

Abstract
Objective. To determine if clinical guidelines recommending therapeutic exercise for people with knee osteoarthritis (OA) are supported by rigorous scientific evidence. To explore whether the magnitude of treatment benefit reported in randomized controlled trials (RCT) is associated with exercise dosage or study methodology.
Methods. We conducted a metaanalysis of RCT comparing some form of land-based therapeutic exercise with a nonexercise group using pain and self-reported physical function outcomes.
Results. The 32 included studies provided data on almost 3800 participants. Metaanalysis revealed a beneficial treatment effect: standardized mean difference (SMD) 0.40 [95% confidence interval (CI) 0.30 to 0.50] for knee pain; SMD 0.37 (95% CI 0.25 to 0.49) for physical function. While the pooled beneficial effects of the 9 RCT evaluating exercise programs providing fewer than 12 direct supervision occasions or the 9 RCT judged to have a low risk of bias remained significant and clinically relevant, the magnitude of treatment benefit pooled from these RCT was significantly smaller than the comparator group (12 or more supervision occasions, moderate to high risk of bias, respectively). The mode of treatment delivery (individual treatments, exercise classes, home program) was not significantly associated with the magnitude of treatment benefit.
Conclusion. There is evidence that land-based therapeutic exercise has at least short-term benefit in terms of reduced knee pain and physical disability for people with knee OA. The magnitude of the treatment effect was significantly associated with the number of direct supervision occasions provided and study methodology (assessor blinding, adequate allocation concealment).
People with symptomatic knee osteoarthritis (OA) complain of deep, aching pain. In early disease, pain is intermittent and mostly associated with joint use. For many people, symptomatic disease will progress. The knee pain becomes chronic, often also present at rest and during the night. The daily functional activities required to remain independent become increasingly more difficult. In fact, knee OA is responsible for more disability in walking, stair climbing, and housekeeping in noninstitutionalized people aged 50 years and over than any other disease1,2. Ultimately, chronic knee OA can also lead to reduced physical fitness and increased risk of cardiovascular comorbidity3,4.
Altered biomechanics and reduced neuromuscular control, resulting in localized stress on the articular cartilage and increased joint loading rate, have important roles in both the initiation and progression of knee OA5–10. Currently, there is no known cure for OA. However, disease-related factors, such as impaired muscle function and reduced fitness, are potentially amenable to exercise. Most international clinical guidelines advocate therapeutic exercise as the first line of effective disease management for people with knee OA11,12. The objective of our metaanalysis was to determine whether these recommendations are supported by a high level of scientific evidence. If the majority of clinical trials conducted to date have been small or poorly conducted, the magnitude of treatment benefit reported may be overestimated. We also wished to explore whether the reported magnitude of treatment benefit was associated with aspects of exercise program dosage or delivery mode. Do we have evidence of what constitutes an optimal graded exercise program for people with knee OA?
MATERIALS AND METHODS
Five electronic databases were searched: Medline, EMBASE, CINAHL, PEDro (Physiotherapy Evidence Database), and the Cochrane Central Register of Controlled Trials (CENTRAL; The Cochrane Library) up to December 2007. The search strategies were specific to each database (Appendix: Medline search strategy).
Reports of randomized or quasirandomized controlled trials (RCT), published in the English language, comparing some form of land-based therapeutic exercise with a nonexercise group among people with either an established diagnosis of knee OA according to accepted criteria or self-reporting knee OA on the basis of chronic joint pain (without radiographic confirmation) were considered for inclusion. The exercise program could include any land-based (in contrast to water-based), but not perioperative, therapeutic regime aiming to relieve the symptoms of knee OA. The comparator (control) group could include any nonexercise intervention, including no treatment or waiting list. The trial needed to include an assessment of knee pain or self-reported physical function. For our metaanalysis, data from the outcomes assessment conducted immediately after completion of the treatment program (or the most immediate assessment post-treatment) have been used.
