF inhibitors, patients were subdivided into separate time periods according to their year of enrollment. Early RA patient enrollment annually was 403 in 2002, 923 in 2003, 913 in 2004, 1103 in 2005, and 435 in 2006. The rate of actual and predicted TNF inhibitor use was analyzed quarterly to evaluate the pattern of TNF inhibitor use. Each year of enrollment was also analyzed for disease activity (DAS28 and CDAI) as a function of TNF inhibitor use. The pattern of TNF inhibitor utilization in combination with methotrexate (MTX) and other DMARD was also evaluated in a subgroup analysis for both early and established RA.
Statistical methods
The demographic and clinical characteristic information for patients with early and established RA were compared using the 2-sample t-test. One-way analysis of variance model (ANOVA) was used to evaluate the trend of clinical characteristics over time. The model was adjusted for age, sex, and race. To assess the trend of TNF inhibitor use over time, we used a linear regression model with percentage of patients using TNF inhibitors in the quarter as the dependent variable and a continuous quarter number as the independent variable. We fitted a linear regression using actual percentage of TNF inhibitor use (as information given by the physician) or CDAI as the dependent variable, and quarter number (e.g., 1 = q1/02, 2 = q2/02, 3 = q3/02) as a continuous independent variable. A straight-line estimation of dependent variables was then obtained from this linear regression. The best fitted lines for TNF inhibitor use, CDAI, or DAS28 were the projected values on the regression lines at specific timepoints. All statistical analyses were performed using Stata 7.0 (StataCorp LP, College Station, TX, USA).
RESULTS
Patient characteristics
Patient demographics and clinical characteristics for all early and established RA are described in Table 1. The majority of patients were female (74%) with established RA (66.3%). Data on disease duration were unavailable for 155 patients (1.4%) and they were excluded from this analysis. The racial/ethnic composition of the population was similar in both groups, with 85.4% Caucasians, 6.5% Hispanics, 4.5% African Americans, and 1.5% Asians. Patients with RA taking TNF inhibitors were slightly younger and more educated compared to patients with RA overall (Table 2).
Patient demographics of all established and early RA.
Patient demographics of established and early RA taking TNF inhibitors.
The clinical characteristics were similar in patients with both early and established RA taking TNF inhibitors, except for a slightly worse physician global assessment of arthritis among those with early RA (29.6 vs 27.7; p = 0.02). Patients with RA enrolled in the CORRONA registry, regardless of their disease duration and TNF inhibitor therapy, had moderately active disease, with a mean DAS28 score of 3.7 to 3.8. Over the past several years, the overall level of disease activity among patients with early RA improved slightly, from a mean DAS28 of 4.09 ± 1.58 in 2002 to 3.73 ± 1.50 in 2006.
Patterns of TNF inhibitor utilization
In the CORRONA registry, approximately one-third of all patients with RA were receiving TNF inhibitors. Despite similar levels of disease activity, a greater proportion of patients with established RA were taking TNF inhibitors compared to patients with early RA (40% vs 25%; p < 0.0001). Among patients with both early and established RA, the majority (70%) of those taking TNF inhibitors were also taking concomitant DMARD, with MTX being the most commonly used DMARD. Concomitant MTX use was slightly greater among patients with established RA than in those with early disease (55% established vs 48% early). Only 30% of all patients with RA taking TNF inhibitors were receiving TNF inhibitor monotherapy.
