

Abstract
Objective. To describe disease expression and damage accrual in systemic lupus erythematosus (SLE), and determine the influence of ethnicity and socioeconomic factors on damage accrual in a large multiethnic Canadian cohort.
Methods. Adults with SLE were enrolled in a multicenter cohort. Data on sociodemographic factors, diagnostic criteria, disease activity, autoantibodies, treatment, and damage were collected using standardized tools, and results were compared across ethnic groups. We analyzed baseline data, testing for differences in sociodemographic and clinical factors, between the different ethnic groups, in univariate analyses; significant variables from univariate analyses were included in multivariate regression models examining for differences between ethnic groups, related to damage scores.
Results. We studied 1416 patients, including 826 Caucasians, 249 Asians, 122 Afro-Caribbeans, and 73 Aboriginals. Although the overall number of American College of Rheumatology criteria in different ethnic groups was similar, there were differences in individual manifestations and autoantibody profiles. Asian and Afro-Caribbean patients had more frequent renal involvement and more exposure to immunosuppressives. Aboriginal patients had high frequencies of antiphospholipid antibodies and high rates of comorbidity, but disease manifestations similar to Caucasians. Asian patients had the youngest age at onset and the lowest damage scores. Aboriginals had the least education and lowest incomes. The final regression model (R2 = 0.27) for higher damage score included older age, longer disease duration, low income, prednisone treatment, higher disease activity, and cyclophosphamide treatment.
Conclusion. There are differences in lupus phenotypes between ethnic populations. Although ethnicity was not found to be a significant independent predictor of damage accrual, low income was.
Systemic lupus erythematosus (SLE) is a multisystem chronic disease whose manifestations and outcome are known to vary among ethnic groups. Higher prevalence rates have been described in a number of ethnicities, including African Americans1–7, Asians5,8–10, and Aboriginals (Native Americans)11–13. Clinical manifestations, course, and outcome of SLE also differ between ethnic groups8,12–18, with more severe disease and worse outcomes described for some groups, particularly African American and Hispanic patients with lupus14,19–23. Although there are few data to date, studies utilizing review of medical records suggest that SLE in Aboriginals tends to be more severe and outcomes appear to be worse11–13.
Socioeconomic status is an important predictor of poor outcomes in SLE, with multiple studies linking poverty and lack of education with higher rates of mortality and damage24–26. Canada has a universal public healthcare system, providing equal access to the same healthcare system across all ethnic groups and income levels; however, utilization of healthcare resources as well as other health-related behaviors may well differ.
The 1000 Canadian Faces of Lupus project is a multicenter, prospective study of the Canadian lupus population. Its objectives were to determine the influence of ethnicity and socioeconomic factors on disease activity, organ involvement, and disease outcomes. This study is particularly important as ethnic minorities are growing at a faster rate in Canada compared to the rest of the population. There is a marked paucity of North American data on lupus in Asians and Aboriginals (Native Americans), 2 populations that are growing at twice the rate of the general Canadian population27,28. In this article, we present the baseline description of our multiethnic cohort, comparing patients of different ethnic backgrounds, in the setting of a universal public healthcare system.
MATERIALS AND METHODS
Patients
Patients were enrolled at 14 sites across Canada, 10 adult rheumatology clinics and 4 pediatric rheumatology clinics. Our study focuses on the adult rheumatology patients. Patients were eligible if they were identified by the site investigator(s) as having a clinical diagnosis of SLE. A clinical diagnosis of SLE, rather than the requirement to meet the American College of Rheumatology (ACR) criteria for SLE29, was allowed. However, the vast majority (1380/1416) of patients met ≥ 4 criteria at the time of enrollment. Both incident and prevalent cases were included. The number of patients at participating sites who declined enrollment was < 5%. Ethics approval was obtained at each participating site.
