

Abstract
Objective. To prospectively examine neuropsychiatric (NP) events and their association with health related quality of life (HRQOL) over time in patients with systemic lupus erythematosus (SLE).
Methods. In an observational cohort study from a single academic center, NP events and their attribution were identified at enrollment and at annual assessments for up to 7 years. NP events were characterized using the American College of Rheumatology case definitions; other variables were global SLE disease activity and cumulative organ damage. The outcomes of NP events were recorded and self-report HRQOL was measured with the mental (MCS) and physical (PCS) component summary scores of the Medical Outcomes Study Short Form-36.
Results. There were 209 patients, 88% female and 92% Caucasian, with a mean (standard deviation) age of 43.7 (13.8) years. Followup was available in 175/209 (84%) patients. There were 299 NP events in 132/209 (63%) patients over a mean followup of 3.6 (2.5) years. Thirty-one percent of NP events in 54 patients were attributed to SLE. Multivariate analysis indicated lower MCS scores in patients with NP events compared to those without events (p < 0.001) regardless of attribution. The group means for PCS scores were significantly lower in patients with NP events (p < 0.001) regardless of attribution. There was no association between HRQOL and cumulative organ damage, nor between NP events and the progression of organ damage.
Conclusion. The association of lower HRQOL with NP events over time, which is independent of progression in cumulative organ damage, emphasizes the persistent negative effect of NP events in the lives of patients with SLE.
Nervous system disease, characterized by a variety of neuropsychiatric (NP) manifestations, is frequent in patients with systemic lupus erythematosus (SLE). The NP events include common clinical conditions such as headache, mood disorders and cognitive complaints, to less frequent entities such as seizures, psychosis, and myelopathy1–6.
Most clinical studies of NPSLE have been cross-sectional in design and there is a relative paucity of information on the longterm outcome of NP events and their clinical effect on patients with SLE. Further, many longitudinal studies have focused upon a specific subset of NPSLE such as cognitive dysfunction7–11, in lieu of a more comprehensive assessment encompassing all NP manifestations12,13. The adverse clinical effect of NP events in patients with SLE has been demonstrated in cross-sectional studies using a variety of outcomes such as the association with patient self-report health related quality of life (HRQOL)3,4, employment history14, disability15, and mortality16,17. However, given the potential for improvement or worsening of NP disease in SLE it is important to examine changes in NP status and its clinical significance over time. Thus, our objective was to prospectively examine the longterm outcome and effect on HRQOL of all NP events, attributed systematically to SLE or non-SLE causes, in patients who were followed at our center for up to 7 years.
MATERIALS AND METHODS
Patients
Consecutive patients attending the Dalhousie University Lupus Clinic at the Queen Elizabeth II Health Sciences Center, Halifax, Nova Scotia, were enrolled in our study between June 2000 and December 2007. The Clinic receives referrals from primary care physicians, general internists, rheumatologists, and other subspecialties such as nephrology, dermatology, and hematology in a referral base of approximately 1 million people and is the only designated lupus clinic in the region. All patients fulfilled the American College of Rheumatology (ACR) criteria for SLE18, and the date of diagnosis of SLE was the time when a patient first fulfilled the ACR criteria as determined by a rheumatologist. The study protocol was approved by the local institutional research ethics committee (Capital Health Research Ethics Board).
Study assessments
Patients were evaluated upon enrollment into the lupus cohort and whenever possible annually thereafter. Data acquisition included a medical history and examination including neurological, psychiatric, neuropsychological and neuroimaging assessments when indicated, completion of standardized instruments for the quantification of disease activity, cumulative organ damage and quality of life, and review of the patient’s medical record. Peripheral blood was collected for the assessment of hematological, biochemical, and serologic variables related to the assessment of SLE. These included a complete blood count, serum creatinine, urinalysis and 24 h urinary protein (if indicated), antinuclear antibody, anti-dsDNA antibody, and serum C3 and C4 levels. Global disease activity was quantified by the SLE Disease Activity Index (SLEDAI)19 and cumulative organ damage by the Systemic Lupus International Collaborating Clinics (SLICC)/ACR Damage Index (SDI)20. HRQOL was measured by patient-generated mental (MCS) and physical (PCS) component summary scores of the Medical Outcomes Study Short Form-36 (SF-36)21.
