

Abstract
Objective. To evaluate the development of hepatitis B virus (HBV) infection in patients receiving tumor necrosis factor-α-blocking agents (TNFBA), and to evaluate whether lamivudine (LAM) prophylaxis can reduce the risk of viral reactivation in inactive HBsAg carriers.
Methods. Local experience and published reports were reviewed. Patients with HBV infection were classified as having chronic HBV hepatitis, or being inactive HBsAg carriers or occult carriers.
Results. Three patients in our series and 24 patients in the literature were identified: 2 had active HBV-associated disease, 23 were inactive HBsAg carriers, and 2 occult carriers. When exposed to TNFBA, HBsAg-inactive carriers pretreated with LAM had lower risk of having detectable HBV-DNA (p = 0.02) or viral reactivation (p = 0.046) than those without LAM prophylaxis. In 3 patients who discontinued TNFBA, LAM prophylaxis was also discontinued 10–12 months thereafter without hepatitis flares. Two cases of reactivation in occult carriers (HBsAg-negative, anti-HBs+, anti-HBc+) were described in the literature.
Conclusion. TNFBA should be avoided in patients with active HBV replication and should be used with caution in inactive HBsAg carriers. In these patients, the risk of viral reactivation seems to be high, but it might be reduced by prophylactic LAM, which should probably be given for a long time when TNFBA are discontinued (e.g., 12 mo). Potential occult carriers might carry a low, but not negligible, risk of viral reactivation. They should therefore be monitored with particular care.
Hepatitis B virus (HBV) infection is one of the most common chronic viral infections affecting the liver, and a leading cause of cirrhosis and hepatocellular carcinoma. Reactivation of HBV replication in patients undergoing immunosuppressive therapy is a well recognized complication of considerable clinical importance.
Presence of chronic HBV infection is generally considered a contraindication to the use of tumor necrosis factor-α-blocking agents (TNFBA)1. Indeed, there have been cases of reactivation of viral replication, with fulminant or lethal hepatitis, in inactive HBsAg carriers who received TNFBA for inflammatory bowel diseases2,3 or rheumatological disorders4.
HBV reactivation may occur also after the discontinuation of immunosuppressive drugs, when T cells may recover their immunocompetence and destroy infected hepatocytes, but no information on the outcome for HBV+ patients treated with TNFBA after the suspension of these agents is available.
Data deriving from onco-hematological literature suggest that prophylactic treatment with antiviral agents can reduce the rate of reactivation and the mortality associated with hepatitic flares. Lamivudine (LAM), an inhibitor of the viral RNA-dependent DNA polymerase, is the agent of choice, for its favorable risk-benefit ratio and its low cost. The preventive effect of LAM in this setting was demonstrated by randomized clinical trials5 and by a metaanalysis that included also cohort studies with or without historical controls6, in which LAM prophylaxis reduced the incidence of viral reactivation and the severity of hepatitis flares induced by chemotherapy.
Since information on the use of TNFBA in HBV+ patients is based only on reports of single cases or very small series, usually with a very short followup, we describe our experience of the use of prophylactic LAM in 3 inactive HBsAg carriers treated with TNFBA for rheumatoid arthritis (RA), focusing particularly on a prolonged followup, in which 2 patients suspended TNFBA under the protection of LAM, and could thereafter also withdraw LAM without complications. We reviewed the literature with the aim of comparing the outcome of inactive HBsAg carriers treated with TNFBA who received prophylactic LAM with that of those who did not receive prophylaxis.
MATERIALS AND METHODS
Patients
At our department, from 1999 to October 2008, 558 patients were treated with at least one TNFBA for rheumatic diseases. Since January 2004, all patients receiving, or planned to receive, either immunosuppressive disease modifying antirheumatic drugs (DMARD) or biological agents (TNFBA, interleukin-1-blocking agents, anti-B cell antibodies) were evaluated for HBV markers, including HBsAg, anti-HBs, and anti-HBc. For HBV infection, patients were classified according the American Association for the Study of Liver Diseases7 guidelines as: chronic hepatitis B (HBsAg persistently positive, HBV-DNA > 10,000 copies/ml, elevated aminotransferase); or inactive carriers (HBsAg-positive, aminotransferase persistently normal; HBV-DNA < 2,000 copies/ml). Patients with anti-HBs negative and anti-HBc positive were considered potential occult carriers8. Among our series, we identified 3 inactive HBsAg carriers with active RA refractory to various combinations of DMARD, who, after informed consent, were treated with LAM and TNFBA, as described9.