Study variables
At the baseline visit, all available medical records were reviewed by the site investigators, and clinical data were abstracted and entered onto a comprehensive form. Clinical manifestations of lupus, including those forming the ACR criteria and those included in the revised Systemic Lupus Activity Measure (SLAM-R)30,31 and the revised SLE Disease Activity Index (SLEDAI-2K)32,33, as well as the date of first occurrence of each manifestation were noted where available. In addition, autoantibody status was recorded for anti-dsDNA (DNA), anti-Sm (Sm), anti-RNP (RNP), anti-La (La), anti-Ro (Ro), and antiphospholipid antibodies (aPL; includes anticardiolipin and lupus anticoagulant). “Ever positive” was collected from the medical record, and blood was collected at the baseline visit and annually to determine current status for antinuclear antibodies (ANA), DNA, Sm, RNP, La, Ro, and aPL. (An individual was considered aPL-positive if either anticardiolipin or lupus anticoagulant was present). Disease activity was measured at baseline and annually using the SLAM-R and the SLEDAI-2K validated lupus activity scales30–33. The SLAM-R also includes a 10-cm visual analog scale (VAS) of physician-assessed global disease activity. Patients also filled out the Self-Assessed Lupus Activity Questionnaire (SLAQ)34, a validated self-reported measure of disease activity, at baseline and each followup visit, which includes a VAS for global disease activity and fatigue. Current and past medication use were recorded and updated at each visit, and patients filled out a generic health status measure, the Medical Outcomes Study Short Form-3635. Components of the Systemic Lupus International Collaborating Clinics/ACR Damage Index (SDI)36,37 were abstracted from the medical record, and reviewed with the patients during the interview, and updated annually. Components of the Charlson Comorbidity Index (CCI)38, a validated measure of comorbidity, were collected and updated in a similar fashion.
Detailed sociodemographic data were collected including age, sex, highest education achieved, total household income, and self-reported ethnicity based on the format and categories used by Statistics Canada39. For the purposes of our analysis, patients were categorized according to the main self-chosen ethnic category; however, patients were allowed multiple choices, and detailed information on parents’ and grandparents’ ethnic background as well as country of origin was also collected. Patients were also asked about smoking habits, physical activity, alcohol use, and perceptions of healthcare access. Questions included availability of a primary care physician, distance from healthcare providers (primary and specialist), and perceptions of difficulty in accessing care providers and medications.
Statistical analyses
Analyses were performed using SPSS 15.0 statistical software (SPSS Inc., Chicago, IL, USA). Ninety percent of enrolled patients belonged to 1 of 4 ethnic groups, therefore the analysis focused on the clinical and sociodemographic differences among these 4 groups. Descriptive analyses of the differences among these 4 ethnic groups were performed with the chi-squared distribution for categorical variables and with analysis of variance for continuous variables. Spearman’s correlation coefficients were computed for associations between continuous socio-demographic variables and disease activity and SDI scores. Multivariate linear regression analysis was performed to ascertain independent predictors of damage. Those variables whose association was found to attain a level of significance of p ≤ 0.01 in univariate analysis were retained in the multivariate analysis. Stepwise, forward, and backward multivariate analyses yielded identical results.
