

Abstract
Objective. Using high resolution computed tomography (HRCT), to assess the lung involvement outcome after autologous hematopoietic stem cell transplant (AHSCT) in patients with scleroderma (systemic sclerosis, SSc).
Methods. HCRT scans prospectively performed before (n = 9 patients) and after (n = 47) AHSCT were blindly reviewed by 2 independent investigators using the Wells score.
Results. After a median 60 months’ followup, the overall disease extent score from HCRT scans decreased from 10 (0–45) to 4 (0–36) (p = 0.04) 6 months after AHSCT, and thereafter increased up to 36 months and stabilized; the modified Rodnan skin score fell (p < 0.05).
Conclusion. The extent of SSc lung involvement on HRCT rapidly but transiently regressed after AHSCT.
- SYSTEMIC SCLEROSIS
- AUTOLOGOUS HEMATOPOIETIC STEM CELL TRANSPLANT
- LUNG INVOLVEMENT
- FIBROSING ALVEOLITIS
- HIGH RESOLUTION COMPUTED TOMOGRAPHY CHEST SCAN
Pulmonary fibrosis (PF) occurring in 50% to 80% of patients with systemic sclerosis (SSc) is their leading cause of death1–3. In this context, cyclophosphamide (CYC) was shown to significantly improve patient’s functional status, skin score, and, albeit modestly, lung function4. In the past 10 years, several phase I–II studies5–8 used high doses of CYC followed by autologous hematopoietic peripheral stem cell transplant (AHSCT)6. The studies showed complete or partial remission with stable vital capacity (VC) and diffusing capacity for carbon monoxide (DLCO) on lung function tests up to 5 years after AHSCT in two-thirds of the patients treated for severe diffuse SSc. High resolution computed tomography (HRCT) of the chest is the most sensitive and reproducible method to analyze PF associated with SSc (PF-SSc)1,3, but presently no data are available on HRCT after AHSCT. We designed this study with a special focus on HRCT analysis of PF-SSC in a subgroup of patients included in a single-institution pilot study as reported5 for whom longterm followup evaluation was available after AHSCT.
MATERIALS AND METHODS
Fifty-six HCRT scans (using sequential acquisition of 1-mm scans, spaced at 10 mm, intervals extending from the lung apices to below the costophrenic angles) were prospectively performed in 9 patients with SSc fulfilling the American College of Rheumatology preliminary diagnosis criteria, before (n = 9) and after (n = 47) AHSCT. All patients with diffuse cutaneous and severe SSc plus early visceral involvement treated by AHSCT as published5 and with at least 1 year followup after AHSCT were analyzed. Before AHSCT and quarterly thereafter, repeated evaluations during followup included: (1) skin involvement using the modified Rodnan skin score (mRSS); (2) lung function and involvement using the New York Heart Association (NYHA) functional class, pulmonary function tests, and HRCT scans.
Two independent investigators (CDB and DL) blindly and randomly reviewed each HRCT using the Wells score1. HRCT were reviewed at 5 levels1. To quantify the extent and the severity of CT patterns at each level, we analyzed (A) the disease extent of interstitial lung involvement, including both reticular pattern and ground-glass opacification, and (B) the coarseness of fibrosis as follows: 0, ground-glass opacification alone; 1, fine intralobular fibrosis; 2, microcystic reticular pattern comprising air spaces ≤ 4 mm in diameter; and 3, a macrocystic reticular pattern comprising air spaces > 4 mm in diameter. This analysis allowed us to compute the overall (1) mean value of disease extent by averaging the measures obtained at each level; (2) proportion of ground-glass opacification; and (3) coarseness score for each patient, derived by summing the coarseness scores (0–3) at 5 levels (minimum score, 0; maximum score, 15). Then, on the whole HRCT, the overall grade of interstitial lung disease was evaluated according to the Wells score1.
Statistical analysis
Categorical variables were summarized as counts and percentage, while numerical variables were summarized as median and full range. Groups were compared using Fisher’s exact test for the categorical variables and nonparametric paired signed-rank test for numerical variables.