NP disease
Specific NP events were characterized using the ACR nomenclature and case definitions for 19 NP syndromes22 described in SLE. In all patients a comprehensive set of questions was used to help screen for the occurrence of any of the 19 NP syndromes. Specific investigations for NP disease were done, not routinely on all patients but only if indicated following clinical assessment. The occurrence of prior NP events was confirmed by review of the medical record. Patients could have more than 1 type of NP event, but repeated episodes of the same event occurring between assessments were recorded only once.
Attribution of NP events
Decision rules were used to determine the attribution of NP events. Factors that were taken into account included: (1) onset of NP event(s) prior to the diagnosis of SLE; (2) presence of concurrent non-SLE factor(s) that were identified within the glossary for the ACR definitions for each NP syndrome and considered to be a likely cause or significant contributor to the event; and (3) occurrence of “minor” NP events as defined by Ainiala, et al, who have reported a high frequency of such events in normal population controls1. These include all headaches, anxiety, mild depression (i.e., all mood disorders that fail to meet the criteria for “major depressive-like episodes”), mild cognitive impairment (deficits in fewer than 3 of the 8 specified cognitive domains), and polyneuropathy without electrophysiological confirmation. Thus, if a NP event occurred around the time of diagnosis of SLE (usually not more than 6 months prior) or at any time following the diagnosis of SLE, and if no other etiology as listed in the ACR glossary for that NP syndrome could be identified, and if the NP event was not 1 of those identified by Ainiala, et al1, then it was attributed to SLE. Conversely, if the NP event preceded the diagnosis of SLE by a considerable period of time (usually more than 6 months) or if an alternative etiology was identified, or the NP event was one identified by Ainiala, et al, then the NP event was attributed to “non-SLE” factors. In keeping with the ACR case definitions22 it was recognized that in some cases both SLE and non-SLE factors contributed to the etiology of NP events.
Prospective evaluation of NP events
All NP events were identified upon enrollment into the cohort and attributed to SLE or non-SLE causes. Patients were reviewed on an annual basis as per study protocol. At followup assessments, the occurrence of new NP events since the previous study visit and their attribution was determined. In addition, previous NP events were recorded as ongoing or resolved. Any NP event that had been recorded as resolved at a prior assessment, but reemerged, was deemed a recurrence. Thus at each assessment the status of NP events could be classified as NP-positive (new, recurrence, or ongoing) or NP-negative (resolved or no event). Resolution was taken as the dominant status for NP events when they occurred and resolved since the previous study visit. Similarly, at each assessment, individual patients could be classified as NP-negative or positive with attribution of event(s) to SLE only, both SLE and non-SLE, and non-SLE-only causes. For some analyses, all NP events were attributed to either SLE or non-SLE causes, in which case those events for which both SLE and non-SLE factors were identified as etiological factors were included with the SLE NP group.
Statistical methods
Individual NP manifestations were categorized by attribution. In addition, the NP manifestations were clustered into subgroups for additional analyses. Thus, the 19 NP syndromes were categorized into central and peripheral nervous system manifestations as described22. In addition, NP events were categorized into diffuse and focal manifestations13: diffuse NP syndromes were aseptic meningitis, demyelinating syndrome, headache, acute confusional state, anxiety disorder, cognitive dysfunction, mood disorder, and psychosis; focal NP syndromes were cerebrovascular disease, Guillain-Barré syndrome, movement disorder, myelopathy, seizure disorders, autonomic neuropathy, mononeuropathy, myasthenia gravis, cranial neuropathy, plexopathy, and polyneuropathy. Medication use was defined by cumulative use of at least 1 medication in 3 non-overlapping drug clusters assembled on the basis of clinical relevance: cluster 1: low-dose aspirin, nonsteroidal antiinflammatory drugs, or COXIB; cluster 2: prednisone, antimalarials, or any immunosuppressive drugs; and cluster 3: medications for treatment of comorbidities such as hypertension, osteoporosis, hyperlipidemia, anticoagulants, anticonvulsants, or other central nervous system related therapies for depression, anxiety, or psychosis. The distribution of patients in the 4-level categorization of NP-positive, with attribution of event(s) to (1) SLE only, (2) SLE and non-SLE, and (3) non-SLE-only causes, as well as (4) a NP-negative group, was examined for associations with the SF-36 component summary scores and SDI scores over time.
