

Abstract
Objective. To evaluate the 2-year efficacy and safety of etanercept in patients with ankylosing spondylitis (AS).
Methods. A 96-week open-label extension study, which followed a 12-week double-blind placebo-controlled trial, was designed to provide longterm efficacy and safety data, including radiographic outcomes, for patients treated with etanercept 25 mg twice weekly (NCT00421980). In all, 81 patients were enrolled (96% of the participants from the double-blind study). Key efficacy measures included improvement using the Assessment in Ankylosing Spondylitis 20% (ASAS20) criteria, the Bath Ankylosing Spondylitis Functional Index (BASFI), and the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI). Radiographic progression was evaluated using the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS) method. Paired t tests were used to test within-group changes from baseline.
Results. The percentage of responders, by ASAS20 criteria, remained relatively constant in patients who received etanercept during the 12-week double-blind study (60% at Week 0 and 83% at Week 96 of the open-label extension); more patients from the placebo group became responders after being switched to etanercept (23% and 74%, respectively). A similar trend was also observed using the ASAS40 and ASAS5/6 criteria, the BASFI, and the BASDAI. Most patients had no change from baseline in mSASSS values. Etanercept was well tolerated; the most frequent adverse events were injection site reactions (n = 30; 37.0%) and headache (n = 18; 22.2%), and the most frequent infections were upper respiratory tract infections (n = 43; 53.1%) and flu syndrome (n = 22; 27.2%).
Conclusion. For 2 years, etanercept was clinically effective and well tolerated, with no unexpected safety findings.
- ANKYLOSING SPONDYLITIS
- ASSESSMENT IN ANKYLOSING SPONDYLITIS 20
- MODIFIED STOKE ANKYLOSING SPONDYLITIS SPINE SCORE
- ETANERCEPT
Ankylosing spondylitis (AS) is a chronic rheumatic disease characterized by inflammatory back pain due to sacroiliitis and spondylitis that affects young adults. Joint damage, including erosions, syndesmophytes, and ankylosis, can result in severe longterm functional impairment leading to a compromised quality of life.
Tumor necrosis factor-α (TNF-α) antagonists such as etanercept are remarkably effective at relieving pain and stiffness1–4 and improving mobility and quality of life in AS5,6. In 2 double-blind studies2,3 significantly more patients receiving etanercept responded to therapy than did those receiving placebo. In both studies, the difference between the etanercept and placebo groups was seen as early as 2 weeks after the start of therapy and was sustained for the duration of the study. In a longterm extension study7, the efficacy and safety of etanercept were evaluated over a period of 4 years in North American patients who completed a 6-month double-blind placebo-controlled trial2. The therapeutic effects of etanercept persisted up to 4 years.
We describe 2 years of etanercept experience from a similar open-label study in European patients with AS completing a 12-week double-blind, placebo-controlled trial3. In the original 12-week double-blind study, etanercept produced rapid, significant, and sustained improvement in disease activity measures and spinal flexion, compared with placebo. Improvements were evident at the 2-week visit and were sustained up to Week 12. The current 2-year open-label extension study, which immediately followed the 12-week double-blind study, was designed to investigate whether etanercept could maintain the clinical efficacy and tolerability seen during the double-blind period. The results of the open-label study are presented here.
MATERIALS AND METHODS
Study design
This open-label, multicenter extension study of about 96 weeks followed a 12-week double-blind placebo-controlled study (NCT00421980)3. There was no treatment interruption for patients entering the open-label extension. The Week 12 visit of the double-blind study was considered the baseline visit of the open-label extension. Efficacy assessments were made every 4 weeks for the first 12 weeks and every 12 weeks thereafter; safety assessments were scheduled at 4-week intervals.
The study was conducted from June 2002 to July 2004 in 14 centers in 8 European countries, in accord with the ethical principles of the Declaration of Helsinki, and was consistent with the Guidelines for Good Clinical Practice. The study protocol and informed consent document were approved by each institution’s review board or independent ethics committee.