RESULTS
Between July 2005 and September 2007, 1537 patients were enrolled into the study cohort. One hundred twenty-one were pediatric patients; their data will be presented in a separate article. Of the 1416 adults, 826 patients were Caucasian (62%), 249 Asian (19%), 122 Afro-Caribbean (9%), and 73 Aboriginal (5%). Seventy-five patients were excluded from our analysis as their ethnicity was not reported. A further 71 participants were also excluded as their ethnicity was other than the 4 main groups. Demographic data are presented in Table 1. The average age at the baseline visit was 45 ± 15 years, with an average age of onset of 32 ± 14 years. Age at disease onset was highest in Caucasians and Aboriginals at 33 and 34 years, respectively, followed by Afro-Caribbeans (30 yrs), and Asian patients the youngest at 25 years (p < 0.001; Table 1). Ninety percent of all patients were women; however, there were significantly more Asian men at 17%, and only 4% of Afro-Caribbean patients were men (p = 0.001 across groups). Mean disease duration was 12 ± 10 years, and was longest in the Caucasian group at 14 years, and shortest in the Aboriginal patients at 7 years (p < 0.001). High school completion was much lower among the Aboriginal patients, at 55%, in contrast to 85%–93% in the other 3 groups (p < 0.001). Aboriginals and Afro-Caribbeans were twice as likely to report total annual household incomes < $15,000 compared to Caucasians and Asians (23% and 19% vs 11% and 9%; p = 0.004); and less than one-third of Aboriginals and Afro-Caribbeans reported incomes in the highest income bracket (> $50,000/yr) compared to over half of Asian and Caucasian patients (Table 1).
Selected demographic and clinical characteristics of the cohort.
The number of ACR criteria met did not differ among the 4 ethnic groups; however, the frequency of fulfilling individual ACR criteria did vary significantly (Figure 1). Asians and Afro-Caribbeans had more frequent renal involvement, at 59% and 56%, compared to Caucasians (40%) and Aboriginals (39%) (p < 0.001). Asians had the lowest frequency of arthritis (64% vs 