Descriptive statistics were used to summarize all variables with percentages, mean ± standard deviation (SD), or median and range as appropriate. A chi-squared test was used to examine the relationship between the attribution of NP events and the distribution of the time (categorized into intervals chosen to give comparable numbers of events in each category) from the diagnosis of SLE to the onset of NP events. Kaplan-Meier-based estimates were used to summarize the cumulative percentage of patients with SLE NP events, non-SLE NP events, or both events over the study period. In addition, we defined a time-to-case resolution variable for the NP events, and used Kaplan-Meier estimates and log-rank tests to investigate the relationships between this event-time variable and the attribution of NP events as well as other NP events categorizations (central vs peripheral, focal vs diffuse).
The relationships between the longitudinal SF-36 scores and patient NP status at each visit, sex, age at enrolment, ethnicity, education status, disease duration at each visit, medication use at each visit, SLEDAI scores (with and without NP variables) at each visit, and SDI scores (with and without NP variables) at each visit were examined by linear regression. Logistic regression analysis was used to examine which subscales of the MCS and PCS scores of SF-36 scores were most highly related to NP status over time and for the cross-sectional relationship between SDI score (without NP variables) and NP status. Estimation was accomplished by generalized estimating equations with a first-order autoregressive working correlation structure in order to allow for the correlation between multiple measurements over time for the same patient.
For cumulative (non-decreasing) SDI scores (with and without NP variables), a non-reversible multi-state Markov model23 was used to investigate the relationships between explanatory variables, such as NP status, and the subsequent rates of transitions to and from damage states defined by the integer values of the SDI scores (0–9 with NP, 0–7 without NP).
RESULTS
Patient characteristics
A total of 209 patients were enrolled (Table 1). They were predominantly Caucasian (92.3%) and female (87.6%) with a mean age (± SD) of 43.7 ± 13.8 years. At enrollment the mean disease duration was 8.4 ± 8.9 years. The spectrum of ACR classification criteria is in keeping with other lupus cohorts24. The frequency of patients with “neurologic disorder,” which includes seizures and psychosis only, was 15%. The mean disease activity and mean cumulative organ damage were low, as reflected by the SLEDAI and SDI scores. Medication utilization was in keeping with an unbiased lupus population. The number of patients who were lost to followup was 24/209 (11.5%) in addition to 10/209 (4.8%) patients who died, but no deaths were due to nervous system disease.
Demographic and clinical manifestations at enrollment of all patients with SLE and those with and without cumulative neuropsychiatric (NP) events regardless of attribution.
Frequency and attribution of neuropsychiatric (NP) events
A total of 132 of 209 (63%) patients had at least a single NP event over the period of study. Eighty-one patients (39%) had 2 or more events, with a maximum of 6 NP events in a single patient. In the 132 patients with NP events there were a total of 299 events (Table 2). The most frequent NP events were headache (32%) and mood disorder (23%). Seven of the NP events had a prevalence of less than 2%. Two of the NP syndromes (Guillain-Barré syndrome and autonomic neuropathy) were not identified.
Neuropsychiatric (NP) events and their attribution since the diagnosis of SLE in 209 patients.
Ninety-two (31%) of the 299 NP events in 54/209 (26%) patients were attributed to SLE, and 207/299 (69%) events in 78/209 (37%) were attributed to non-SLE causes. The most frequent NP events attributed to SLE were cognitive dysfunction (21%), cerebrovascular disease (15%), and seizures (13%), and the most frequent NP events attributed to non-SLE causes were headache (46%), mood disorder (29%), and anxiety (12%).
The onset and attribution of NP events and the relationship to the time of diagnosis of SLE is illustrated in Figure 1. The proportion of NP events attributed to SLE compared to non-SLE causes was highest in the 6 months prior to and in the first year following the diagnosis of SLE (p < 0.0001). Ten NP events in 7 patients that were attributed to SLE had their onset more than 6 months prior to the diagnosis of SLE. These were cerebrovascular events (5 events in 4 patients), seizure disorder (3 events in 3 patients), cognitive dysfunction (1 patient), and myasthenia gravis (1 patient). The median (range) interval between the onset of these 10 events and the diagnosis of SLE was 25 (6–52) months.

The time of onset of neuropsychiatric (NP) events in relation to the date of diagnosis of SLE. All the NP events have been attributed to SLE (SLE NP events) or non-SLE (non-SLE NP events) causes.