Patients
Adult patients who had previously completed the 12-week, double-blind, placebo-controlled study were eligible to participate. Enrollment criteria were the same as those described for the double-blind study3. Briefly, patients aged 18 to 70 years, diagnosed with active AS using the modified New York criteria8, were eligible for entry to the original double-blind study3. Active disease was defined as an average visual analog scale (VAS) score ≥ 30 for spinal inflammation and a score ≥ 30 on at least 2 of 3 additional symptom domains (back pain, patient global assessment of disease activity, and physical function). Patients were excluded if they had complete ankylosis (fusion) of the spine; used TNF-α inhibitors previously, including etanercept; used disease modifying antirheumatic drugs other than hydroxychloroquine, sulfasalazine, or methotrexate within 4 weeks of baseline; used multiple nonsteroidal antiinflammatory drugs (NSAID); used > 10 mg prednisone daily; or changed doses of NSAID or prednisone within 2 weeks of baseline.
Treatment
All patients received etanercept 25 mg subcutaneously, twice weekly. Patients who received etanercept during the double-blind study continued their therapy (the ETN/ETN group); patients who received placebo were switched to etanercept (the PBO/ETN group).
Efficacy assessments
The main efficacy variable was improvement in AS as defined by the Assessment in Ankylosing Spondylitis (ASAS) criteria9. ASAS20 responders were defined as patients with a ≥ 20% improvement with a minimum of 10 units in at least 3 of 4 domains [pain, function, inflammation, and patient global assessment (PtGA)], without worsening in the fourth domain by 20% and 10 units9. At the time the study protocol was designed, the ASAS40 and ASAS5/6 criteria for assessing efficacy of therapy were not available. Because these criteria are currently recommended for assessing efficacy of therapy for patients with AS10, retrospective analyses [last-observation-carried-forward (LOCF) method] were performed using the ASAS40 and the ASAS5/6 criteria.
Other efficacy variables included patient and physician global assessments of disease (VAS 0–100 mm); nocturnal and total back pain assessments; the Bath Ankylosing Spondylitis Functional Index (BASFI; VAS 0–100 mm); the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI; VAS 0–100 mm); spinal mobility as measured by the modified Schober test, chest expansion scores, and occiput-to-wall distance; number of painful and swollen joints; serum C-reactive protein levels; and percentage of patients achieving partial remission (defined as score < 20 in each of the 4ASAS domains: patient global assessment, pain, function, and inflammation) 9. Painful (70 joints assessed) or swollen joints (68 joints assessed because the hip joints were excluded) were given a score of 1; joints with no pain or no swelling were assigned a score of zero. For the efficacy evaluations, baseline values from the double-blind study were used.
Radiographic assessments
To assess radiographic progression, digitized radiographs of the cervical (C-spine) and lumbar spine (L-spine) taken at baseline of the double-blind study, and at Week 48 of this open-label extension (Week 60 of observation) or at the early withdrawal visit of this study, were read by a physician who was blinded to the time sequence of images. The modified Stoke Ankylosing Spondylitis Spine Score (mSASSS11,12 — 0, normal; 1, erosions, sclerosis, or squaring; 2, obvious syndesmophyte formation; and 3, total bony bridging) was recorded for each of the 6 vertebral units of each section (bottom anterior or top anterior) for both the C-spine (C2, C3, C4, C5, C6, and C7 in the bottom anterior section and C3, C4, C5, C6, C7, and T1 in the top anterior section) and the L-spine (T12, L1, L2, L3, L4, and L5 in the bottom anterior section and L1, L2, L3, L4, L5, and S1 in the top anterior section).
Safety assessments
Assessments were based on reports of adverse events, the results of routine physical examinations, and laboratory determinations. The National Cancer Institute (NCI) grading scale was used to identify patients with abnormal laboratory test results for hematology and biochemistry. NCI grades 3 and 4 were considered to be of potential clinical importance. Adverse events that coded to the World Health Organization preferred term uveitis or iritis or included the term iridiocyclitis were recorded as uveitis adverse events; adverse events that coded to the preferred term of colitis, colitis ulcer, ileitis and proctitis ulcer, or Crohn’s disease were recorded as inflammatory bowel disease (IBD).