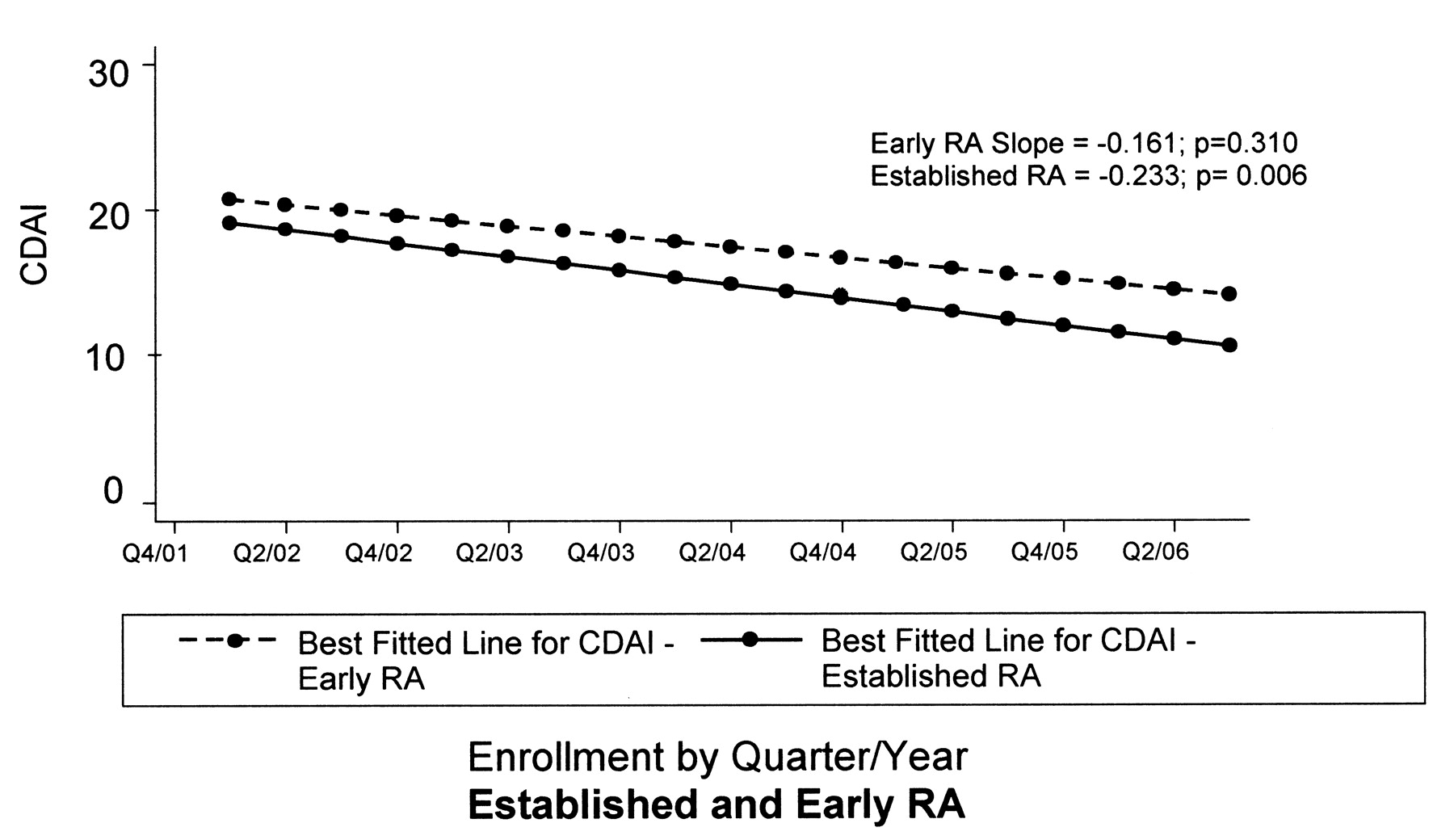
In recent years, the use of TNF inhibitors has increased in patients with both established and early RA, although it was more prominent among patients with established RA (Figure 1). The use of TNF inhibitors increased at a rate of 2.8% per year (0.7% per quarter) for patients with established RA and 1.2% per year (0.3% per quarter) for early RA. Interestingly, the level of disease activity at which TNF inhibitors were initiated decreased over time in patients with both established and early RA (Figure 2 and 3). Among patients with established RA, the mean CDAI at the start of TNF inhibitor initiation decreased from 22.4 in 2002 to 9.5 in 2006 at a rate of −0.233 per quarter (p = 0.006), while the mean DAS28 decreased from 4.7 to 2.9 at a rate of −0.04 per quarter (p = 0.022). Similar findings were noted for patients with early RA, with TNF inhibitors being initiated at a lower disease activity level. The mean DAS28 at the start of TNF inhibitor initiation decreased from 5.7 in 2002 to 4.0 in 2006 at a rate of −0.06 per quarter (p = 0.027).

Pattern of TNF inhibitor use: established RA vs early RA.

Best fitted line for Clinical Disease Activity Index (CDAI) score at the time of TNF inhibitor initiation in established and early RA.