The 2 authors (SM, MF) independently screened retrieved clinical studies for inclusion, extracted data from all included studies, and conducted the methodological quality assessment. If agreement was not achieved at any stage, a third review author (Dr. Mary Bell) adjudicated.
Methodological quality assessment
The quality of each included RCT was evaluated according to 3 criteria: (1) blinding of outcomes assessment; (2) appropriate handling of withdrawals and dropouts; (3) adequate allocation concealment.
An overall assessment was then assigned: low risk of bias (all 3 criteria met); moderate risk of bias (1 or 2 criteria met); or high risk of bias (no criteria met).
Data analysis
Standardized mean differences (SMD) and a random-effects model were used to combine treatment effects, extrapolated from mean change scores and related standard deviations (Review Manager 5, The Cochrane Collaboration). Change scores were used, as many of the studies were small and demonstrated marked differences at baseline between the allocation groups. Authors were contacted if these data could not be extrapolated from the published manuscript.
Sensitivity analyses were conducted according to treatment delivery mode (individual, class-based, home programs) and the number of directly supervised contact occasions. Sensitivity analyses were also conducted on critical aspects of study methodology (blinding of outcomes assessment, statistical analysis method, allocation concealment) and an overall assessment of bias risk. Differences in treatment effect between the stratifications were tested with chi-squared distribution.
RESULTS
Characteristics of the included RCT
Of the 85 retrieved clinical trails identified from the literature searches, 32 RCT met the inclusion criteria13–45. Four of the included studies recruited people with hip or knee OA18,20,23,44. Contact with the authors provided data specific for participants with knee OA. Of the 32 included studies, 1 large study had 2 clearly different land-based exercise groups (aerobic walking and resistance training) and was treated as 2 trials, with the sample size of the control group being equally divided between the 2 exercise groups17. Two of the included studies included both a hydrotherapy and a land-based exercise allocation18,20. Only the land-based arm was evaluated in our review. Two studies allocated participants to 221 or 324 forms of muscle strengthening. The mean effect of the exercise allocations were combined and compared with the control group.
One study25 had treatment allocations combining exercise with ultrasound or hyaluron, another study had 3 active treatment allocations, 2 of which included a weight reduction program30, and a third study had 4 allocations, 2 involving a spouse-assisted coping strategy intervention27. Only the allocation to exercise alone was considered in our systematic review. One study45 included participants without knee pain. Data were provided by the author on the 37 participants with knee pain and confirmed knee OA.
The pain outcome measure for 1 study35 was not included as all participants were required to take daily non-steroidal antiinflammatory drugs (NSAID), a study design factor we considered would unfairly attenuate any pain-relieving benefit attributable to the exercise program. Two studies did not provide self-reported physical function as an outcome measure27,40.
Most studies recruited 50 to 150 participants. However, 11 (36%) studies recruited fewer than 25 participants in 1 or both allocation groups13,14,18,21,27,32,37–40,45, while 1 study recruited more than 750 participants41.
Participant characteristics
Sample recruitment varied widely, with studies recruiting exclusively community volunteers15,17,20,26,33,34,36, specialist rheumatology or orthopedic clinic patients18,38,39,42, a mix of community volunteers and specialist clinic patients14,27,32,35, general physician referrals22,41,44, or patients on the physiotherapy waiting list16,19. Approximately 50% of participants in 1 study reported a symptom duration of less than a year44, while other studies reported a mean symptom duration of more than 10 years29,32. Most studies stated that the American College of Rheumatology diagnosis criteria were used for study inclusion. However, “knee pain in the past week”33 and patellofemoral knee pain36 were sufficient in 2 studies. Two other studies required at least Kellgren and Lawrence Grade III radiographic disease for study participation37,42. Studies ranged from those excluding people taking NSAID14 to others including only people currently taking NSAID at least twice a week28. One study recruited only overweight or obese participants [body mass index (BMI) ≥ 28 kg/m2]30, resulting in a sample with a mean BMI of 34 kg/m2. This range of recruitment strategies and inclusion criteria resulted in a wide variability in baseline radiographic and symptomatic disease severity between studies, when reported.