HBV-DNA was measured by branched-DNA polymerase chain reaction assay (HBV-DNA 3.0; Siemens, Milan, Italy). Sensitivity limit is 2,000 copies/ml.
Review of the literature
This was performed using the Medline database for the keywords “hepatitis B virus,” “tumor necrosis factor alpha,” “infliximab,” “etanercept,” and “adalimumab.” Additional articles of interest were selected from the bibliographies of the published literature. Nineteen articles describing a total of 27 patients with HBV infection exposed to TNFBA were retrieved2–4,9–24 (Table 1). These patients also were classified as active carriers, inactive carriers, or potential occult carriers, as described above.
Clinical and demographic characteristics of 27 HBV+ patients treated with TNF-α-blocking agents (TNFBA).
RESULTS
Case reports
Patient 1: A 73-year-old woman, HBsAg-positive, with a 36-year history of rheumatoid factor (RF)+, anti-cyclic citrullinated peptide (CCP)+, active RA [28-joint disease activity score (DAS28) = 7.64], previously treated without success with gold salts, penicillamine, methotrexate (MTX), sulfasalazine (SSZ), cyclosporine, azathioprine, hydroxychloroquine (HCQ), leflunomide, anakinra in various combinations; initiated LAM prophylaxis in May, 2004; HBV-DNA was undetectable. In June 2004, etanercept (ETA) 25 mg twice a week was started, continuing prednisone 5 mg/day. A moderate European League Against Rheumatism (EULAR) response was initially achieved, but she relapsed and had recurrent upper respiratory infections. ETA was therefore discontinued in June 2007, and 12 months later LAM was also discontinued. No flare of HBV infection was documented during followup.
Patient 2: A 67-year-old woman, HBsAg-positive, with a 6-year history of RF+, active RA (DAS28 = 6.13), previously treated without success with gold salts, HCQ, MTX, cyclosporine, in various combinations, initiated LAM prophylaxis in April 2005. HBV-DNA was undetectable. At the same time, infliximab 3 mg/kg was started while continuing with prednisone 5 mg/day and MTX 10 mg/week. A moderate EULAR response was initially achieved, but she relapsed. In April 2006, TNFBA therapy was switched to ETA 25 mg twice a week; this obtained a moderate to good EULAR response. The patient is still receiving LAM + ETA + MTX + prednisone at the usual dosage. No flare of HBV infection was documented during a 43-month followup.
