

Abstract
Objective. To establish thresholds for rheumatoid arthritis (RA) activity categories according to the RA Disease Activity Index-5 (RADAI-5).
Methods. Three hundred ninety-two patients with RA were categorized according to Disease Activity Score 28-joint count (DAS28), Clinical Disease Activity Index (CDAI), and their satisfaction (PATSAT) with disease status. These measures built the basis for the calculation of disease activity limits for the RADAI-5. Patient assessments simultaneously meeting the identical DAS28, CDAI, and PATSAT categories were taken as the references to establish the thresholds for the respective RADAI-5 categories by calculating the third quartile of the corresponding RADAI-5 values. Subsequently, these new thresholds were applied to all assessments.
Results. Seven hundred fifty-eight assessments in 392 patients (2 assessments median/patient) could be obtained, most patients having mild to moderate disease according to DAS28 and CDAI. Calculating the third quartile, the RADAI-5 thresholds were as follows: 0.0–1.4 for a remission-like state, 1.6–3.0 for mild disease activity, 3.2–5.4 for moderate, and 5.6–10.0 for high disease activity. Categorization according to the RADAI-5 showed a normal distribution, while DAS28 and CDAI were somewhat shifted to the left. DAS28 and CDAI levels, as well as tender and swollen joint counts and physician’s global assessment and erythrocyte sedimentation rate, proved to be highly significantly different within the different RADAI-5 categories (Kruskal-Wallis test p < 0.001).
Conclusion. RADAI-5 thresholds for RA activity could be elaborated. Patient self-report questionnaires may substitute composite disease activity scores and may contribute significantly to improving documentation in routine patient care.
- RHEUMATOID ARTHRITIS
- RHEUMATOID ARTHRITIS DISEASE ACTIVITY INDEX-5
- DISEASE ACTIVITY ASSESSMENT
- DAILY ROUTINE
Valid measurement tools are a necessity for disease activity assessment in patients with rheumatoid arthritis (RA) in daily routine care. Important prerequisites of valid instruments are their feasibility as well as easy applicability. It can be anticipated that assessment of patients applying valid tools, regardless of composite indexes or patient questionnaires, would result in better patient outcome. Nevertheless, most physicians unfortunately do not use disease activity assessment tools in daily practice1.
Almost all composite disease activity scores, like the Disease Activity Score (DAS28)2 or the Clinical Disease Activity Index (CDAI)3 use a 28-joint count requiring experience in joint assessment. We recently published a 5-item questionnaire — the RADAI-54, a modification of the Rheumatoid Arthritis Disease Activity Index — for patient-centered RA activity assessment. The RADAI-5 omits the patient self-assessed tender joint count (TJC) of the original RADAI5. The background for doing so was to provide physicians, particularly the non-rheumatologist, who may not be that familiar with joint assessment, with an instrument to assess RA activity in daily routine care. The RADAI-5, a completely patient self-administered tool, was shown to be capable of measuring RA activity accurately when compared to the DAS28 and the CDAI. Moreover, its reliability and convergent validity could be documented4.
To date, thresholds for disease activity categories have not yet been defined for this instrument. Therefore, this investigation was performed to establish cutoff values for the RADAI-5 defining a remission-like state as well as mild, moderate, and high disease activity. Such thresholds have been evaluated for the composite indexes as well as for another patient self-report questionnaire, namely the Routine Assessment of Patient Index Data 3 (RAPID3)6. Disease activity categories and their respective limits are desirable to provide physicians with green, yellow, and red “flags” that enhance risk estimation for the individual patient during the disease course.
MATERIALS AND METHODS
Patients
Three hundred ninety-two outpatients with RA, all meeting the 1987 American Rheumatism Association classification criteria7, were enrolled into our study after giving informed consent. They were followed longitudinally in a hospital based rheumatology outpatient department and in a private rheumatology office. Three hundred twenty-three patients (78.3%) were women, 69 men, median age was 61 years (range 20–87), 59.4% were rheumatoid factor (RF)-positive, the median disease duration was 62 months (range 4–545). Ninety-eight percent of the patients were taking various disease modifying antirheumatic drugs (DMARD) including biologics, 74% were taking additional glucocorticoid therapy (between 2.5 and 12.5 mg prednisolone equivalent per day); 2 patients additionally received 25 mg prednisolone. All patients took nonsteroidal antirheumatic drugs at least on demand. For patient demographic data see Table 1.