Exercise programs
A wide range of therapeutic exercise programs were assessed. All included studies were categorized into 1 of 3 groups according to the treatment delivery mode: individual treatments, class-based programs, or “home” programs. However, it should be noted that many “home” programs incorporated home visits by a trained nurse or community physiotherapist. Also, most individual treatments or class-based programs included provision of a home exercise program.
Treatment content varied from mostly aerobic walking programs17,28,30,32,40 to very complex, comprehensive programs including manual therapy, upper limb and/or truncal muscle strengthening, and balance coordination15,16,34,37,44, in addition to the more usual lower limb muscle strengthening. Two studies evaluated tai chi classes20,39.
Apart from delivery mode and content, treatment “dosage” varied widely between studies. The total number of monitored exercise sessions provided ranged from none35,40 to 36 or more14,17,27,30,32,34. Monitored treatment sessions, in either individual or class-based format, ranged from 30 minutes14,22,29,44 to 90 minutes28 per session. The total treatment duration ranged from 1 month16 to 6 months30,33,45 and 2 years41. Treatment intensity ranged from “maximum effort” muscle strengthening21,38 to low intensity aerobic walking14,30,40.
Methodological quality
According to our criteria of methodological quality assessment (see Materials and Methods), only 9 (28%) studies could be considered low risk of bias from the published report. A further 14 (44%) were categorized as at moderate risk of bias, while the remaining 9 (28%) had a high risk of bias.
Magnitude of treatment effect
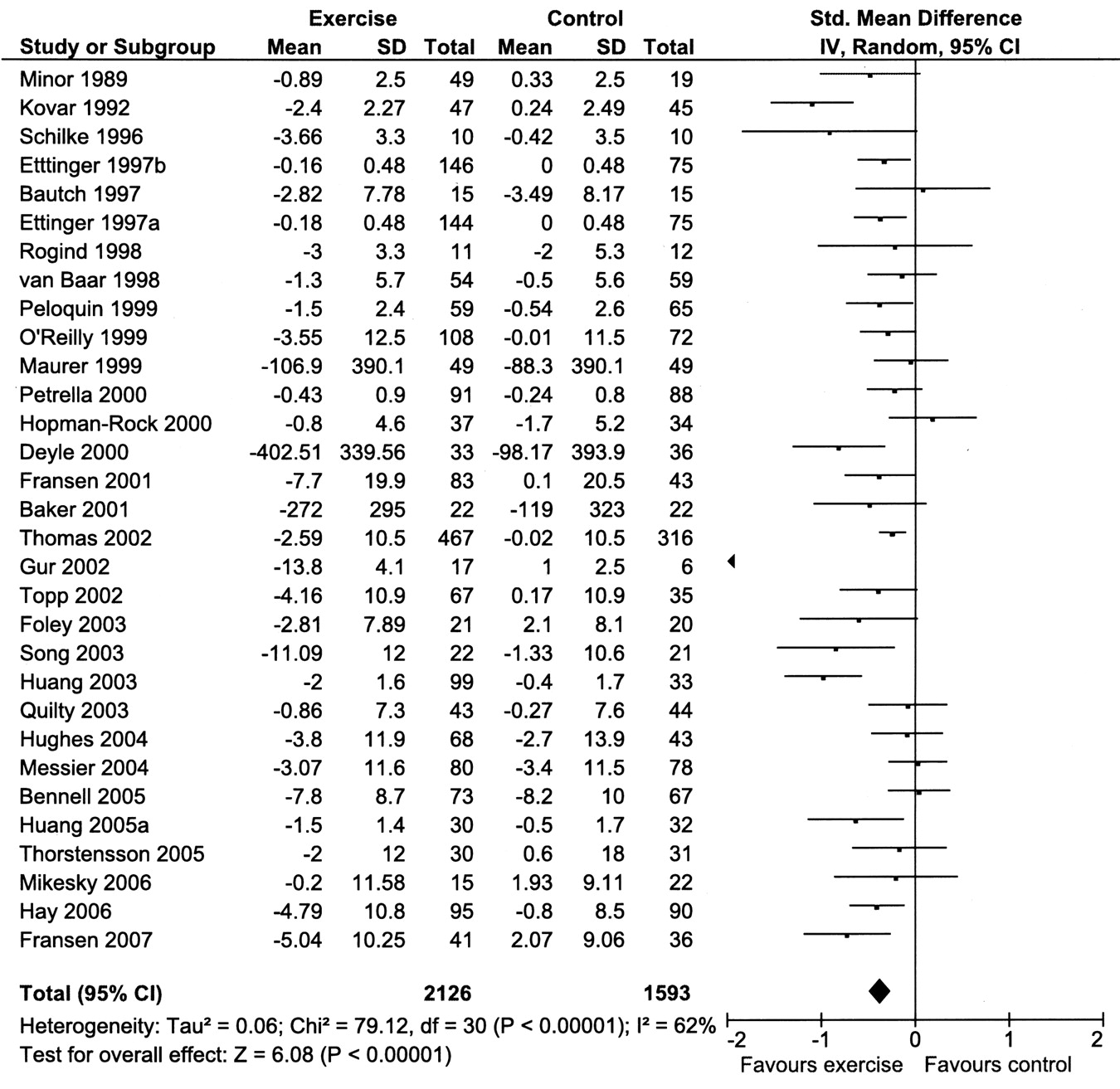
All included RCT (Figures 1 and 2): The 32 included RCT provided data on almost 3800 participants. Combining results demonstrated a statistically significant benefit (SMD) using a random-effects model of 0.40 (95% CI 0.30 to 0.50) for knee pain and 0.37 (95% CI 0.25 to 0.49) for self-reported physical function. Both these effect sizes would be considered small46. Between-study heterogeneity was marked: I2 = 47% and 62% for pain and physical function, respectively.

All randomized controlled trials: knee pain outcome. Mean change, standard deviation, sample size for treatment and control groups.
All randomized controlled trials: physical function outcome. Mean change, standard deviation, sample size for treatment and control groups.