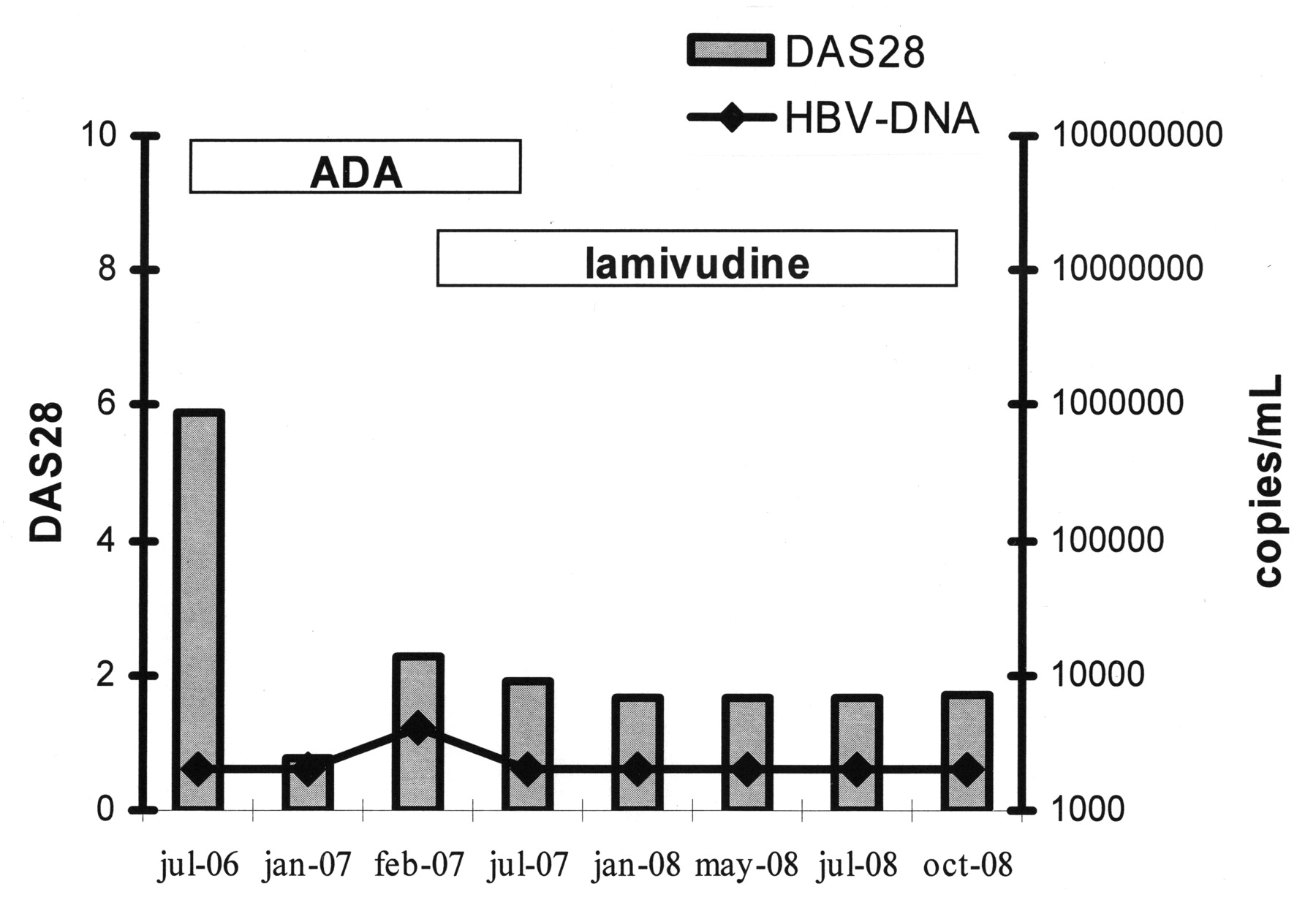
Patient 3: A 56-year-old man, HBsAg-positive, with a 6-year history of RF+, anti-CCP+ RA was evaluated by another rheumatologist in July 2006. He was previously treated without success with HCQ, MTX, cyclosporine, SSZ, in various combinations. Since active disease was present (DAS28 = 5.68) despite combination therapy with MTX 10 mg/week, SSZ 2 g/day, and methylprednisolone 4 mg/day, adalimumab (ADA) 40 mg every other week was prescribed, discontinuing MTX. At that time HBV-DNA was below the sensitivity limits (Figure 1). EULAR remission (DAS28 = 1.66) was obtained. However, in January 2007, mild signs of HBV replication (4,144 copies/ml) were detected and the patient was referred to our attention. LAM was prescribed, with normalization of HBV-DNA. After steroid tapering, since RA remission persisted, ADA was interrupted in July 2007. Twelve months later, LAM was suspended without problems. He is still in remission receiving SSZ, and aminotransferase and HBV-viremia are still within normal limits.

Clinical and laboratory progress in a HBV+ patient treated with TNF-α-blocking agents. DAS28: 28-joint Disease Activity Score; ADA: adalimumab.
Review of the literature
Nineteen articles describing 27 patients with HBV infection exposed to TNFBA were retrieved2–4,9–24 (Table 1). No article described more than 3 patients. Eight patients received infliximab for Crohn’s disease2,3,13,17,18,20 and 19 patients were treated for rheumatic diseases [12 with RA, 6 with ankylosing spondylitis (AS), 1 with adult onset Still’s disease]. Ten of them received infliximab, 10 ETA, and 2 ADA, and 3 patients received more than 1 TNFBA sequentially.
As for HBV infection status, 2 patients had active HBV-associated disease when they were treated with TNFBA, 23 were inactive carriers, and 2 were occult carriers.