Outcome of neuropsychiatric (NP) events
The proportion of patients with NP events and their attribution at each of the study assessments over 7 years are summarized in Table 3. As individual patients could have NP events attributed both to SLE and to non-SLE causes the NP-positive group was divided into 3 mutually exclusive groups (patients with SLE NP events only; patients with non-SLE NP events only; and patients with both SLE and non-SLE NP events). The proportion of patients in each subgroup at study assessments remained remarkably stable over the period of followup, and indicated that up to 49% of patients had some form of NP event recorded at each assessment. The proportion of patients with NP events attributed to SLE only, non-SLE only, and SLE plus non-SLE causes was approximately 1:3:1.
The number (%) of patients with NP events and their attribution at each study assessment over 7 years.
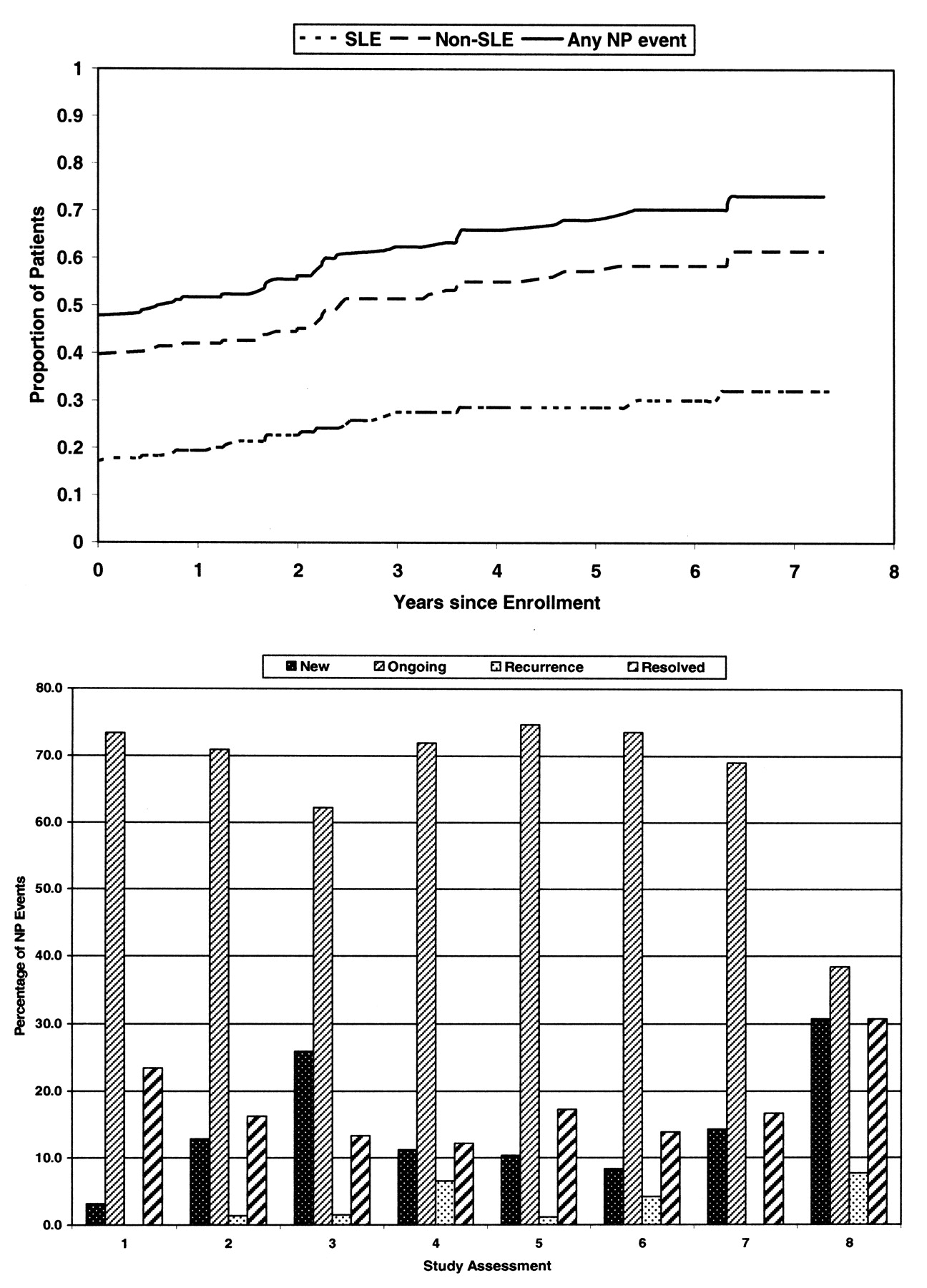
Additional analysis indicated that the cumulative percentage of patients with NP events increased over time: NP events attributed to SLE (32%) and non-SLE NP events (61%); only 27% of patients remained in the NP-negative group by the end of the study (Figure 2). At each assessment (Figure 2) the status of NP disease was a mixture of new, ongoing, recurrent, and resolved events reflecting a dynamic rather than a static process. There was no significant difference (p = 0.13) in the time to resolution between NP events attributed to SLE (median 1.17 yrs) versus those attributed to non-SLE causes (median 1.14 yrs). Similarly, comparisons of central versus peripheral NP events (p = 0.36) and diffuse versus focal NP events (p = 0.89) did not reveal any significant differences.