Sensitivity analyses (Table 1)
Effect size estimates for knee pain and physical function. Subgroup comparisons.
Treatment delivery mode: All included RCT were stratified to exercise programs delivered individually to the patient15,16,21,24,25,29,36,38,44, provided in a class-based format14,17,18,20,26–28,32,34,37,39,42, and exercise programs mostly undertaken by the patient at home13,22,33,35,41,43. All 3 forms of treatment delivery achieved significant treatment benefits in terms of pain and physical function. The difference in mean effect size among these 3 categories did not reach statistical significance for knee pain or physical function (Table 1).
Supervision occasions: All included RCT were stratified according to the number of directly supervised sessions provided (in clinics or as home visits): those providing fewer than 12 occasions15,16,22,23,33,35,36,40,41,45, and the others providing 12 or more occasions. Both categories achieved significant treatment benefits in terms of pain and physical function. However, programs providing fewer than 12 direct supervision occasions demonstrated only small mean benefits for pain and for physical function. Studies evaluating programs providing 12 or more direct supervision occasions demonstrated moderate mean effect sizes for pain and physical function. The difference in mean treatment effect between the 2 categories of exercise programs was significant for both outcome measures (Table 1).
Blinding of outcomes assessment: All included studies were stratified according to whether the blinding of outcomes assessment was reported (blinded) or those RCT with uncertain blinding or where blinding of outcomes assessment was not part of the study design (unblinded). Just over half (56%) of the 32 studies clearly stated that the outcomes assessor was blinded to group allocation15–18,20,22,23,25,29,30,34–37,39,41,44,45.
Both subgroups achieved significant treatment benefits. However, blinded outcomes assessment was clearly influential on the magnitude of treatment effect. Blinded studies demonstrated a small mean treatment effect for pain and for physical function. Unblinded studies demonstrated moderate treatment effects for pain and for physical function. The difference in mean treatment effect size between these 2 subgroups was significant for both outcome measures (Table 1).