Statistical analyses
Because this was an open-label study, the efficacy and safety analyses are descriptive. The LOCF method was used for imputing missing values. The total mSASSS values at baseline and at Week 60 were calculated for the C-spine and the L-spine, separately and overall. If > 3 scoring vertebral units in a section were missing, the total mSASSS was assigned a missing value; if ≤ 3 units were missing, the mean of the other scoring units was used as a substitute for the missing units. Only patients having total mSASSS at both baseline and Week 48 were included in the radiographic analysis. Basic summary statistics (n, mean, standard deviation, median) are reported by treatment sequence and for all patients. Paired t tests were used to test within-group changes from baseline. Intrareader variability was assessed by calculating the intraclass correlation coefficient between the 2 matched readings of 9 patients, for both baseline and Week 48 images.
RESULTS
Patient characteristics
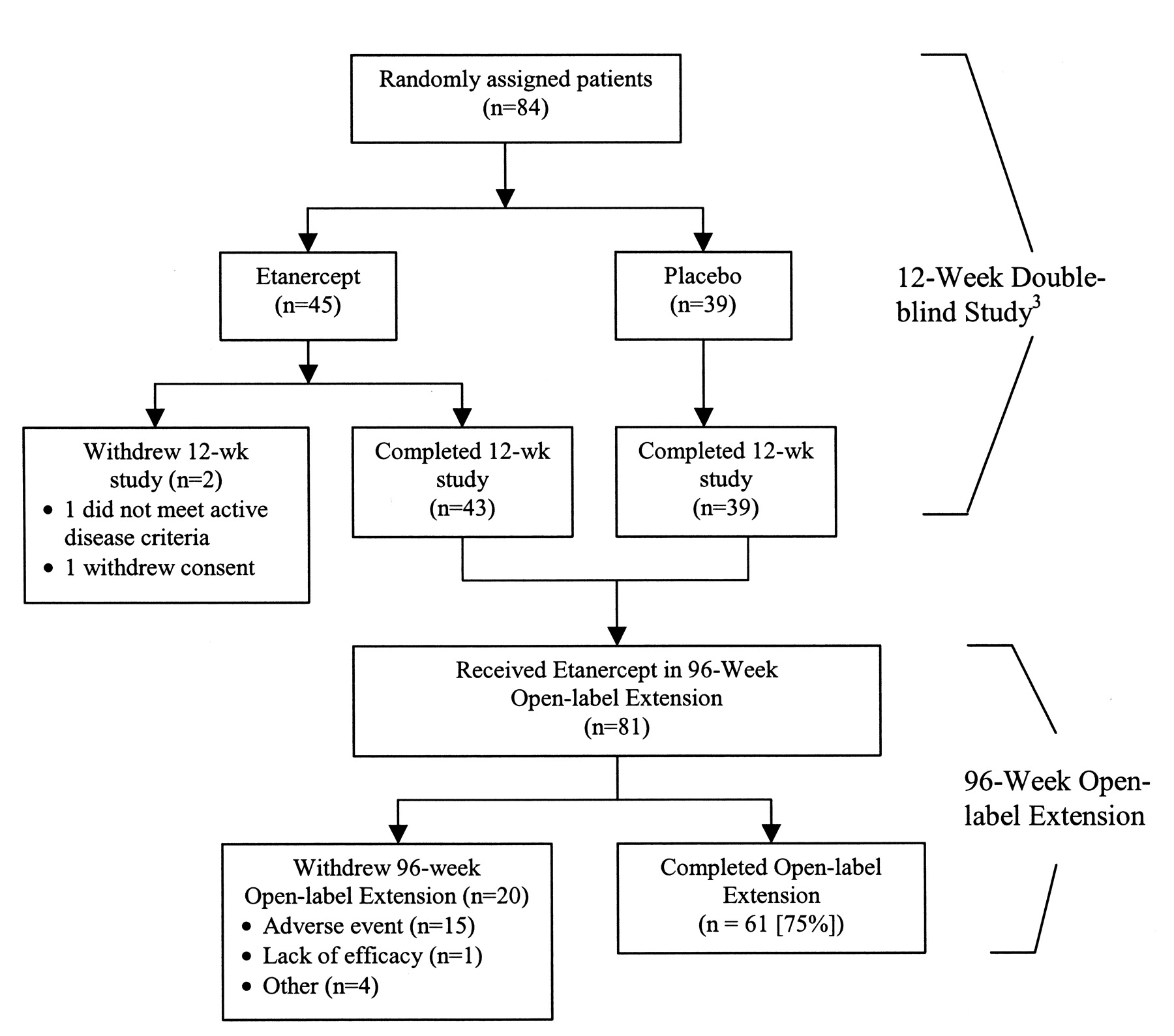
Of the 84 patients enrolled in the double-blind study, 82 (43 from the etanercept group, 39 from the placebo group) completed the 12 weeks and entered the extension study; 81 received the study drug and are included in this report (Figure 1). A total of 130 patient-years of etanercept treatment accrued over the 2 years.