82% for total group) (p < 0.001) and serositis (23% vs 34% for total group) (p = 0.002), while Caucasians had more frequent mucocutaneous features (mucosal ulcerations, photosensitivity, and malar rashes; 87% vs 78% for total group) (p < 0.001) except for discoid rashes, which were most common in Afro-Caribbeans (30% vs 11% for total group) (p < 0.001). There were also differences in less typical manifestations of lupus. Asians and Aboriginals were more likely to experience fever (17% and 24%, respectively, vs 10% in Caucasians, and 9% in Afro-Caribbeans) (p < 0.001) and weight loss as part of their lupus (22% and 17%, respectively, vs 11% in Caucasians and Afro-Caribbeans) (p = 0.018), and Aboriginals had more frequent non-malar lupus-related rashes (20% vs 9% for total group) (p = 0.005), cutaneous vasculitis (15% vs 6% for total group) (p = 0.006), and mononeuritis multiplex (6% vs 1% for total group) (p = 0.011).
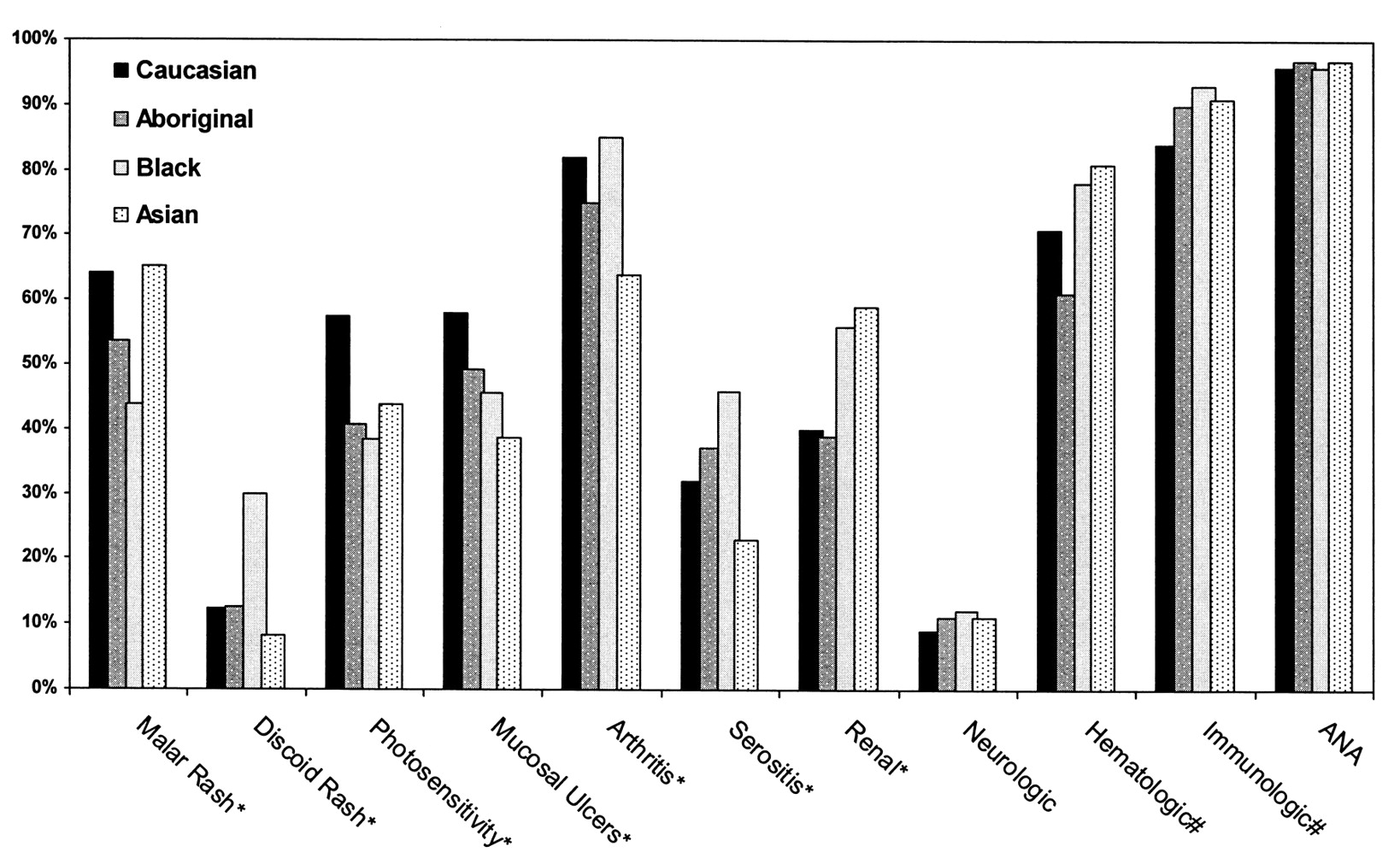
Proportion of patients in each ethnic group meeting individual ACR criteria for SLE at the baseline study visit. Chisquared distribution, *p < 0.001; #p < 0.01.
Serologic differences are shown in Figure 2. DNA antibodies were more frequent in all 3 non-Caucasian ethnic groups at 68% in Aboriginals, 64% in Afro-Caribbeans, and 73% in Asians, compared to 55% in Caucasians (p < 0.001). Sm and RNP were most common in Afro-Caribbean patients at 55% and 48%, compared to 31% and 17%, 27% and 25%, and 39% and 23% in Caucasians, Aboriginals, and Asians, respectively (p < 0.001 for both Sm and RNP). There were no significant differences in the frequency of Ro and La. Fifty percent of Aboriginal and Asian patients were positive for anticardiolipin antibodies, compared to one-third of Caucasian and Afro-Caribbean patients (p = 0.05). The lupus anticoagulant was also more frequent in Aboriginal patients at 28%, compared to 18% in Caucasians, 11% in Afro-Caribbeans, and 10% in Asians (p = 0.004).

Proportion of patients in each ethnic group ever positive for autoantibodies. Chi-squared distribution, *p < 0.001; #p < 0.001; $p < 0.05.