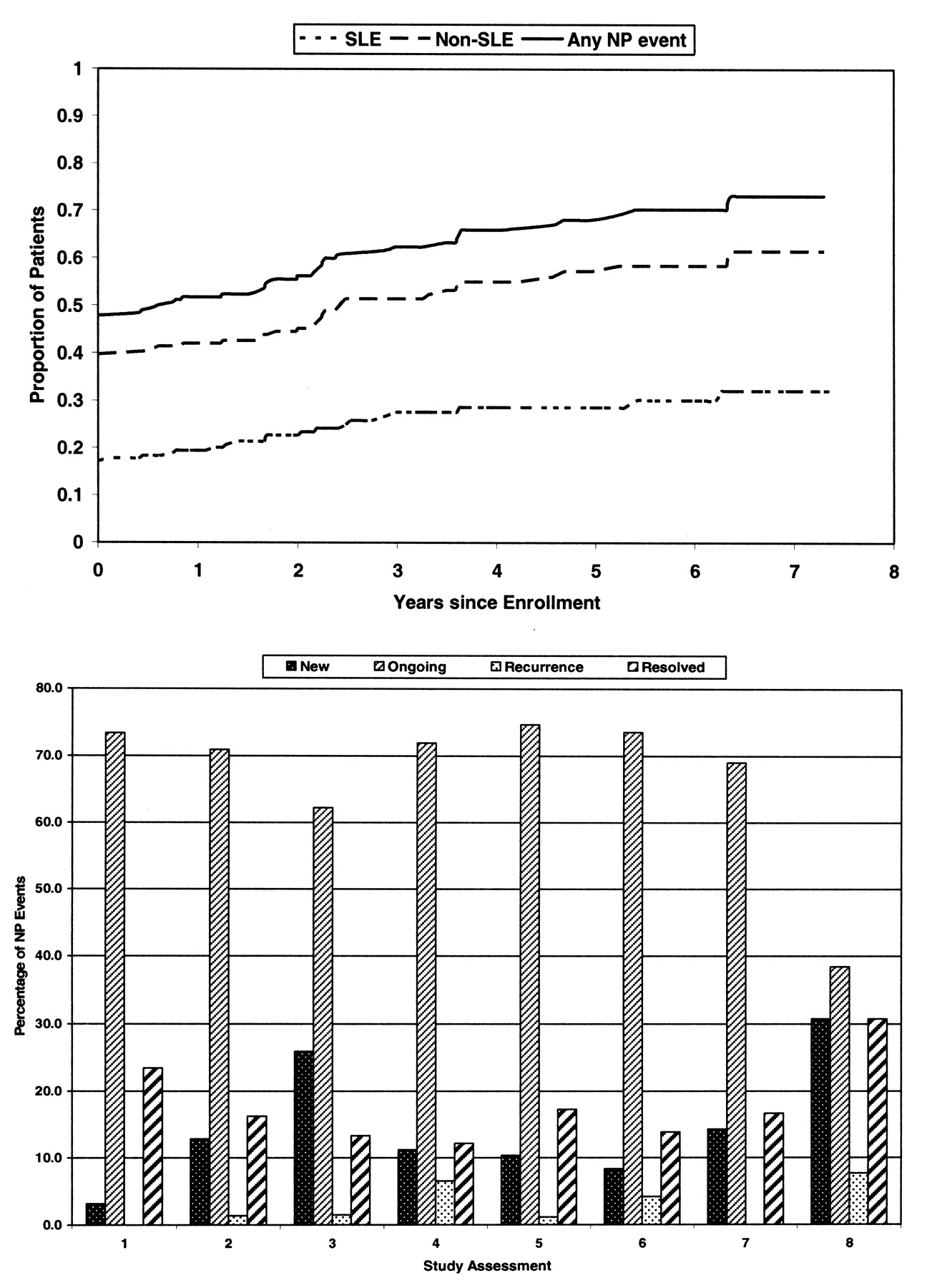
Cumulative NP events in 209 patients with SLE assessed annually for up to 7 years. NP events are attributed to SLE and non-SLE causes and the outcome expressed as the proportion of patients with cumulative NP events (upper panel). Status of NP events at enrollment and at each annual assessment is classified as new, ongoing, recurrence, or resolved (lower panel).