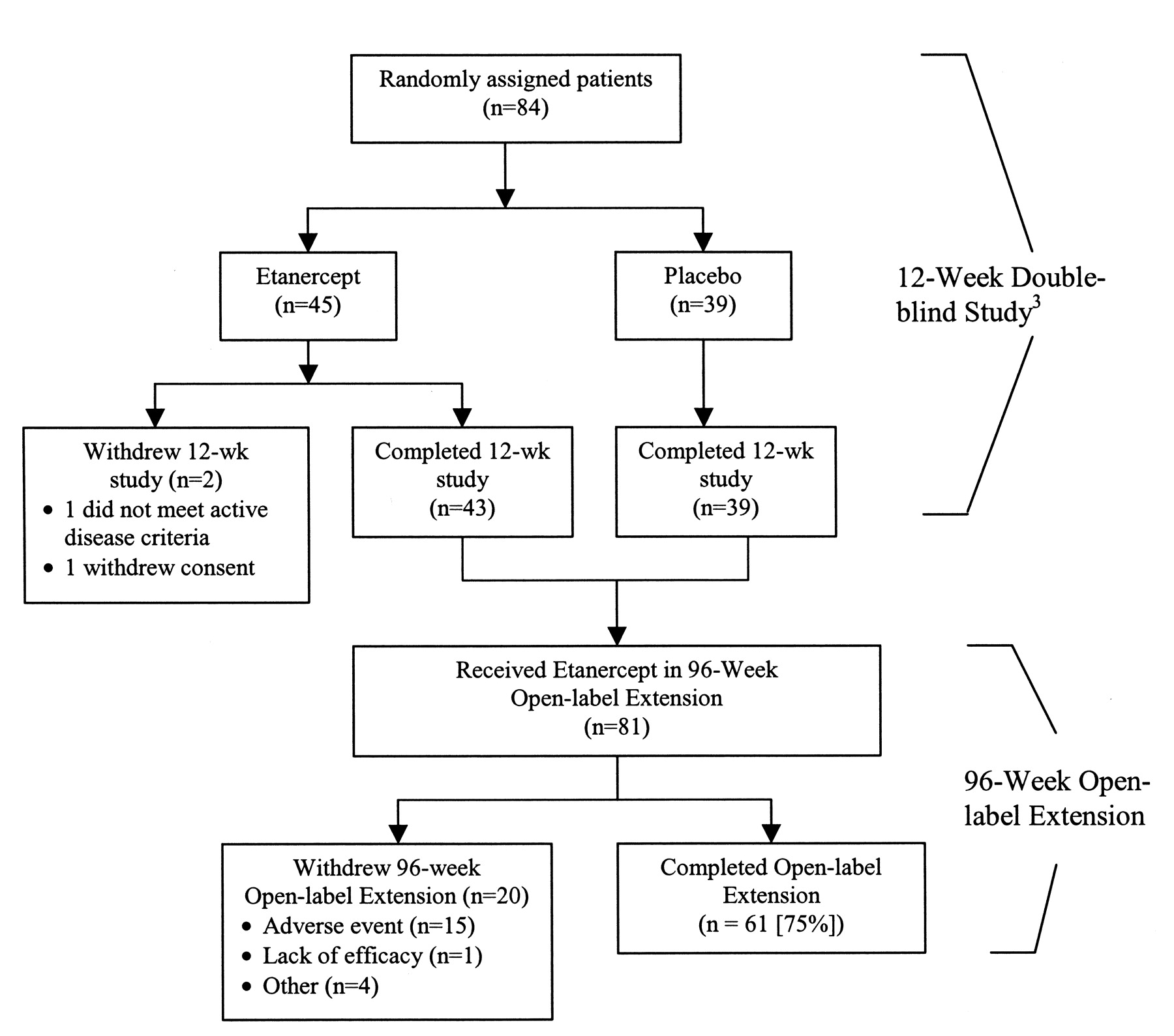
Patient disposition in the 12-week double-blind study and 96-week open-label extension.