RESULTS
The baseline characteristics of the patients, aged 41 years (range 16–61), with clinical, functional, and HRCT development before and after AHSCT are given in Tables 1 and 2. All but 2 patients had chest skin involvement at baseline. During the 60 months (range 18–24) of followup after AHSCT, 1 death from disease progression including skin and lung progression occurred at 18 months and another from relapse after prior major response5, with septic shock originating from skin lesions at 24 months. Neither was treatment-related. A continuous and significant decrease in mRSS (p < 0.05) was observed. NYHA functional status remained stable with most patients sustained in class I/II. VC tended to be higher 24 months after than before AHSCT [83% (62–111%) vs 72% (37–108%), respectively; p = 0.078]. The same comparison including only the 7 patients alive at 60 months yielded similar results (data not shown). HRCT pattern analysis showed a significant fall in the mean overall disease extent 6 months after AHSCT [4 (0–36) vs 10 (0–45); p = 0.04], with further increase up to 36 months and stabilization thereafter (Figure 1). Notably, at 6 months compared to baseline, the overall disease improved in 5 and remained stable in 1 out of the 6 patients with baseline PF-SSc, while it remained stable in the 3 others. To further confirm that disease extent improved at 6 months and worsened at 1 year, it was recoded as: 1 if lowered, 2 if stable, and 3 if increased when compared to previous CT scan. Using the nonparametric paired signed-rank test, difference was significant between 6 months and 1 year (p = 0.03), confirming that disease extent improved at 6 months and worsened thereafter. Figure 1 shows individual development of the overall disease extent score. The overall coarseness remained stable and the overall proportion of ground-glass opacification decreased after AHSCT, but not significantly.
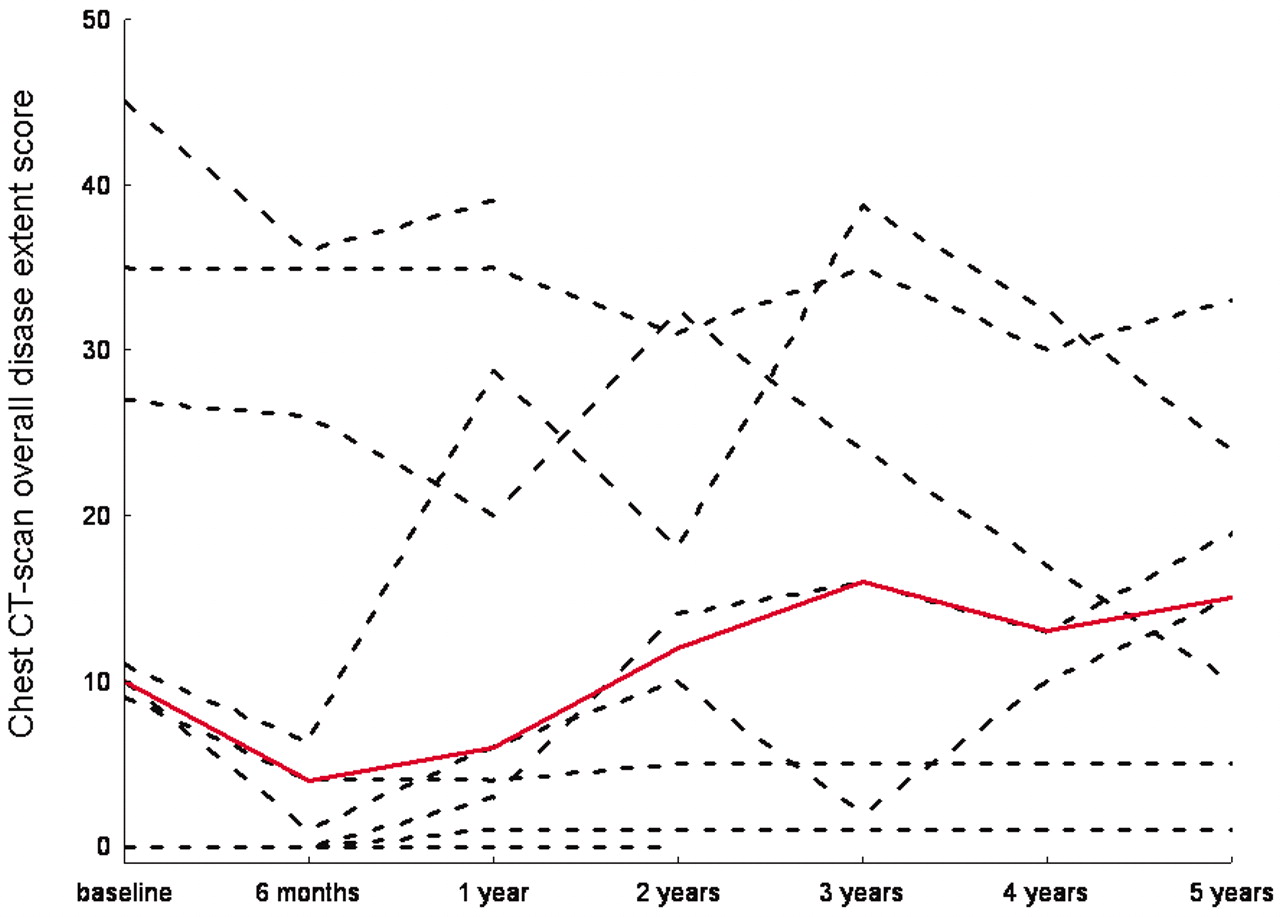
Progression of the individual overall disease extent scores on HRCT scans of the chest. Red line represents the median value.