Patients’ characteristics, medians and range, unless otherwise indicated.
Calculation of the RADAI-5 disease activity thresholds
During the waiting period the patients were asked to complete the RADAI-5 questionnaire. If necessary a short instruction was given by a nurse. The questionnaire was completed by the patient without influence by a third person. In addition, the patients were asked to rate their satisfaction with the disease status (PATSAT) according to the Austrian school mark system from 1 to 5 (1 = excellent, 2 = good, 3 = average, 4 = adequate, and 5 = unsatisfactory). The Austrian school mark system resembles a Likert scale and is well established and therefore misinterpretation by the patient is very unlikely8. The purpose of this procedure was to obtain a second patient-dependent measure to define disease activity.
A 28-joint count for tender and swollen joints was performed by experienced joint assessors in the outpatient department (BR, PMH, JS, CD) as well as in the private practice (BFL). Additionally, patient’s global assessment of the disease status (PATGLOB) on a 100-mm visual analog scale (VAS) and the erythrocyte sedimentation rate (ESR, 1st h) were recorded to calculate the DAS282. Physician’s global assessment (MDGLOB) on a 10-cm VAS was also recorded to enable calculation of the CDAI3.
Subsequently, patients were classified according to the DAS28 and CDAI thresholds for remission or mild, moderate, or high disease activity. Further, patients were classified according to their PATSAT in 4 categories, where PATSAT 1 represents remission-like state, 2 represents mild, 3 moderate, and 4 and 5 high disease activity. We found it justified to integrate PATSAT 4 and 5 into 1 category, since we have found patients rating their satisfaction in that way were highly active8. Patient assessments simultaneously meeting similar categories according to the DAS28, CDAI, and PATSAT were taken as references to establish the thresholds for the respective RADAI-5 categories by calculating the third quartile of the corresponding RADAI-5 values. The third quartile was chosen to eliminate outliers and to provide that 75% of the patient group fulfil the tested criterion.
Statistics
Statistical evaluation was performed using SPSS for Windows, version 11.0 (SPSS, Chicago, IL, USA). Testing for normal distribution was primarily performed applying the Kolmogorov-Smirnov accommodation. The Kruskal-Wallis test was applied to analyze differences of DAS28, CDAI, and PATSAT as well as TJC, swollen joint count (SJC), ESR, and MDGLOB, as well as in the respective RADAI-5 disease activity groups. Kappa statistics were applied to evaluate the degree of agreement between the disease activity categories according to the DAS28, CDAI, and RADAI-5. Cohen’s kappa measures the agreement between the evaluations of 2 raters when both are rating the same object9. A value of 1 indicates perfect agreement, a value of 0 indicates that agreement is not better than chance. Kappa values > 0.60 are commonly regarded as indicating a substantial relationship9,10. Since some patients were assessed repeatedly, the coefficient of variation (CV) was calculated in repeated assessments to exclude redundant results.
RESULTS
Seven hundred fifty-eight assessments in 392 different patients could be evaluated [median assessments per patient 2 (range 1–8), median interval 3 months (range 1–19)]. Repeated measurements were highly statistically significantly different as expressed by the CV (for RADAI-5, DAS28, CDAI, and PATSAT values 69.34%, 35.13%, 74.72%, and 43.87%, respectively), which indeed reflects daily routine. Patients in the private practice had significantly milder disease (p < 0.01) and were more frequently assessed than patients of the outpatient department (Table 1). Patients reported no difficulties in completing the questionnaire; the reported average time to complete the questionnaire was 50 seconds.