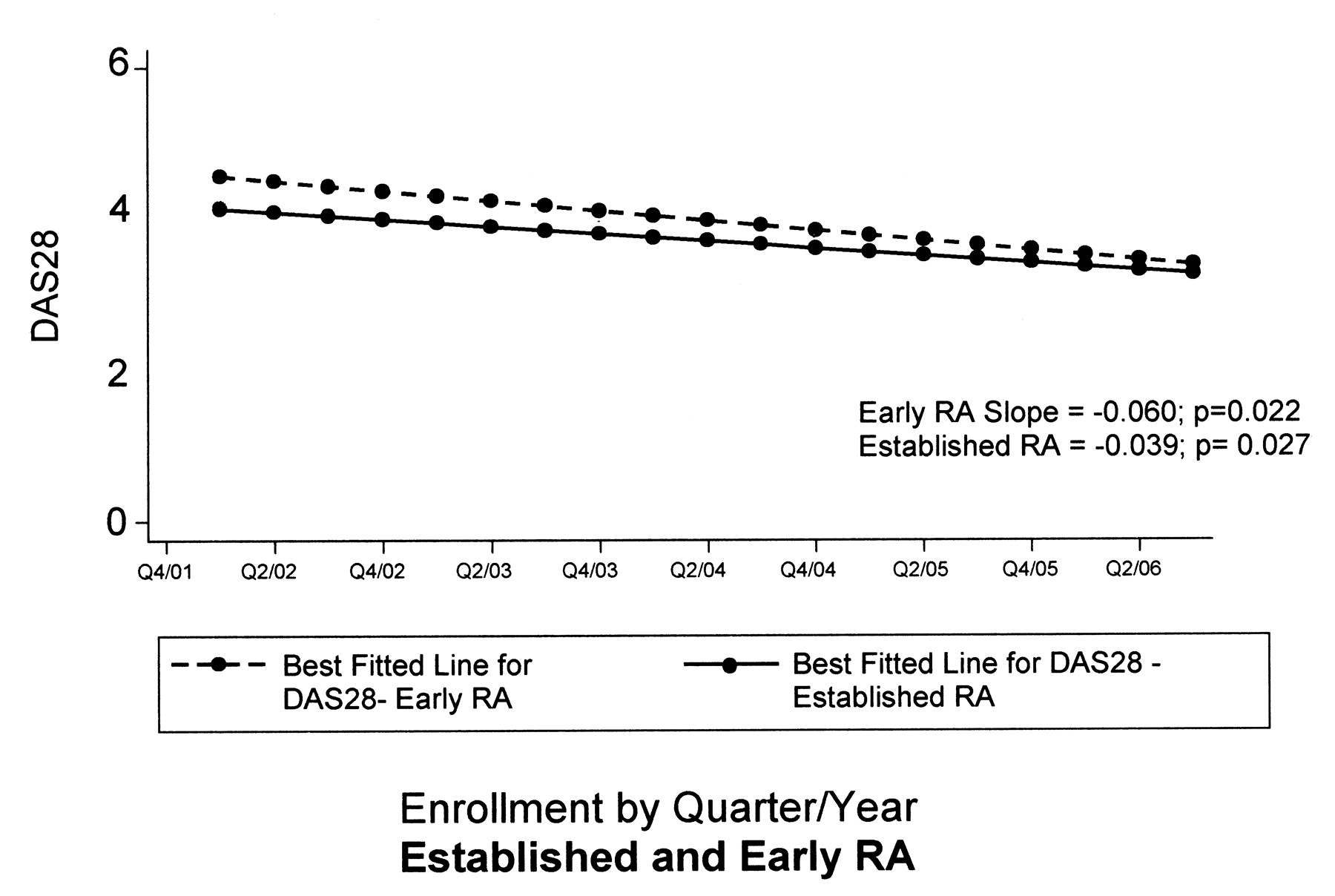
Best fitted line for the 28-joint Disease Activity Score (DAS28) at the time of TNF inhibitor initiation in established and early RA.
DISCUSSION
In light of recent data supporting an earlier use of TNF inhibitors in patients with RA, we analyzed the CORRONA registry to assess if the pattern of TNF inhibitor utilization has changed over time, especially among those with early RA. Our results showed that approximately one-third of all patients with RA were taking TNF inhibitors, with a greater use among patients with established RA (40%) compared to those with early RA (25%). The majority of patients (70%) receiving TNF inhibitors were on combination therapy with DMARD, most commonly with MTX. While the use of TNF inhibitors did appear to be increasing for the treatment of RA from 2002 to 2006, this trend was more prominent among patients with established RA. This suggests that, despite using TNF inhibitors for about one-third of patients, with a small recent upward trend, participating rheumatologists in the CORRONA US registry have not yet widely adopted TNF inhibitor therapy for early RA. Further, these data do not suggest that an alteration in the treatment paradigm, such that TNF inhibitor use is becoming first-line therapy, has occurred to date. As has become common practice, our study shows that the majority of patients with both early and established RA receiving TNF inhibitors were taking combination therapy with DMARD. This suggests that even in early RA, TNF inhibitors are typically being added onto preexisting DMARD rather than being initiated as first-line therapy. However, the overall threshold to initiate TNF inhibitors appears to be lowering, with RA patients being started on TNF inhibitors at an overall lower disease activity level than in the past. With recent publication of the American College of Rheumatology 2008 recommendations and guidelines for the use of biological agents in RA, the treatment paradigm may shift towards an increased and earlier use of TNF inhibitors over the next several years9.