The patients who participated in the open-label extension were predominantly men (78%), with a mean age of 43 years and mean disease duration of 12.5 years.
Clinical efficacy. ASAS responses
At the end of the 12-week double-blind study, 60% of patients in the etanercept group and 23% of those in the placebo group had achieved an ASAS20 response. In the extension study, the proportion of ASAS20 responders in the ETN/ETN group increased initially and then remained stable for the duration of the study (Figure 2A). After being switched to etanercept therapy, the proportion of ASAS20 responders in the PBO/ETN group increased markedly, initially, and continued to increase, approaching the proportions seen in the ETN/ETN group (Figure 2B). Overall, 79% of the patients achieved an ASAS20 response at Week 108.

Responders (last-observation-carried-forward method) as determined by the Assessment in Ankylosing Spondylitis (ASAS) criteria. A. Etanercept/etanercept group. B. Placebo/etanercept group.
ASAS40 and ASAS5/6 responses followed a similar trend (Figure 2A, 2B). At Week 108, 59% and 30% of the patients achieved ASAS40 and ASAS5/6 responses, respectively.
Bath AS Disease Activity Index
At the end of the 12-week, double-blind study, the mean BASDAI scores for the placebo group had decreased from 58.6 mm to 50.1 mm (13.6% improvement) and the etanercept group had shown a decrease from 61.0 mm to 33.8 mm (43.6% improvement). During the open-label extension, BASDAI scores for the PBO/ETN group showed continued improvement through Week 108 (Figure 3). The percentage improvement in overall BASDAI scores from baseline was 60% at Week 60 of treatment (corresponding to the timepoint for radiographic assessment) and 57% at Week 108.

Mean BASDAI scores over 108 weeks.
Other clinical endpoints
Individual components of the ASAS criteria (back pain, BASFI, morning stiffness, and PtGA) showed continued improvement during the open-label study in both treatment groups (Table 1). The improvement seen in the PBO/ETN group approached that of the ETN/ETN group for PtGA, the BASFI score, and morning stiffness. Inflammation, assessed by intensity and duration of morning stiffness, continued to improve with etanercept during the open-label study. Similarly, total back pain and nocturnal back pain continued to improve during this study. The ETN/ETN group had less pain than the PBO/ETN group after 108 weeks.
Clinical efficacy assessments: data are mean scores (percentage change from baseline).
Spinal mobility was determined using the modified Schober test, chest expansion scores, and occiput-to-wall distance (Table 2). Improvements in the modified Schober and chest expansion scores were seen early and continued or were sustained over the 2-year period in the ETN/ETN group; occiput-to-wall scores showed little or no change from baseline. The PBO/ETN group showed improvement in all 3 scores after patients switched to etanercept (Table 2).
Spinal mobility assessments: data are mean scores (percentage change from baseline).
At baseline of the double-blind study, there were 14 patients each in the ETN/ETN and PBO/ETN groups with swollen joints and 31 and 28 patients with painful joints; mean tender counts for each group were 6.6 and 9.8, respectively, and mean swollen joint counts were 3.6 and 5.1, respectively. At Week 108, these patients showed a mean improvement (LOCF analysis) of 1.2 (76.1%) and 0.8 (78.4%) in number of swollen joints and 3.1 (68.2%) and 2.5 (63.1%) in number of painful joints in the ETN/ETN and the PBO/ETN groups, respectively. At Week 12 of the double-blind study, partial remission was achieved by 17.8% of patients receiving ETN and 10.3% receiving placebo (p = 0.3457); partial remission was achieved by 15 (36%) and 11 (28%) of patients in the ETN/ETN and the PBO/ETN groups, respectively, by Week 108.