DAS28, CDAI, PATSAT, and RADAI-5 values were highly significantly correlated (rs between 0.624 and 0.806; p < 0.001). The median DAS28 was 3.26 (range 0.49–8.09), indicating moderate disease activity according to the DAS28 criteria2; the median CDAI was 7.25 (range 0.0–62.1) — within the mild disease activity category according to this score3; and the median RADAI-5 amounted to 2.8 (range 0.0–8.6). The median PATSAT was 2, indicating good satisfaction with disease status and mild disease activity with respect to our predefined definition. For the other evaluated RA-relevant measures, see Table 1.
Calculation of the RADAI-5 disease activity thresholds
Of all 758 assessments, 71 simultaneously met the thresholds for remission with respect to the categories according to the DAS28 and CDAI and reported a PATSAT score of 1 (in 49 patients, 32 women). The median RADAI-5 in these assessments amounted to 0.8 and the respective third quartile was 1.4. Therefore the remission-like state was defined as a RADAI-5 score ranging from 0 to 1.4. The same procedure was applied to define the limits for mild, moderate, and high disease activity, resulting in the following ranges: 1.6–3.0 for mild disease activity (on the basis of 48 assessments of 43 patients, 33 women); 3.2–5.4 for moderate activity (102 assessments of 78 patients, 69 women); and 5.6–10 for high disease activity (Table 2).
Patients’ characteristics according to the RADAI-5 disease activity categories (medians and ranges).
Application of these RADAI-5 categories to all 785 assessments
Applying these newly established RADAI-5 disease activity categories to all assessments, 182 assessments (23%) in 115 patients met the remission-like category. Two hundred thirty-four (31%, in 168 patients) assessments were categorized as mild, 224 (30%, in 167 patients) as moderate, and 118 (16%, in 87 patients) as high disease activity. As shown in Figure 1, the RADAI-5 categories very much resemble a normal distribution in contrast to the DAS28 and CDAI-categories, which are shifted to the left. Characteristics of the disease status as expressed by the core-set measures within the RA activity categories according to the RADAI-5 are shown in Table 2.

Distribution of the patients according to Rheumatoid Arthritis Disease Activity Index-5 (RADAI-5), Disease Activity Score 28-joint count (DAS28), Clinical Disease Activity Index (CDAI), and predefined patient satisfaction (PATSAT) disease activity categories.
The median DAS28 in the RADAI-5-dependent remission-like category was 2.39 (range 0.49–5.11), in the mild category 3.07 (0.49–5.69), and in the moderate category 3.83 (0.88–5.96), all 3 meeting the corresponding DAS28 thresholds. In the RADAI-5-dependent high disease activity category the median DAS28 amounted to 4.65 (range 1.33–8.09), which is apparently below the respective high disease activity threshold. An identical situation was found for the respective CDAI values: they were 2.8 (range 0.0–20.5), 6.5 (0.0–25.4), 10.2 (1.1–35.4), and 16.5 (0.5–62.1), respectively.
DAS28 and CDAI levels corresponding to the RADAI-5 categories appeared to be highly statistically significantly different (p < 0.001). Not only the composite indexes’ values, but also tender and swollen joint counts proved to be highly significantly different within the RADAI-5-dependent categories (p < 0.001) according to the Kruskal-Wallis test (Figure 2), which also holds true for MDGLOB (p < 0.001) and the ESR (p < 0.001) (Table 2).