TNFBA in active HBV-associated disease: In 1 patient with Crohn’s disease and cirrhosis13, and another with RA and chronic hepatitis with active HBV replication23 who were treated with TNFBA, LAM was used as a therapy and not as a prophylaxis, without significant improvement of viral replication or other liver measures.
TNFBA in inactive HBsAg carriers: The progress of 23 patients considered as inactive carriers, as they had no apparent signs of active HBV-correlated disease at the time of exposure to TNFBA, is shown in Figure 2: 16 did not receive any prophylaxis, while 7 were pretreated with LAM before or when starting TNFBA. Among patients receiving LAM prophylaxis, mild increase of HBV-DNA (< 10,000 copies/ml) was observed in only 1 case, in which liver enzymes remained normal and viral replication was under control12, whereas in the other 6 patients no worsening of liver function or virological status was observed. The median time of exposure to TNFBA in these patients was 21 months (range 4–43) for a total of 149 months.
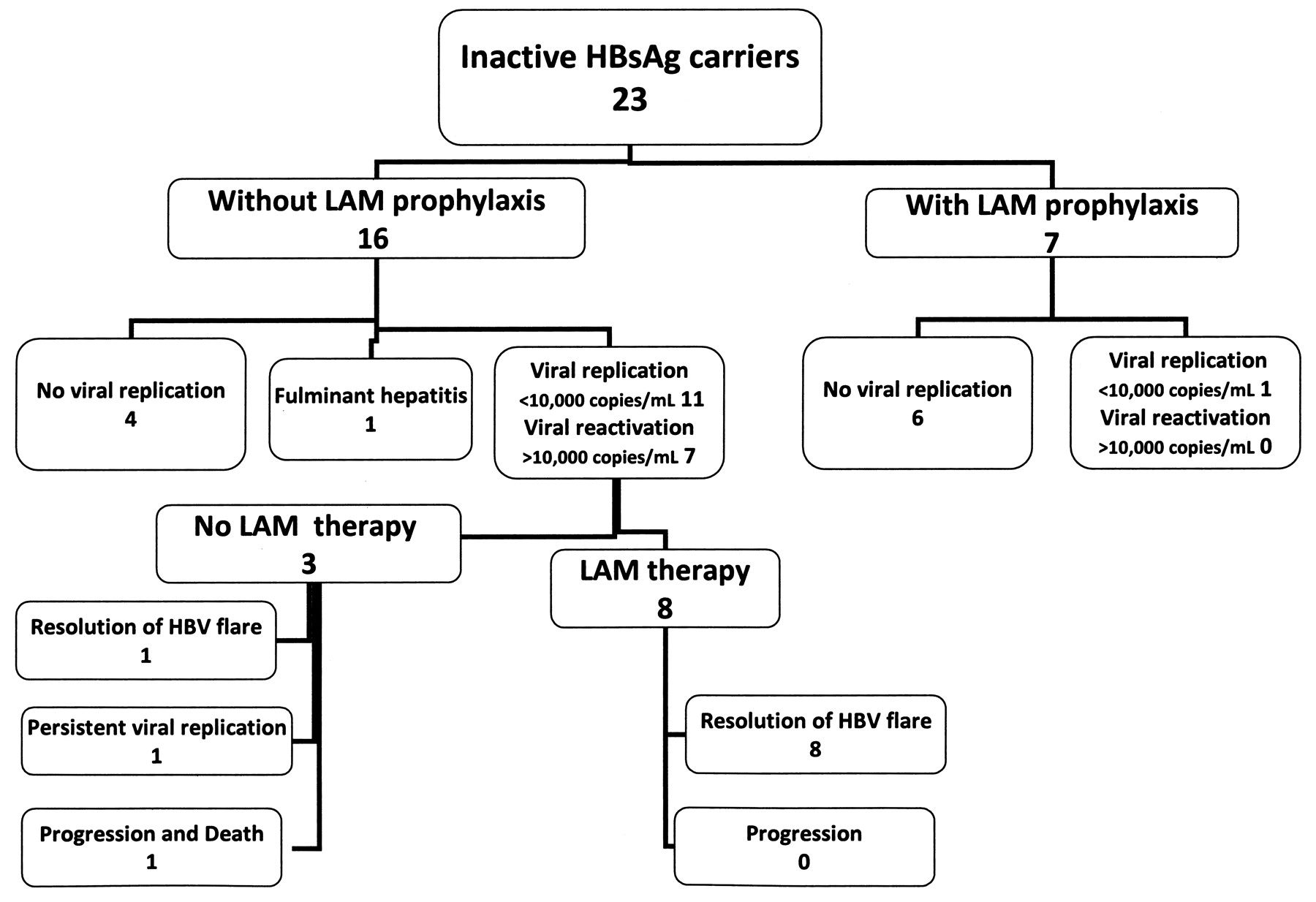
Outcomes of 23 HBsAg+ inactive carriers exposed to TNF-α-blocking agents. LAM: lamivudine.