NP events, HRQOL, and cumulative organ damage
Significantly lower group means over time for MCS scores in patients with NP events compared to those without events were observed (43.1 vs 51.9; p < 0.001 in a multivariate analysis). A summary multivariate analysis (Table 4) that used an expanded categorization of NP status also demonstrated associations between lower MCS scores and Caucasian race (p = 0.009), younger age at enrollment (p = 0.029), and overall cumulative medication use (p < 0.001), although there was no significant variation across individual medication clusters for patients receiving medication. Similarly, the group means for the PCS of the SF-36 were significantly lower in patients with NP events (34.3 vs 42.3; p < 0.001 in a multivariate analysis) regardless of attribution. In the summary multivariate analysis (Table 5), other significant associations with lower PCS scores were with lack of college education (p < 0.001), older age at enrollment (p < 0.001), global SLE disease activity excluding NP variables (p < 0.001), and overall cumulative medication use (p < 0.001). The mean MCS and PCS scores at each study assessment are shown in Figure 3 for patients with and without NP events incorporating attribution of NP events to SLE or non-SLE causes.
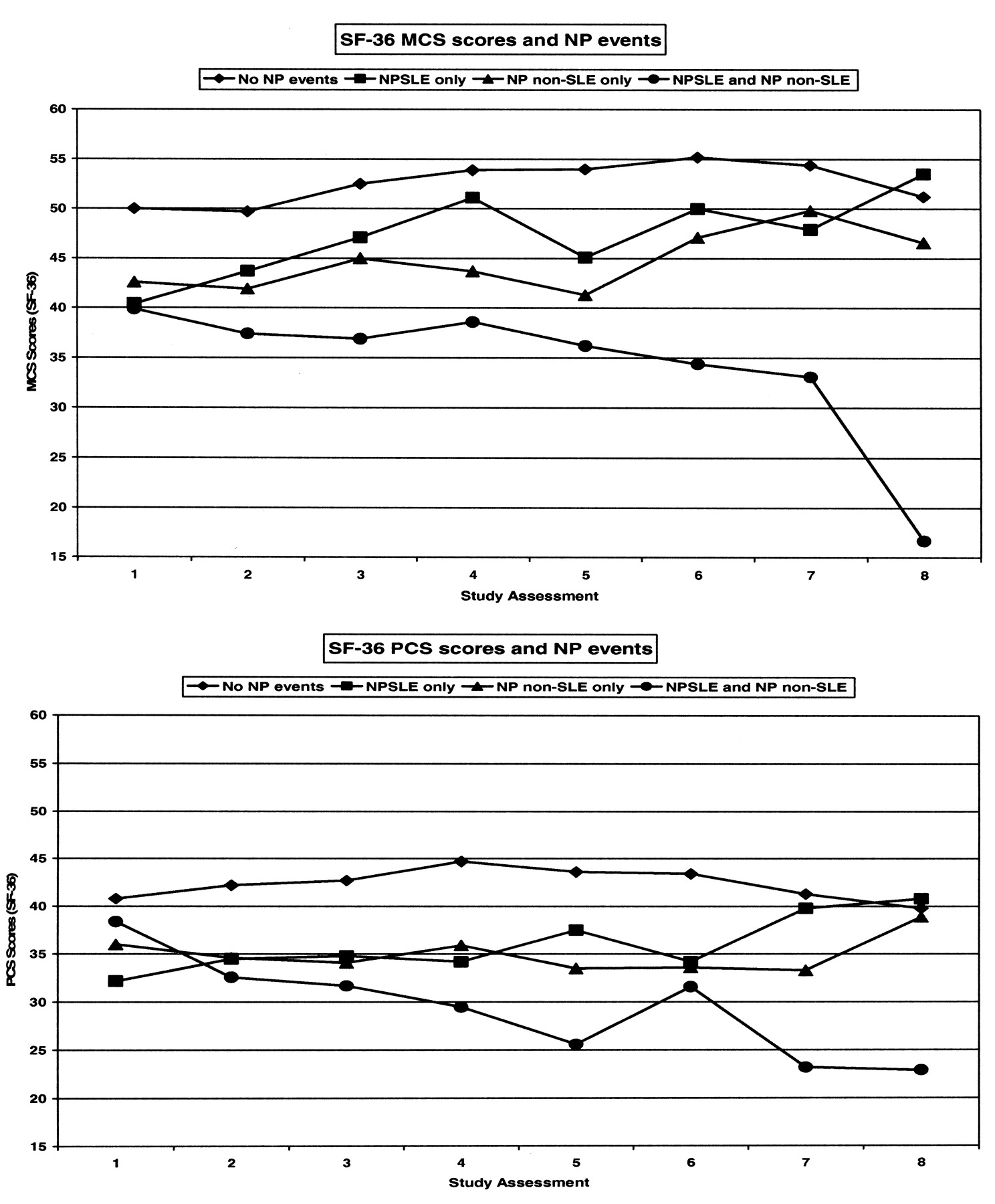
Mean mental (MCS; upper panel) and physical component summary scores (PCS; lower panel) in 209 patients with SLE at enrollment and annually for up to 7 years. The group means over time for both MCS and PCS scores were significantly lower (p < 0.001) in patients with NP events regardless of attribution compared to patients without NP events. Patients with NP events were clustered into groups with events attributed only to SLE (NPSLE only), events attributed to non-SLE causes only (NP non-SLE only), and events attributed to SLE and non-SLE causes.
Multivariate regression analysis for Mental Component Summary scores.
Multivariate regression analysis for PCS summary scores.
A logistic discriminant analysis, to compare patients with NP events to those without events, showed that the difference in MCS scores between these patient groups was primarily due to observed differences in the vitality subscale of the SF-36. A comparable analysis of PCS scores showed that differences were primarily linked to observed differences in the physical function and general health subscales of the SF-36.
While there was no cross-sectional association between SDI scores of cumulative organ damage and HRQOL, there was a suggestive relationship between higher SDI scores (excluding NP variables) and positive NP status (p = 0.04). However, the progressive multi-state model analysis demonstrated no association between subsequent progression of SDI scores and NP events.