Statistical analysis method: All included studies were stratified according to the method chosen to deal with study participants without followup data or dropouts: intention-to-treat (all randomized participants) or efficacy analysis (only participants with followup data or only treatment completers). Both subgroups achieved significant treatment benefits. RCT using the more rigorous intention-to-treat analysis demonstrated a small mean effect for pain and for physical function, compared with the larger effects demonstrated by studies using efficacy analysis. However, the difference between the 2 subgroups did not reach statistical significance for either outcome measure (Table 1).
Allocation concealment: All included RCT were stratified according to the adequacy of allocation concealment: 15 RCT reporting randomization procedures providing adequate allocation concealment13,15–20,22,30,33,35,36,39,41,44 and the others not reporting sufficient details of the randomization procedure to be certain that allocation was concealed.
Both study subgroups achieved significant treatment benefits. However, studies providing adequate allocation concealment reported small mean treatment effects for pain and for physical function. Studies not reporting sufficient detail for certain, adequate allocation concealment achieved moderate mean treatment effect sizes. The difference between the 2 study subgroups was significant for both outcome measures (Table 1).
Overall estimate of bias risk: Only 9 (28%) studies could be considered low risk of bias from the published report15,17,18,20,22,30,36,41,44. All 3 study categories (low, medium, or high risk of bias) achieved significant mean treatment benefits in terms of pain and physical function. However, studies at low risk of bias demonstrated small mean treatment effects for pain and physical function. Studies at moderate or high risk of bias demonstrated mostly moderate mean treatment effects. The difference among the 3 study subgroups was significant for both outcome measures (Table 1).
DISCUSSION
Our systematic review was restricted to RCT evaluating land-based therapeutic exercise for people with symptomatic knee OA in terms of self-reported knee pain and physical function. Overall, metaanalysis demonstrated that the evaluated exercise programs resulted in a mean treatment benefit for both knee pain (SMD 0.40, 95% CI 0.30–0.50) and physical function (SMD 0.37, 95% CI 0.25–0.49). These mean treatment benefits, extrapolated from 32 RCT recruiting almost 3800 participants, would be considered small. The magnitude of treatment benefit is, however, comparable to reported estimates for current simple analgesics and NSAID taken for knee pain47. If the metaanalysis is restricted to those 9 RCT evaluated as having a low risk of bias, land-based therapeutic exercise demonstrated smaller but still significant benefits in terms of knee pain (SMD 0.28, 95% CI 0.15–0.42) and physical function (SMD 0.25, 95% CI 0.13–0.38).
Due to marked heterogeneity between the content of evaluated exercise programs in the included RCT, sensitivity analyses could only meaningfully be conducted according to fairly crude exercise program characteristics: the mode of treatment delivery and the number of directly supervised treatment occasions. While these subgroups analyses are nonrandomized comparisons and should therefore be viewed as being exploratory, there were some interesting findings. While RCT assessing home programs demonstrated effects for pain and physical function that were consistently smaller than those using more closely supervised forms of treatment delivery (individual treatments or class-based programs), the difference between the various treatment delivery modes did not reach statistical significance. This nonsignificant finding is likely to reflect the incorporation of regular home or clinic visits by trained health professions into several of these “home” programs13,22,33,41. In fact, the magnitude of the treatment benefit demonstrated by the RCT included in this metaanalysis was significantly influenced by the number of directly supervised occasions provided within a program.
Exercise “dosage” is a factor of frequency, intensity, and program duration and varies considerably between the studies included in this systematic review. Uncertainties in actual dosage arise due to the dependence of exercise intensity not only upon exercise prescription but also upon individual exertion. The influence of program duration upon dosage is difficult to quantify, with simple addition not providing a sufficiently physiological, plausible model. None of the included studies attempted to evaluate the influence of exercise dosage. Further, there were insufficient studies with comparable exercise program content to provide a meaningful subgroup analysis of the influence of exercise dosage on treatment effectiveness. Specific recommendations cannot, therefore, be made about optimal dosage (frequency, intensity, duration).