Disease activity as measured by SLEDAI-2K showed no difference among the 4 ethnic groups (data not shown), with an overall mean score of 4.8. SLAM-R scores were significantly lower in Asian patients at 4.10, compared to 6.36 in Caucasians, 7.11 in Aboriginals, and 5.43 in Afro-Caribbeans (p < 0.001). When SLAM-R and SLE-DAI-2K scores were divided into quartiles, there were no differences in the proportion of patients from the 4 ethnic groups in the 4 quartiles of the SLEDAI-2K score (data not shown). However, there was a higher proportion of Aboriginal patients with SLAM scores in the highest quartile at 35%, compared to 10% in Asians, 16% in Afro-Caribbeans, and 23% in Caucasians; and the smallest proportion of Aboriginal patients with SLAM scores in the lowest quartile at 12%, compared to 57% in Asians, 47% in Afro-Caribbeans, and 31% in Caucasians (p < 0.001). Physician global disease activity VAS scores did not differ among ethnic groups (data not shown), with an overall mean of 1.4 cm, but patient global rating of disease activity was significantly lower in Asians at 2.8/10, compared to Caucasians (3.9), Aboriginals (4.1), and Afro-Caribbeans (3.8) (p < 0.001).
Treatment differences
There were no differences in the use of antimalarials, with approximately two-thirds of all patients taking antimalarials at the time of the baseline visit, and about 16% who had never taken antimalarials (Table 2). However, significantly more Asians and Afro-Caribbeans were being treated with prednisone (65% and 67%, respectively) or mycophenolate mofetil (16% and 13%, respectively) at the baseline visit compared to Caucasians and Aboriginals (p < 0.001 for all comparisons). Past treatment with prednisone and mycophenolate mofetil was also higher in Asians and Afro-Caribbeans (Table 2). All non-Caucasian ethnic groups were significantly more likely to have received cyclophosphamide in the past (p = 0.002; Table 2). Current use of cyclophosphamide was low, at about 2% of patients overall.
Treatment.
Asians were least likely to have accumulated any damage, with 59% having an SDI score of zero (p < 0.001; Table 1). Asians also had the lowest mean SDI scores, at 0.95, compared to Caucasians, Aboriginals, and Afro-Caribbeans (1.45, 1.23, and 1.63, respectively; p < 0.001). Univariate associations with damage accumulation are presented in Table 3. As expected, age and disease duration were strongly correlated with damage scores, as was the Charlson Comorbidity Index. Those in the lowest income category had significantly higher SDI scores (1.65 vs 1.03; p = 0.002), as did those without a high school education (1.90 vs 1.39; p = 0.004). Renal involvement (as defined by the ACR criteria for renal involvement) was associated with higher damage scores, and both the total number of ACR criteria met and the physicians’ global disease activity assessments were correlated with significantly worse damage. While those patients who had ever had a positive Sm antibody had higher damage scores, no other autoantibodies were associated with damage scores (data not shown). Those patients currently treated with antimalarials had less damage accumulation, while those who had never been treated with an antimalarial had more. Prednisone, cyclophosphamide, and mycophenolate treatment were all associated with more damage accumulation. Comorbidity, as measured by the Charlson Comorbidity Index, was slightly, but significantly higher in Aboriginals compared to the other 3 groups (p = 0.05; Table 1).
Univariate analyses of associations of clinical and socioeconomic variables with damage.
In multivariate analysis (Table 4), the most important variables in the model to predict damage were disease duration, age, SLAM-R, current prednisone treatment, the use of cyclophosphamide (ever), and low income, with an R2 for the model of 0.27. It is likely that cyclophosphamide and prednisone treatment in this analysis reflect greater disease severity as much as or more than a causal association between treatment and damage, given that this is a prevalent cohort where past treatment patterns and timing of damage accrual are not known. Of note, ethnicity, renal involvement, autoantibodies, education, and antimalarial use were not retained in the model.
Multivariate analysis of association of clinical and sociodemographic factors with damage accumulation.
DISCUSSION
The 1000 Canadian Faces of Lupus study illustrates the marked ethnic diversity of the Canadian lupus population. In our study we have clearly demonstrated ethnic differences in disease expression and therapy, despite a universal healthcare system.