Among the 16 inactive carriers who received TNFBA without LAM prophylaxis, no sign of viral reactivation was described in 4 patients15,19,22, followed for a median time of 12.5 months (Figure 2); while in the other 12 patients, fulminant hepatitis (possibly attributed by the authors to HBV) in 1 case4, and increase of viral load, with or without hepatitis, in 11 cases, were reported (Figure 2). In 8 of these last 11 patients viral reactivation was detected within the first 6 months of TNFBA therapy, but cases of reactivation after 2 years in which anti-TNF therapy was administered without complication were also described18,21. In most cases, a picture of acute or subfulminant hepatitis, with rise of aminotransferase serum levels in the range of 10–30 times upper limits of normal (ULN), and high levels of viral replication were observed3,10,14,18,20. In a few cases there was only mild (2–4 times ULN), or even no, increase of liver enzymes, and viral replication was not quantified19, or was below 10,000 copies/ml (patient 3 of our series, and16,21), when treatment with LAM was started.
In all, 8 patients were treated with LAM after the detection of viral replication induced by TNFBA: the drug was efficacious in all cases (Figure 2). Median followup with LAM in the 8 patients treated after the detection of viral replication was 6 months (range 2–56), for a total of 101 months. No case of hepatitis flare was described in these patients.
The only case with bad outcome was reported by Michel, et al4: an inactive HBsAg carrier with adult onset Still’s disease who, 2 weeks after receiving the second dose of infliximab, developed a fulminant hepatitis that required liver transplant despite the use of LAM. However, there was no evidence of HBV reactivation (serum HBV-DNA undetectable; no sign of chronic hepatitis and no evidence of HBsAg in the extracted liver). Therefore the etiological role of HBV in this case was unclear.
Finally, 3 patients did not receive antiviral therapy despite viral reactivation: 1 with fulminant hepatitis died before receiving liver transplant2, whereas other cases with spontaneous normalization of HBV-DNA2 or persistence of milder viral replication with normal liver enzymes17 were described (Figure 2).
TNFBA in HBV occult carriers: Two cases of reactivation of HBV occurred in occult carriers (HBsAg-negative, anti-HBs+, anti-HBc+), after 14 and 24 months of therapy with TNFBA18,24, respectively. Both patients were successfully treated with LAM, and in 1 case24 TNFBA therapy was restarted.
TNFBA discontinuation in HBV+ patients: 3 patients (patient 1 and 3 of our series, and18) suspended TNFBA, while continuing with LAM for 10–12 months, without reactivation.
Excluding the case of Michel, et al, which is difficult to interpret, HBV-DNA was detectable in 11 out of 15 patients without LAM prophylaxis versus 1 out of 7 who received LAM prophylaxis (p = 0.02; 2-tailed Fisher’s exact test). Considering that in 1 patient HBV-viremia was not quantified19, viral reactivation, with HBV-DNA > 10,000 copies/ml, was observed in 7 out of 14 evaluable patients who were not pretreated with LAM versus none of 7 pretreated patients (p = 0.046).
DISCUSSION
The management of patients with RA (or other rheumatic disorders) and HBV infection is a complex issue that deserves particular care and cooperation between different specialists9. An unrecognized HBV infection may expose patients with rheumatic diseases to the risk of potential complications when receiving traditional DMARD and/or biological agents. Clear screening recommendations are therefore needed in candidates for these treatments and have been provided by several authorities. For example, according to the Associazione Italiana Studio del Fegato (AISF)25 and the US Centers for Disease Control and Prevention26, all these patients should be tested for serologic markers of HBV infection, including not only HBsAg, but only anti-HBc and anti-HBs antibodies. The presence of HBV infection may also cause delay or avoidance of the use of immunosuppressive drugs, with the risk of undertreating rheumatic patients who need such therapy.