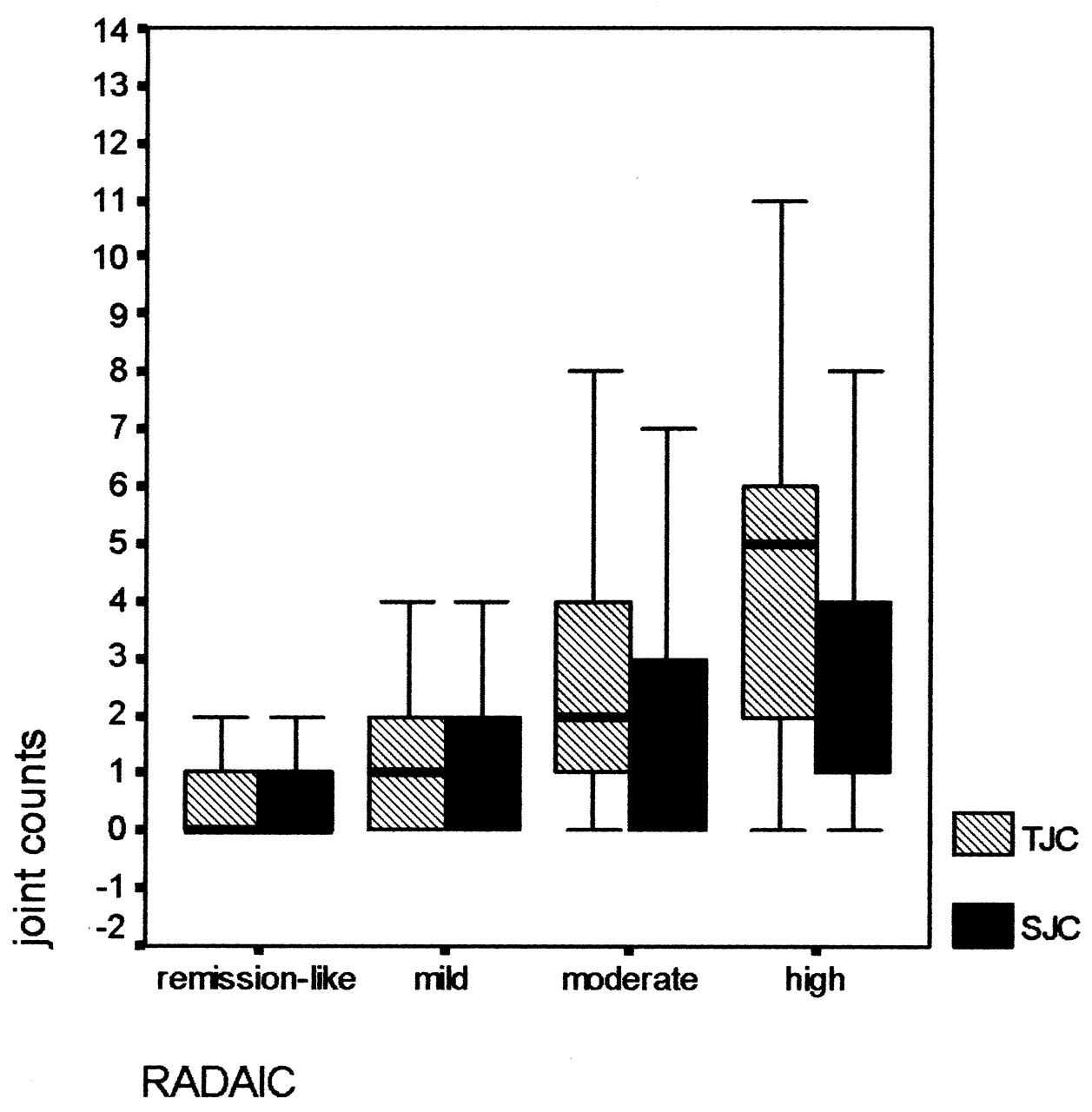
Tender and swollen joint counts (TJC and SJC) within the 4 RADAI-5-dependent disease activity categories (p < 0.001, Kruskal-Wallis test).
Applying kappa statistics for agreement analysis between the disease activity categories according to the 3 different tools revealed a statistically significant result. However, the relationships between the RADAI-5-dependent categories and the respective DAS28 and CDAI categories were only fair (kappa 0.236; p < 0.001 and 0.280; p < 0.001, respectively). Agreement between the DAS28 and CDAI-dependent categories was moderate, as expressed by a kappa of 0.410 (p < 0.001). Kappa for the relationship between PATSAT and the RADAI-5 categories was 0.490 (p < 0.001), also indicating moderate agreement.