Almost 40% of those in our cohort reported non-Caucasian ethnicity, which is higher than the proportion of visible minority and Aboriginal people in the general population of Canada (17% in 2001)27,40. It is not clear whether this reflects a greater predisposition to lupus in non-Caucasians, or the demography of large Canadian urban centers where most of the participating clinics are located. The distribution of visible minority peoples varies widely across Canadian provinces and cities; the majority of Asian and Afro-Caribbean Canadians live in or near larger urban centers40. The reverse is true for Canadian Aboriginals: only 27% of Aboriginals live in larger metropolitan areas, the remainder live on reservations, rural areas, or communities41. At 5%, the proportion of Aboriginals in our cohort was only slightly higher than that of Aboriginals in the general Canadian population at 3%. Health utilization patterns of Aboriginal people may also play a role; lower rates of specialist contact have been documented for Aboriginal people, in spite of lower health indicators42,43. Visible minority and Aboriginal Canadians are projected to increase to 25% of the population by 201728,41; therefore, although our cohort is clearly not population-based it does indicate the need for further study of the influence of ethnicity on disease expression among patients with lupus in Canada.
Asian and Afro-Caribbean patients with lupus in this cohort had evidence of similarly severe disease, with a high frequency of lupus nephritis, and frequent treatment with corticosteroids, cyclophosphamide, and mycophenolate. However, at an average of 10 years of disease, almost 60% of Asians had no damage accumulation, compared to only 35% of Afro-Caribbean patients with lupus, who also had higher mean SDI scores. Previous studies have reported greater damage accrual in Afro-Caribbean patients, but there are few reports in Asians. In another Canadian study of a multiethnic cohort followed at a single center, Asians had more damage accrual than African-Canadians with similar disease duration and ages44. As described by others, we found that older age was an important predictor for damage accumulation in our cohort25,45,46. Socioeconomic status (household income and education) in Asians in this cohort was on par with Caucasians, while household income was lower for Afro-Caribbeans. While there are no data on Asian patients with lupus, it is likely that higher socioeconomic status had an important protective effect on damage accumulation for Asians in this cohort, as has been shown in studies of other ethnic groups20,26,47.
Lupus in Aboriginal Canadians in this study was less severe than previously described11–13, essentially very similar to the Caucasian group. The main differences were higher comorbidity scores in spite of shorter disease duration, and significantly lower levels of education and household income. Onset age was also not different from that of the Caucasians, again different from previous reports, which describe a younger onset age. This may relate to the methods, as the previous reports were population-based, while our study is based on those patients presenting for care to lupus clinics, and agreeing to participate in the study. Alternatively, it is also very possible that due to the long disease duration of the cohort (7 yrs for Aboriginals, 12 yrs overall), those Aboriginal patients with the most severe disease did not survive to become part of the cohort (survivor bias), thus underestimating disease severity for the group as a whole. Such a survival bias may also underestimate disease severity for the entire cohort.
Aboriginal Canadians in this cohort also had a strikingly high prevalence of aPL, a previously unreported finding. The significance and implications of this finding are not clear. There is a well described association between aPL and infections48–50, and rates of many infections are more common in Aboriginals, including hepatitis C, otitis media, gastroenteritis, and tuberculosis51–54. We do not have data on infectious exposures in this cohort. Rates of venous thrombotic events were not higher in this group (data not shown), but atherosclerotic events (myocardial infarctions and cerebrovascular accidents) as collected in the SLICC Damage Index and the Charlson Comorbidity Index were highest in Aboriginals, at 20%, compared to 11% in Caucasians, 7% in Afro-Caribbeans, and 5% in Asians (p = 0.002). However, smoking rates and prevalence of diabetes were also highest in Aboriginal patients (data not shown). The relative importance of aPL in Aboriginal patients with lupus is an important area of future research.