DISCUSSION
We examined the longterm outcome and influence on HRQOL of a wide range of NP events prospectively categorized and attributed to SLE and non-SLE causes. Although the cumulative frequency of NP events increases over time, the NP status of individual patients changes between assessments. The presence of NP disease is associated with a significant negative effect on HRQOL. Further, applying previously described decision rules for attribution, it is clear that both SLE and non-SLE related NP events contribute to the self-report reduction in HRQOL.
The demographic features, clinical manifestations of SLE, and medication use indicate an unbiased cohort of patients24 that was predominantly Caucasian, female, and middle-aged, with a mean disease duration of 8.4 years at enrollment. Although 63% of patients had at least 1 NP event over the study, only 31% of these were attributed to SLE. The proportion of NP events attributed to SLE was highest in the 18 months around the diagnosis of SLE. Despite the long study duration, with a total of 741 patient-years of observation, 7 of the 19 NP syndromes had a frequency of ≤ 2% each and 2 additional NP events were not recorded in any patient. The predilection for NP events to present early in the disease course25–28 and the low frequency of some types of NP disease in SLE have been noted in other studies.
Previous cross-sectional studies of patients with SLE have found a high variability in the frequency of NP events, even when the ACR case definitions have been used1–6. The reasons are multiple and include retrospective study design based upon chart review, patient evaluation at a single time in the disease course, and variability in the rigor for determining the attribution of NP events. We prospectively identified all NP events on an annual basis for up to 7 years and systematically applied previously described decision rules for determining their attribution. Patients continue to accrue new NP events over time, attributed to both SLE and non-SLE causes, which may partially explain the discrepancy in the frequency of NP disease between previous cross-sectional studies. This is supported by reports of an association between the occurrence of NP events and disease duration6. At each of the annual study assessments the proportion of patients with NP events attributed to SLE, with or without the co-occurrence of non-SLE NP events, was a minority.