In 69 assessments (9.1% of all assessments, 37.9% of remission according RADAI-5) or in 49 patients (12.5% of all patients, 42.6% of patients meeting remission according to RADAI-5) remission-like disease activity is expressed by RADAI-5 and DAS28 as well as by CDAI values. In these patients the median PATSAT amounted to 1 (range 1–2). For the other categories and patients’ characteristics, see Table 3.
Assessments and patients meeting the same disease activity category according to RADAI-5, DAS28, and CDAI.
DISCUSSION
To enhance applicability in daily routine care it was deemed necessary to establish thresholds for the recently presented RADAI-5 to allow the categorization of patients with RA. Commonly, patients with RA are classified as in “remission-like state” or as having mild, moderate, or highly active disease. Translating those categories into current routine care, the clinical remission-like state corresponds to a green flag, the mild disease activity category to a yellow one, and adequate as well as high disease activity agrees with a red flag situation, which should be clarified as soon as possible — meaning reconsidering the patient’s management and taking action. Since the RADAI-5 is calculated by addition of 5 integral numbers from 0 to 10 of a numerical rating scale, followed by a division by 5, its result has to have a 1-digit even number as first decimal. Derived from this observation, the following thresholds are proposed for patient categorization: 0.0–1.4 for a remission-like state, 1.6–3.0 for mild disease activity, 3.2–5.4 for moderate, and 5.6–10.0 for high disease activity.
These thresholds were established assessing patients of a rheumatology outpatient department and a private practice. The patients with RA included in our study represent a broad spectrum, from early RA with disease duration from at least 3 months to longstanding disease of up to 545 months. Patients from the private practice had milder disease and were assessed more often than those in the out-patient department. As also indicated by the CV for repeated measures, disease activity fluctuations occurred in single patients, mirroring daily rheumatologic practice.
The limits for the RADAI-5 categories were developed under rigorous criteria: it was necessary to meet not only the DAS28 criteria, but also — for remission — the more stringent CDAI criteria11. In addition, PATSAT as an exclusively patient-dependent measure was included as a reference. As a proof for the requested stringency, only 49 assessments simultaneously met the criteria to be primarily classified as in a “remission-like state.”
The composite indexes taken as references (DAS28 and CDAI) comprise selective measures such as ESR, PATGLOB, TJC, and SJC or MDGLOB, resulting in a score representing actual disease activity at the time of investigation (“on spot”). In contrast, the RADAI-5 assessment addresses not only current RA activity (tenderness and swelling of the joints, pain, and morning stiffness) and patient’s general health, but also asks for “arthritis activity during the last 6 months” (question 14,5). Hence, the RADAI-5 value is also influenced by the course of the disease and cannot be regarded as merely “snapshot-like,” as the composite indexes are; in our opinion, this constitutes an important factor in a chronic disorder. The longterm perspective may be one of the reasons for the more normal distribution of the RADAI-5 categories compared to the respective DAS28 or CDAI-dependent ones, and may explain the “only fair” agreement between the RADAI-5 categories and those of the composite indexes. Another reason for the DAS28 and CDAI categories’ shift to the left may be provided by the lower numbers of patients experiencing high disease activity according to the respective indexes. Since remission in particular cannot be seen as an instantaneous aspect of the disease, but by definition has to be a stable condition for at least 2 months12,13, the inclusion of the time factor constitutes a substantial advantage of the RADAI-5 questionnaire. Recently, a shortening of the timeframe of the original RADAI of 6 months was discussed14, which could result in a higher percentage of patients categorized in a remission-like state. However, we do not regard such discussions as essential in light of the results obtained here.
A remission-like state and above all, stable remission, according to the RADAI-5, definitely mean something different from remission according to the DAS28 or CDAI. To highlight this, consider the following example: a patient with flaring RA and a DAS28 of 5.82 (TJC 8, SJC 6, ESR 35 mm/h, VAS for global health 75) is prescribed 25 mg prednisolone daily and 2 weeks later is reassessed, with a good response, resulting in a DAS28 of 2.59 (TJC 0, SJC 1, ESR 20, VAS global health 15). Does this DAS28 really reflect remission? Because of question 1, a result meeting the RADAI-5 remission-like state cannot be expected after 2 weeks.