Several other factors such as race, education, and socioeconomic status may also contribute to this pattern of treatment utilization and need to be explored further10–14. Nonetheless, our study suggests that although TNF inhibitors may not be the first line of therapy, they are being used more aggressively than in the past at a lower level of disease activity in hopes of potentially slowing the disease progression. We believe that this is the first time that this has been shown. In addition, the rates of TNF inhibitor utilization are significantly different from those reported in several European registries, in which 8% and 12%–15% of patients with RA are receiving TNF inhibitors15.
Since their introduction, biologic agents have significantly increased available therapeutic options and substantially improved disease outcomes for patients with RA. Until recently, most studies demonstrating the efficacy of TNF inhibitors have been in patients with established RA. However, several recent studies have assessed the utility of these agents in patients with earlier disease. Treatment of patients with early RA with TNF inhibitors has shown equivalent or superior results compared to more established RA in terms of improved signs and symptoms, inhibition of structural damage, and enhanced functional status4,16–19. Because patients with early RA will have less irreversible damage from RA, it has been suggested that TNF inhibitors may have a greater clinical and radiographic effect in such patients. This, along with the potential ability to withdraw therapy in a subset of patients, has led to the concept of a “window of opportunity” in the treatment of early RA with the goal of inducing remission20–22. Indeed, recent data suggest that for a subset of patients with early RA, institution of therapy with TNF inhibitors combined with MTX can achieve a very high level of response, with the potential for withdrawal of TNF inhibitor therapy for a number of patients21. However, a number of factors, including cost, longterm safety considerations, and perhaps individual clinician experience, may affect treatment paradigms23–25. To date, such considerations may have limited the widespread use of TNF inhibitors as the first line of therapy in early RA, despite the promising published data.
There are several limitations to our study. The CORRONA registry is a longitudinal observational database. As is true of any such registry, data may be less complete than data obtained from controlled clinical trials. In addition, we chose to define early RA as those patients with a diagnosis of RA for less than 3 years. While currently there is no universal consensus on a definition of “early” RA, many would consider 3 years to be too long a disease duration to be called “early.” However, given the evolving considerations in RA, we felt it to be a useful landmark from a treatment standpoint to track changes in the pattern of TNF inhibitor use. Despite a large number of patients with RA, both early and established, in the CORRONA registry, a relatively smaller number of early RA patients taking TNF inhibitors at this time limits our ability to perform stratified analysis based on their prior nonbiological and biological DMARD therapy. Finally, it is possible that a trend in early adoption of TNF inhibitors is occurring only at present, or may occur in the near future. Many important medical break-throughs do not achieve instant uptake throughout the community. Thus, it will be important to continue this analysis.
Our study shows substantial use of TNF inhibitors in the RA population in general and a trend towards increasing use from 2002 to 2006. While there was not a marked recent trend in treating early RA more aggressively, a quarter of patients with early RA are being treated with TNF inhibitors and the trend shows an increase. Further, in this large cross-sectional analysis over time of private and academic sites in 23 states within the US, we have documented that the overall utilization of TNF inhibitors is substantially different from that reported in registries from several European countries15. Moreover, the overall level of disease activity at the initiation of TNF inhibitors among patients in the CORRONA registry is significantly lower than in certain European countries. For example, in the UK, a DAS of 5.1 is required in order to be eligible to receive TNF inhibitors15. With fewer restrictions related to the level of disease activity (e.g., DAS28) in the US, our observed trend for prescribing of TNF inhibitors at lower level of disease activity would not be expected to be found in countries where minimal disease activity measures for TNF inhibitor eligibility are required. It would therefore not be possible to demonstrate a “migration” of treatment trends for greater utilization in these systems unless more patients became eligible for treatment by virtue of more active disease. Fewer prescription restrictions and greater drug availability in the US provide a unique opportunity to study the practice patterns of TNF inhibitor use in a “real world” setting. We expect our findings to be varied from European registries and believe that large US cohorts, as represented in the CORRONA registry, are uniquely positioned to demonstrate evolutionary trends in TNF inhibitor utilization.
Footnotes
-
Sources of support: Dr. Lee, Centocor; Dr. Yazici, BMS, Centocor, Roche, Wyeth; Dr. Greenberg, Arthritis Foundation, BMS, Centocor, CORRONA, NIAMS, NIH, Roche, UCB; Dr. Kremer, Abbott, Amgen, BMS, Centocor, Genentech, Roche; Dr. Kavanaugh, Abbott, Amgen, Biogen-Idec, BMS, Centocor, Genentech.
- Accepted for publication January 15, 2009.








{kind=link}
{kind=link}
{kind=link}