Baseline clinical and serologic characteristics of the patients with SSc (n = 9) treated by autologous hematopoietic stem cell transplant according to the ISAMAIR protocol5 and followed at least 1 year after transplant with repeated CT scans.
Outcome of clinical characteristics, pulmonary function tests, and CT scan patterns after autologous hematopoietic stem cell transplant. Results are given as median (range).
DISCUSSION
Reports from several European5–7 and North American8 studies have shown promising results in patients with severe diffuse SSc treated by AHSCT with significant, rapid, and durable fall in skin score, improved functional status, and stable lung function. However, none has yet analyzed the progression of HRCT pattern outcome after AHSCT using a validated methodology1.
The main finding of our pilot study of a small number of highly selected patients was to document a significant and rapid fall in the overall extent of PF-SSc on HRCT 6 months after AHSCT using the Wells score1. Five of the 6 patients with evidence of PF-SSc before AHSCT experienced improvement of PF-SSc on HRCT as soon as 6 months after AHSCT. Moreover, 4 of these 6 patients had high grade 2 or 3 lesions on HRCT. Such results are important since, to our knowledge, no other study has shown the same rapid response in such a proportion of patients with severe SSc after 6 months of CYC therapy9,10. All these data support the observation that AHSCT that includes high dose of CYC can rapidly reverse ground-glass opacification and decrease the extent of PF-SSc on CT scan even in SSc patients with severe disease. It is interesting that after an initial improvement, the overall extent of disease on serial HRCT increased again in some patients and was back to the pre-transplant extent 24 months after AHSCT, and then was relatively stable up to 60 months of followup. These results may illustrate the attenuation with time of the effect of CYC11 and a new increase in PF-SSc contrasted with a persistently improved skin score. Our study provides no new insight into this unexpected finding. Indeed, there is a possible uncoupling between skin and lung involvement in SSc, as patients with limited cutaneous SSc can have severe interstitial lung disease. Moreover, in the Scleroderma Lung Study, there was also a relapse in interstitial lung disease after 18 months, whereas the skin score stabilized11.
Our study confirmed that AHSCT induced a rapid and significant regression of skin fibrosis, as assessed by mRSS. It showed rather stable lung function after AHSCT and even pointed out a trend towards improved lung volumes at 24 months. The stability of lung volumes and of DLCO after AHSCT has to be seen as a good result in these patients with severe diffuse SSc. Indeed, Wells, et al recently pointed out that the attainment of complete stability in PF-SSc with treatment should not be underestimated12.
A significant and rapid decrease of the extent of PF-SSc was observed on HRCT scans in patients treated for severe diffuse SSc 6 months after AHSCT. Longer-term followup showed that the impressive early treatment effects of AHSCT on the extent of PF-SSc decreased over time and were transient in some patients, which again raised questions about the need for maintenance immunosuppression after AHSCT. These results will have to be confirmed in larger numbers of patients, as intended in the ongoing European (ASTIS; www.astistrial.com) and North American (SCOT; www.sclerodermatrial.org) studies comparing AHSCT to monthly intravenous CYC therapy.
Footnotes
- Accepted for publication February 11, 2009.








{kind=link}