The longterm outcome of NP events, whether attributed to SLE or non-SLE causes, has not been well studied. The limited clinical trials have been uncontrolled, or of short duration, or focused upon a single NP manifestation29–34. The data from observational cohorts have been inconsistent. For example, increased mortality in patients with NP events has been reported in some studies35–37 but not in others28,38,39. In a 2-year followup study12 of 32 patients hospitalized for NPSLE, the outcome was generally favorable, with either substantial improvement (69%) or stabilization (19%). However, Jonsen, et al15 reported a higher frequency of disability in SLE patients with NP disease compared to patients without NP events and to the general population. In our study, there was a resolution of approximately 15% of NP events at each assessment, although the majority of events were persistent. Of interest, the attribution of NP events to SLE or non-SLE causes did not predict their resolution. This is in contrast to the findings from a recent large inception cohort study of SLE13 in which the short-term outcome was more favorable in patients with NP events attributed to SLE. It may be that treatment of NPSLE early in the disease course may have a more favorable outcome, and so may present a therapeutic window of opportunity akin to that seen in other rheumatic diseases40,41.
An indicator of the clinical significance of NP events in SLE patients is self-report HRQOL. Normative data on SF-36 scores are available for the Canadian population42 and the mean MCS and PCS summary scores in patients with NP events are approximately 7 and 16 points below the expected population means. The group mean differences over the course of the study in MCS and PCS scores between patients with and without NP disease were 8.8 and 8.0, respectively. These values exceed the change in mean group scores in patients with scleroderma43 and chronic obstructive pulmonary disease44 who had concurrent clinically significant improvement in disease-specific outcomes while enrolled in clinical trials. The results presented here indicate that the negative relationship between NP events and HRQOL that we have previously reported in cross-sectional studies of SLE3,4 persists over time. As in the earlier studies3,4, there was no statistically significant distinction between the effect of NP events due to SLE and non-SLE causes. Indeed, the data presented in Figure 3 suggest that patients with concurrent NP events attributed to both SLE and non-SLE causes had the lowest mean MCS and PCS scores over time. These findings are in contrast to those found when SLE patients with cognitive dysfunction were studied in a similar manner over 5 years7, and emphasize the importance of including all NP events in clinical studies of NPSLE.
There are a number of limitations to our study. First, as this was not a disease inception cohort, we were unable to accurately determine the outcome of NP events diagnosed and treated early in the disease course. As indicated, the highest proportion of NP events attributed to SLE occur early, and therapeutic intervention at this time may be associated with a better prognosis. Second, although 17 of the 19 NP syndromes identified in the ACR case definitions were represented in our cohort, 7 of the 17 had a frequency of less than 2% over the entire period of observation. Thus, large multicenter studies will be required to specifically address the outcome of such infrequent NP events. Finally, we did not perform routine neuroimaging or neuropsychological assessments on all of our patients, but utilized such investigations when they were clinically indicated and required by the ACR case definitions. Although additional abnormalities would likely have resulted from this approach, our protocol was intended to reflect as much as possible the approach in clinical practice and to avoid the inclusion of subclinical NP disease, which has not been shown to have clinical significance7–10,45–47.
We have demonstrated that in patients with well established SLE, NP events are common and 31% are attributable to SLE. The presence of NP events, regardless of their attribution to SLE or to non-SLE causes, is associated with a significant negative effect on HRQOL, which is independent of cumulative organ damage. Additional studies are warranted to determine which SLE-specific and nonspecific interventions are required to treat these events and improve the outcome of NP disease and HRQOL in patients with SLE.
Acknowledgments
We are grateful for the support of the attending staff rheumatologists (Drs. E. Sutton, V. Bakowsky, D. Mosher, S. Ahmad, S. Shatshat, T. Taylor, and J. Wong) at Dalhousie University and Queen Elizabeth II Health Sciences Centre for allowing us to study their patients.
Footnotes
-
Supported by the Canadian Institutes of Health Research grant MOP-57752 and Capital Health Research Fund (Dr. Hanly), MRC (UK) grant U. 1052.00.009 (Dr. Su), and MRC (UK) grant U.1052.00.009 (Dr. Farewell).
- Accepted for publication January 19, 2009.








{kind=link}
{kind=link}
{kind=link}