

We describe a case of retropharyngeal calcific tendinitis, an uncommon benign condition that was first described by Hartley in 19641.
A 37-year-old woman presented with a 3-day history of right occipital neck pain and odynophagia. There was no associated fever or recent illness. She denied any trauma or history of injury to the neck area. Ear-nose-throat and neck examinations were normal apart from limited neck motion with right occipital tenderness but no lymphadenopathy. Laboratory studies including white blood cell count, erythrocyte sedimentation rate, and C-reactive protein were normal. Magnetic resonance imaging of the cervical spine was performed. T2-weighted image showed an area of high signal intensity extending from C1 to C5 consistent with prevertebral edema (Figure 1, arrow), and a hypointense area anterior to C1–C2 consistent with calcification (Figure 1, arrowhead). A diagnosis of retropharyngeal calcific tendinitis was made, and the patient was treated with a nonsteroidal antiinflammatory medication. Her symptoms resolved completely in 6 days.
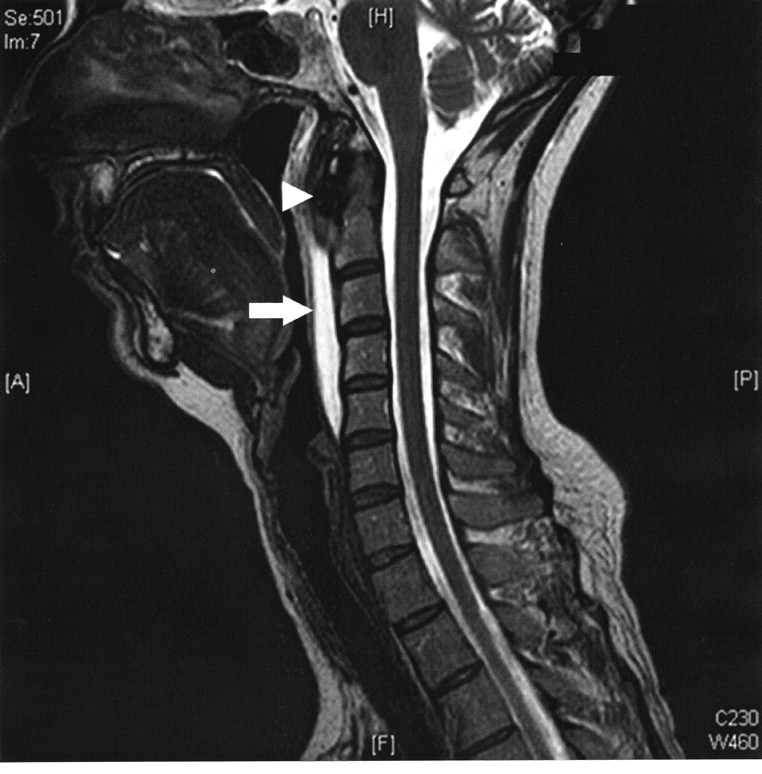
T2-weighted image showing an area of high signal intensity extending from C1 to C5 consistent with prevertebral edema (arrow) and a hypointense area anterior to C1–C2 consistent with calcification (arrowhead).
Retropharyngeal calcific tendinitis1 is an uncommon benign condition caused by an aseptic inflammatory process in the superior oblique tendon fibers of the longus colli muscle, triggered by deposition of calcium hydroxyapatite crystals2. The pathogenesis of crystal deposition in these fibers remains unclear, although repetitive trauma, ischemia, necrosis, and genetic predisposition have been suggested as possible etiologies3. The most common symptoms are neck pain, neck rigidity, dysphagia, odynophagia, and headache. Laboratory data are usually normal, but inflammatory changes may be observed with elevated erythrocyte sedimentation rate and mildly elevated white blood cells4. The pathognomonic radiographic findings consist of prevertebral soft tissue swelling typically extending from C1 to C4 and calcification anterior to C1–C2 at the insertion of the superior oblique tendon of the longus colli muscle1,2,4,5,. Symptoms usually resolve over the course of 1 to 2 weeks treated conservatively with nonsteroidal antiinflammatory medications and avoidance of aggravating neck movements.








{kind=link}