As noted, the distribution of the disease activity categories differed depending on the particular instruments. The RADAI-5-dependent ones very much showed a normal distribution, while the DAS and CDAI-dependent ones were shifted somewhat to the left, with a reasonably lower number of patients experiencing high disease activity. An important factor possibly exerting an influence on the distribution of disease activity categories could be the clinical status of the patients — median TJC of 1, swollen joint count of 1, ESR of 16. This may also explain why the DAS and CDAI curves were shifted to the left, and it could be that RADAI-5 scores overestimate the impression of the level of inflammation. However, if this is true, it would suit the RADAI-5 even better to be applied as an alerting instrument.
At first sight, the limit for “remission” according to the CDAI may seem to be more stringent, compared to the RADAI-5. However, this is more than outweighed by the high number of mild disease activity assessments resulting from application of the CDAI. As expected, far more patients could be categorized as being in remission according to the DAS28; moreover the vast majority of patients were found to have moderate disease activity (Figure 1).
Of course, the patient’s perspective of the disease could be determined more accurately by applying a patient self-assessment tool. Instruments such as the Health Assessment Questionnaire (HAQ)15 and its derivatives as well as the RAPID36 are well known to possess predictive value for the disease course, for functionality and even mortality. Further studies are warranted to investigate the RADAI-5 in these respects. In any case, patient-administered tools can be expected to reveal patients’ attitudes with respect to treatment decisions better than composite indexes, as it is well known that patients’ and physicians’ perspectives on disease course are divergent16.
Direct joint assessment proved to be not essential for routine RA activity assessment. This was another expected, yet remarkable result of our study and is in agreement with our previous findings. Not only the DAS28 and CDAI values, but also TJC and SJC within the RADAI-5-dependent RA activity categories were highly significantly different according to the Kruskal-Wallis variance analysis. Also, the MDGLOB and even the ESR were found to be significantly different within the RADAI-5 categories. Proving to be in accord with changes of TJC and SJC reinforces the use of the RADAI-5 as a tool for RA activity assessment, particularly for physicians with less rheumatologic experience in joint assessment.
The RADAI-5 thresholds for disease activity categories presented here were elaborated in daily routine care. In a busy outpatient department or practice, particularly when carried out by a nonrheumatologist (e.g., a general practitioner), documentation of disease activity is as necessary as in clinical trials17. Unfortunately, to date, patients with RA in most cases are not monitored as closely and as accurately as required18, since often not enough rheumatologists are available19. For high quality RA patient care, not only treatment as early as possible, with monitoring as closely-matched as possible18, but also monitoring tools that are as accurate as possible are mandatory20.
Self-report questionnaires, such as the RADAI-5, have been shown capable of substituting for physician-derived disease activity scores, which were developed primarily for research purposes21. Both the RADAI-5 and the RAPID3 have been designed specifically for busy clinical settings4,6, with attention not only to validity and reliability, the primary criteria for any questionnaire, but also to feasibility and acceptability. Both refrain from formal joint counts and therefore both require minimal costs and professional time, which should contribute to their acceptability by practicing physicians22. It takes less than 10 seconds to calculate the RADAI-5. This self-report questionnaire has proven to be in accord with more time-consuming tools such as the DAS2823 or the CDAI. The proposed limits for disease activity categories should enhance the use of this tool in future, e.g., by general practitioners, providing them with an alerting instrument for RA monitoring. A better and more uniform way of documenting the individual patient’s disease should ultimately result in improved routine rheumatology patient care.
Acknowledgments
We thank DGKS Gerlinde Ramharter, DGKS Elisabeth Hagmann, and Monika Weiskirchner for collaboration on distributing the questionnaires to patients and instructing patients how to complete them without influencing their answers.
Footnotes
- Accepted for publication December 16, 2008.








{kind=link}
{kind=link}