Radiography results
Radiographic data from subjects with valid baseline and post-baseline images were included in the analysis (N = 67). After 1 year of etanercept therapy, radiographic assessments found no evidence of deterioration or disease progression. Overall mSASSS for C-spine and L-spine showed little or no change from baseline at Week 48 for either group (Table 3).
Radiographic assessments (mSASSS scores for C-spine and L-spine) at baseline and at 60 weeks.
Safety and tolerability
Safety data for the double-blind study have been published3. Over the 96 weeks of the open-label extension, 20 (25%) patients were withdrawn; the most common reason for this was the occurrence of adverse events in 15 (19%) patients (Figure 1). No predominant adverse event led to discontinuation; no unexpected adverse events were reported.
Most of the adverse events reported during the open-label extension were mild to moderate in severity; the most frequent treatment-emergent adverse events (excluding infections) were injection site reactions, headache, and abdominal pain; and the most common infections were upper respiratory tract infection and flu syndrome (Table 4). No cases of central demyelinating disease or blood dyscrasias were reported.
Treatment-emergent adverse events (≥ 10%).
A total of 19 patients had serious adverse events (excluding infections and injection site reactions), and no serious adverse event occurred in more than one patient. Five serious infections (requiring hospitalization or parenteral anti-biotics) were reported in 5 patients (0.038 events/year); these included appendicitis, infectious diarrhea, acute gastroenteritis, respiratory tract infection, and bacterial (unconfirmed) arthritis, which occurred in one patient each. No cases of tuberculosis or other opportunistic infections were reported.
Four malignancies (melanoma, metastatic carcinoma, pituitary tumor, and basal cell carcinoma) were reported during the study. One patient (age 64 years), diagnosed with liver metastasis of non–small cell carcinoma of unknown origin 12 months after the start of the double-blind study, died 3 months after discontinuing etanercept treatment despite intensive chemotherapy. The incidence of malignancies over the course of the studies (12-week double-blind study and the open-label extension) was compared with that estimated from the United States NCI Surveillance, Epidemiology, and End Results (SEER) database13. The expected number of SEER–eligible cancers over the course of both studies (the 12-week double-blind study and the open-label extension) was significantly lower (0.556 expected vs 3 malignancies observed; p = 0.019). The one case of basal cell carcinoma not included in the comparison was a recurrence of a lesion that had been resected 2 years previously.
At baseline, 7 patients with a history of IBD were enrolled. Two of these patients had an IBD-related adverse event during the study, and 2 new cases were reported. Both patients with newly emergent IBD were withdrawn from the study, one because of a lack of efficacy and the other because of ileitis; both conditions were subsequently resolved.
At baseline, 26 patients had a history of uveitis. There were 18 reports of uveitis in 10 patients during this study; all 10 patients completed the study. Of these 10 patients, 8 had a history of uveitis; 2 patients who had no history of uveitis developed new symptoms during the study, which resolved on continued treatment.
During the study, there were 5 reports of grade 3 laboratory test result abnormalities; none was associated with an adverse event leading to withdrawal. No particular grade 3 abnormality occurred in more than one patient. One grade 4 abnormality (platelet count) was not associated with any relevant adverse event and returned to normal at the next study visit.
DISCUSSION
This multicenter, open-label study confirmed that etanercept provided substantial and sustained clinical benefits, including spinal mobility, in patients with AS for up to 108 months of treatment. Patients who switched from placebo to etanercept demonstrated rapid and marked improvement in the individual components of the ASAS criteria (back pain, BASFI, morning stiffness, and PtGA); 74% achieved an ASAS20 response, compared with only 23% after 12 weeks of placebo. Overall, 79% of the patients achieved an ASAS20 response at the end of the study. Using more stringent criteria, 59% of the patients achieved ASAS40 responses and 30% achieved ASAS5/6 responses after at least 96 weeks of etanercept treatment.