Low household income was one of the strongest predictors of damage accrual in this cohort, in spite of supposed equal access to healthcare. Some previous studies47,55,56, but not all22, have found low income or low socioeconomic status to be a predictor of damage and poor outcomes. Low income and mortality in lupus are more clearly linked57,58. There is an extensive body of literature showing overall socioeconomic status to vary inversely with outcomes in chronic disease in general59–61. The persistence and strength of this variable in the setting of public healthcare support the complex interaction between socioeconomic status and health-related behaviors.
A number of limitations are recognized in our study. Concerns include the definition of the ethnic groups. While we report ethnic groups in 4 large categories, clearly there are differences to be found within these groups. Further, the effect of mixed parental heritage and heterogeneous backgrounds was not taken into account by these methods. Data on detailed ethnic origin are collected and will be the subject of future analyses. Genetic admixture analysis would be a valuable tool to better account for mixed ethnic heritage and determine the genetic component of ethnicity and its contribution to disease course and outcome, as has been shown successfully in other studies62,63. We are in the process of collecting DNA, and hope to do this in the future.
As this is largely a prevalent rather than an incident cohort, patterns of past disease activity are not known, past clinical manifestations may have been missed, and treatment burden underestimated. As mentioned, those with the most severe disease may be less likely to survive for inclusion in the cohort, making differences between ethnic groups less evident and limiting conclusions about the disease course.
We have shown there are differences in lupus phenotypes between ethnic groups when examining age of onset, clinical manifestations, and autoantibody profiles. Further, although we did not demonstrate ethnicity to independently predict accumulation of damage, we did find that low income remains a very strong independent predictor of damage accrual, despite a setting of universal healthcare. It may well be that genetic factors are most important in determining disease activity and clinical manifestations, but that socioeconomic factors are more important in determining longterm outcomes.
Acknowledgments
We thank the CaNIOS coordinators and research assistants for their dedicated work in recruiting the patients: Andrea Craig, 1000 Faces National Coordinator, University of Manitoba; Jaime Claudio, PhD, CaNIOS National Coordinator, University Health Network; Sara Hewitt and Janine Ouimet, St. Joseph’s Health Centre, London, Ontario; Mellissa Moyen, Health Sciences Center, Winnipeg; Michele Tobaly and Tania Santopietro, Montreal General Hospital; Diane Ferland, Hopital Maisonneuve-Rosemont, Montreal; Sherri Simpson and Katrin Smith, Ottawa Hospital; Tony Hong, America Uribe, and Meghan MacLeod, Vancouver General Hospital; Annella Wehlage, Lethbridge, Alberta; Jessica Bernstein, Jewish General Hospital; Tamara McKenzie, University Health Network.
Canadian Network for Improved Outcomes in Systemic Lupus Erythematosus (CaNIOS) 1000 Faces Investigators: Glinda S. Cooper, PhD, Environmental Protection Agency, Washington, DC, USA; Lori Albert, MD, S. Carette, MPhil, MD, and R.D. Inman, BA, MD, Toronto Western Hospital, University Health Network, Department of Medicine, University of Toronto, Toronto, Ontario; Carol Hitchon, MD, MSc, Health Sciences Centre, University of Manitoba, Winnipeg, Manitoba; Lori Tucker, MD, and Ross Petty, MD, Vancouver Children’s Hospital, University of British Columbia, Vancouver, BC; Gaelle Chedéville, MD, Sarah Campillo, MD, Karen Duffy, MD, and Rosie Scuccimarri, MD, Montreal Children’s Hospital; Murray Baron, MD, and Laeora Berkson, MD, Jewish General Hospital, McGill University, Montreal, Quebec; Suzanne Ramsey, MD, and Adam Huber, MD, IWK Grace Health Centre, Dalhousie University, Halifax, Nova Scotia, Canada.
Footnotes
-
Supported by a grant from The Arthritis Society National Office, Toronto, Ontario, Canada.
- Accepted for publication January 8, 2009.








{kind=link}
{kind=link}