To reduce the risk of bias in a clinical trial, apart from adequate allocation concealment and limited loss to followup, blinding of therapists, study participants, and outcomes assessors is recommended. This approach provides the best protection that trial results will be free of selection, performance, attrition, and detection bias. Blinding of therapists and study participants is arguably impossible to achieve in studies evaluating exercise programs. Using “sham” exercise as the control intervention is fraught with ethical concerns (substantial wasted time for control participants attending an ineffective program) and is likely to be fairly transparent to the majority of people with knee OA. Therefore, a slight modification to the usual methodological criteria has been used in this systematic review. Within the blinding criteria, only blinding of outcomes assessment was required. It is of concern, therefore, that only 18 (56%) of the included RCT reported using blinded outcomes assessment; only 14 (43%) studies used an intention-to-treat analysis; and only 15 (47%) studies reported adequate allocation concealment. Not unexpectedly, the 9 studies evaluated as having a low risk of bias by fulfilling all 3 methodological quality criteria demonstrated significantly smaller mean effect sizes for pain and physical function compared with the studies evaluated as having moderate or high risk of bias (Table 1).
There are some important caveats to this review. The first concerns the responsiveness of self-reported pain and physical function. Many of the studies included in this systematic review included mostly participants with early or mild symptomatic disease. Although people with early disease frequently demonstrate reduced muscle strength and aerobic capacity compared with their age and sex peers without symptomatic OA, these physiological impairments are often not yet large enough to translate into reportable difficulties on simple questionnaires. This lack of reportable difficulties would considerably reduce the potential range of improvement possible (ceiling effect) on self-report questionnaires in people with early or mild disease. One of the potential benefits of exercise in people with early disease, such as increasing physiological reserve capacity, will not be identified by these questionnaires. Objective measures of physical performance not only strengthen the methodological quality of a study where masking to allocation is unattainable for the participant, but also potentially provide data better able to discriminate between people with early disease, where disease-related impairments have not yet developed into self-reported functional limitations or disability. Second, regular exercise provides general health benefits beyond reducing joint symptoms. This review is, therefore, likely to be underestimating the overall beneficial effect of exercise among people with knee OA.
Most people with knee OA have a pattern of chronic, fluctuating symptoms. Longterm adherence to exercise, or increased leisure-time physical activity, is required to maintain the benefits of exercise. Adherence to therapeutic exercise, however, usually requires the stimulus of regular supervision or monitoring48. Unfortunately, most individuals or healthcare systems do not have sufficient resources to allow ongoing unrestricted access to individually provided treatments for chronic musculoskeletal conditions. This systematic review could not establish a significant difference in treatment benefits, in terms of knee pain or physical function, between studies assessing individual treatments, class-based programs, or (usually closely individually monitored) home programs. It could, however, be argued that the class-based format potentially provides a cost-effective alternative that could be more regularly accessed by older people when introduced to community centers or gymnasiums; and that the social contact with peers, particularly those experiencing similar disease-related symptoms, is highly likely to encourage treatment adherence.
There is evidence that land-based therapeutic exercise has a benefit in terms of reduced knee pain and disability for people with knee OA. This is supported by our systematic review that includes at least 2 individual controlled trials, each with sample sizes of at least 50 per group and satisfying methodological quality criteria49. People with painful knee OA can be reassured that therapeutic exercise (individual treatments, exercise classes, or monitored home program) provided by a physiotherapist or trained health professional has the real potential to reduce, at least for the short term, their knee pain and physical disability. The magnitude of treatment benefit is likely to be associated with the number of direct supervision occasions provided.
APPENDIX. Medline search strategy

Footnotes
-
Dr. Fransen was supported by a National Health and Medical Research Council Career Development award.
- Accepted for publication January 30, 2009.








{kind=link}
{kind=link}