At the end of the extension study, patients had similar improvements in most measures of physical function and spinal mobility, regardless of whether they had received placebo or etanercept during the 12-week double-blind trial. Compared with the PBO/ETN group, patients in the ETN/ETN group showed little or no improvement in occiput-to-wall measurement, which may be expected, because they were significantly older and had a significantly longer disease duration and a significantly higher occiput-to-wall distance at baseline3. It is notable that only one patient discontinued treatment because of a lack of efficacy and that a total of 31% of the patients achieved partial remission.
ASAS response rates in our study were similar to those reported after 2 years of etanercept therapy in a 4-year open-label extension study7. Patient populations included in the original double-blind studies2,3 were similar, but the duration of the double-blind study preceding this open-label extension study was 3 months3 versus 6 months for the study by Davis, et al2. Etanercept continued to be well tolerated in this 2-year open-label study; there was no increase in the number of adverse events or infections per patient-year compared with that in the preceding double-blind study period. A total of 5 serious infections were reported during the 2 years of this study, resulting in an event rate of 3.8 per 100 patient-years. This rate fell between the 1.6 events per 100 patient-years reported for patients with AS14 and the 6.7 events for patients with rheumatoid arthritis (RA)15, both after 2 years of open-label etanercept therapy.
Four malignancies were reported in this extension study (1 malignant melanoma, 1 metastatic carcinoma, 1 pituitary tumor, and 1 skin carcinoma), and the one patient who had metastases died during this study. The 3 SEER-eligible13 malignancies did not follow any particular pattern. Although the incidence of SEER-eligible malignancies observed in this study was higher than expected, no SEER-eligible malignancies were reported in the study by Davis, et al after 2 years of etanercept treatment at the same dose in 257 patients withAS14. Malignancy data from the 2 studies were pooled because they had similar study designs, inclusion and exclusion criteria, and baseline characteristics. Taken together3,14,16, a total of 6 malignancies (only 3 were SEER-eligible) were reported in 351 patients with AS treated with etanercept for approximately 2 years. The overall exposure in these 2 studies and their longterm extensions was 506 patient-years and the number of expected events was 1.085 based on the SEER database. The standardized incidence ratio comparing the observed to expected was 1.66 (95% confidence interval 0.34 to 4.86). Thus, in these 2 multicenter phase 3 clinical studies of etanercept in patients with AS, there was no statistically significant increase in the incidence of malignancies and, importantly, there were no cases of lymphoma. Our results agree with those of previous studies showing that patients with AS have an overall malignancy risk similar to that in the general population17,18.
Patients with AS are at an increased risk for other inflammatory diseases such as IBD and uveitis19. Unlike the monoclonal anti-TNF agents infliximab and adalimumab, etanercept has not demonstrated a therapeutic effect with respect to IBD, particularly Crohn’s disease20,21. However, these data do not suggest any detrimental effects with etanercept therapy. There were 2 cases of newly diagnosed IBD in this study, and most patients with a history of IBD had no relapses. In a similar study in patients with AS14 there was only one new case of IBD. In a combined analysis of 9 trials22 the incidence of new-onset IBD in patients receiving etanercept was similar to the placebo group, but higher than with infliximab. A combined analysis of placebo-controlled trials of etanercept in the treatment of AS found that the incidence of new cases of IBD (0.75 events/100 patient-yrs) or flares (0.75 events/100 patient-yrs) with etanercept was similar to that seen with placebo (1.294 and 0.0 events/100 patient-yrs, respectively, p not significant)23. An analysis of all patients receiving etanercept in the placebo-controlled trials and in open-label extensions found that there was no increase in the rate of events between Years 1 and 223.
Uveitis occurs in 30% to 40% of patients with AS24. In our study, 32% of patients had a history of uveitis. However, during the 96 weeks of the study, only 18 uveitis events were reported in 10 (12.3%) patients. When data from the original controlled study3 were combined with the extension study data to determine the exposure-adjusted incidence rate of uveitis, the rate of uveitis was higher for the patients in the placebo group than for those treated with etanercept. Although the study was not powered to evaluate etanercept in the prevention of uveitis, these results suggest that etanercept may have a protective effect, which is in agreement with a recent publication in which the uveitis data from 4 placebo-controlled studies in patients with AS were analyzed25. A similar protective effect on subsequent uveitis flares was not seen in a retrospective chart study of 13 patients with spondyloarthropathy26. An analysis of uveitis cases occurring in the United States from the World Health Organization’s adverse drug events database or the National Registry of Drug-Induced Ocular Side Effects (Casey Eye Institute, Portland, OR, USA) found that the incidence of uveitis was higher with etanercept than with either infliximab or adalimumab27. However, the number of reported cases seen with etanercept (43) was well below the number estimated for the general population (53).