In particular, the effects of the use of TNFBA in HBV+ patients are not clear, since information on this issue is scarce. Examining published data, we observed that a clear picture of acute or subfulminant hepatitis was observed in at least 7 out of 14 evaluable inactive HBsAg carriers exposed to TNFBA. In other cases, milder induction of viral replication, with moderate or no increase of liver enzymes, was described. Although publication bias cannot be excluded, with increased probability of reporting of worse cases, these data suggest a high rate of viral reactivation when HBsAg+ patients are exposed to TNFBA.
These results are not unexpected since TNF-α may play a role in clearing and controlling HBV by synergizing with interferons in suppressing viral replication27–29. Inactivation of TNF-α by TNFBA could therefore lead to enhanced viral replication and reactivation of hepatitis30.
Although antiviral treatment with LAM, when instituted, was able to control the infection in all the reported cases, 1 patient with fulminant hepatitis who did not receive LAM died before receiving liver transplant2.
There are, however, observations from the literature, and from our experience, suggesting that prophylaxis with LAM may prevent viral reactivation and hepatitis flares, analogous to what has been observed in onco-hematological studies5,6,31,32. Publication bias can also not be excluded in this case, with increased probability of reporting cases with better outcome. Therefore, these observation are preliminary and caution must be taken when considering the use of TNFBA in patients with HBsAg positivity. These observations suggest, however, that when this is planned, adequate HBV treatment with LAM should be used, irrespective of the presence of active viral replication.
In the long term, the benefits of LAM may be limited due to gene mutations resulting in resistance to the drug, which may be associated with severe flares of hepatitis. Among patients treated with TNFBA, LAM resistance was described only in a patient with active chronic hepatitis23. More data with longer followup are needed in order to determine the real incidence of viral reactivation in this setting, and the clinical and virological predictors of it. In LAM-resistant HBV mutants, alternative drugs such as adefovir dipivoxil are a therapeutic option, and may be needed to gain longterm control of the underlying HBV infection9.
Two cases of viral reactivation were observed also in occult HBsAg-negative carriers18,24. Since patients with HBc antibody positivity are generally not excluded from treatment with TNFBA and the frequency of occult carriers is much higher than that of HBsAg-positive patients, the number of potential occult carriers exposed to TNFBA is probably very great. Therefore, the risk of viral reactivation for patients with a known history of HBV who are HBsAg-negative appears to be significantly less than in HBsAg-positive patients, but data from the literature indicate that it cannot be totally ruled out. This possibility suggests that if treatment with TNFBA is initiated in patients identified as potential HBV occult carriers, they should be closely monitored for clinical and laboratory signs of HBV reactivation (e.g., with frequent monitoring of HBsAg, as suggested by AISF25).
There are no case reports of HBV reactivation after discontinuation of TNFBA. However, fatal HBV reactivation has been described in inactive carriers (HBsAg+, HBV-DNA-negative), treated with low-dose MTX and steroids for RA, shortly after discontinuation of the treatment32–36. Therefore, we suggest that if introduced, antiviral treatment should be continued for a long time after stopping TNFBA. We present here the results of 2 patients of ours who could discontinue TNFBA with 12 months of LAM therapy, and a similar case has been described by others18.
Conclusions of our study are limited by the small number of patients evaluated and by possible publication bias. However, based on the reported results we suggest that (1) in patients with active HBV replication the use of TNFBA should be avoided. (2) Even if no signs of active viral replication are present, TNFBA should be used with caution in inactive HBsAg carriers. In these patients, the risk of viral reactivation seems to be high, but it might be reduced by prophylactic LAM, analogous to what happens in other immunocompromised patients. (3) When TNFBA are discontinued in HbsAg+ patients, LAM prophylaxis should probably be continued for a long time (e.g., 12 mo). (4) Potential occult carriers (HBsAg–, anti-HBc+) might carry a low, but not negligible, risk of viral reactivation. They should therefore be monitored with particular care.
Footnotes
- Accepted for publication January 13, 2009.








{kind=link}
{kind=link}