Another important safety finding was that no cases of demyelinating disease, blood dyscrasia, lupus, or opportunistic infections such as tuberculosis were reported in this study.
This study found no radiographic progression in most patients with AS after 1 year of treatment with etanercept. Few radiographic data are available today, partly because the radiographic progression in patients with AS is slow. Therefore, it is recommended that the minimal followup time for the evaluation of radiographic progression should be 2 years. In one study28 in which the 2-year radiographic progression of AS in 41 patients receiving infliximab was compared with that of 41 patients receiving conventional treatment (GESPIC), patients receiving infliximab were found to have less progression (although statistically nonsignificant) than the GESPIC cohort, despite being older and having a longer disease duration and greater radiographic damage at baseline. In a study comparing the 2-year radiographic data from the study by Davis, et al in patients with AS receiving etanercept with radiographic progression in historic controls, radiographic progression was not different from the control cohort29. These results are in concordance with a similar comparison between patients with AS receiving infliximab30 and the same control cohort, suggesting that anti-TNF therapy may not be modulating structural changes that are measured by the mSASSS method11,12.
The pathophysiological changes in bone associated with AS could explain why anti-TNF agents may not be effective in reducing new bone formation31. Levels of key target cytokines, such as TNF, involved in syndesmophyte formation are lower in patients with AS than in patients with RA. Recent findings from studies using a mouse model of spondyloarthropathy showed uncoupling of inflammation and joint remodeling. In mouse models of inflammatory arthritis, Diarra, et al32 have shown that inhibition of Dickkopf-1 (DKK-1), a regulatory molecule of the wingless (Wnt) group of proteins, results in the formation of syndesmophytes associated with AS. They also showed that TNF is a key inducer of DKK-1 and that TNF inhibition and DKK-1 blockade resulted in syndesmophyte formation in the mice32. In light of these new data, additional studies are needed to confirm our observations, particularly studies with longer followup in patients with early AS.
This open-label extension study demonstrated that the early clinical benefits of etanercept therapy in patients with AS were sustained for up to 2 years. Etanercept was well tolerated with no new safety signals.
Acknowledgments
We thank Ruth Pereira, PhD, and Maitland Young, PhD, from the Publications and External Communications department at Wyeth for their assistance with the preparation of this article.
B.A.C. Dijkmans received grants from Wyeth for research/fellowships. P. Emery was reimbursed for attending a symposium, speaking at a symposium, and organizing education and has received funds for research funding of a staff member as well as consulting for Wyeth. M. Hakala was reimbursed by Wyeth, the manufacturer of etanercept, for attending the 2006 American College of Rheumatology meeting. M. Leirisalo-Repo was paid for running education programs, speaking at meetings, received consulting fees, and has participated in industry-sponsored drug trials sponsored by Wyeth, Roche, Abbott, Centocor, UCB, and Novartis. E. Martin Mola received fees for speaking and consulting from Wyeth. R. Sanmarti received reimbursement from Wyeth for attending a symposium and fees for speaking and consulting. D. van der Heijde received consultancy fees, research funds, and/or payments for attending a conference from Abbott, Amgen, Centocor, UCB, Wyeth, Schering-Plough, Roche. S. van der Linden has received consultancy fees from Wyeth and fees for organizing educational sessions. J. Sieper has received fees for speaking and funds for research from Abbott, Schering-Plough, andWyeth. C. Salvarani, J. Sibilia, and F. Van Den Bosch have declared no competing interests. L. Paolozzi and J. Wajdula are employees of Wyeth.
Footnotes
-
Supported by a grant from Wyeth Research, Collegeville, Pennsylvania, USA, and Amgen Inc., Thousand Oaks, California, USA.
- Accepted for publication December 31, 2008.








{kind=link}
{kind=link}
{kind=link}