

Abstract
Objective. To investigate whether the achievement of inactive disease in the first 5 years predicts a more favorable outcome of children with juvenile idiopathic arthritis (JIA).
Methods. We reviewed clinical charts of 123 patients who started taking methotrexate, were followed for at least 5 years, and received a yearly assessment in the first 5 years. At each yearly visit, the presence of inactive disease was assessed. Patients were divided into 3 groups: (1) patients who never reached inactive disease; (2) patients who reached inactive disease in only 1 visit; and (3) patients who reached inactive disease in ≥ 2 visits. Outcome was evaluated after 6 to 18 years (median 7.1 yrs) by assessing the following clinical measures: restricted joint count, Childhood Health Assessment Questionnaire (CHAQ), Juvenile Arthritis Damage Index (JADI), and Poznanski score of radiographic damage.
Results. In the first 5 years, 62 patients (50.4%) were noted to have active disease at their yearly visit, 40 patients (32.5%) were noted to have inactive disease only once, and 21 patients (17.1%) were noted to have inactive disease in ≥ 2 visits. Patients who achieved inactive disease 1 or more times had lower restricted joint count (p = 0.007) and JADI-Articular score (p = 0.004) at last followup visit than those who never reached such a state. A similar trend, although not significant, was observed for CHAQ and Poznanski score of radiographic damage.
Conclusion. Attainment of the state of inactive disease at least once in the first 5 years was found to be associated with less longterm joint damage and with a trend toward less functional impairment.
- JUVENILE IDIOPATHIC ARTHRITIS
- JUVENILE RHEUMATOID ARTHRITIS
- JUVENILE CHRONIC ARTHRITIS
- INACTIVE DISEASE
- REMISSION
- LONGTERM OUTCOME
- PHYSICAL DISABILITY
- RADIOGRAPHIC ASSESSMENT
Juvenile idiopathic arthritis (JIA) is a heterogeneous entity that is diagnosed with reference to the International League of Associations for Rheumatology (ILAR) classification criteria1. The clinical course of JIA is variable and its prognosis is difficult to predict2. In many patients the disease follows a benign and self-limiting course, whereas in others the disease process is severe and unremitting and results in progressive joint destruction and serious disability3. However, outcomes vary widely4–6.
In recent years, the expectation of benefit of treatment of children with chronic arthritis has evolved. With the shift towards early aggressive therapeutic interventions and the advent of the novel potent biologic medications, disease remission is now a goal for many pediatric rheumatologists7–9. Although this objective has been easier to achieve in children with oligoarthritis who are treated with only intraarticular corticosteroids, it is still problematic in the subset of patients who have polyarticular disease. A recent analysis of 437 patients with JIA (excluding those treated with intraarticular injections alone) followed for at least 4 years or more showed that as many as 89% of the patients experienced one or more episodes of inactive disease and 44% of the patients achieved the state of clinical remission without medication. However, the latter state was not found to be durable, with only 58% of the episodes of inactive disease being sustained over 1 year and a small proportion (6%) sustained over 5 years8.
Studies in adult patients with rheumatoid arthritis have shown that cumulative disease activity is associated with the degree of joint destruction and functional impairment10–12. It is now well established that minimizing disease activity over time reduces radiographic progression and improves functional outcome13,14. In JIA, the relationship between the time course of disease activity and the longterm outcome has seldom been evaluated. In a previous study, we found that a greater magnitude of clinical response in the first 6 months of methotrexate (MTX) therapy was associated with a greater improvement in joint disease and a higher frequency of inactive disease at 5 years in children with polyarticular JIA15. In another analysis, the area under the curve of joint disease activity in the first 5 years was found to be significantly correlated with the amount of clinical and radiographic articular damage at last followup assessment (Magnani, et al: unpublished observation).
Our aim was to investigate whether achievement of the inactive disease state in the first 5 years after first observation predicts a more favorable outcome of JIA patients with polyarthritis.
MATERIALS AND METHODS
Patient selection.
We reviewed the clinical charts of all consecutive patients who had JIA by the ILAR criteria1, had a polyarticular course of arthritis, started taking MTX therapy at the study units between November 1986 and February 2002, had a followup of at least 5 years after the first observation, and had received a yearly visit from first observation to 5 years. Yearly visits were defined as visits 12 ± 3 months apart, starting from first observation. The 5-year cutoff was chosen arbitrarily: it was felt that the first 5 years of disease could represent an appropriate period of time to assess the effects of the achievement of clinical remission on the development of longterm functional and structural damage. All patients seen before the publication of the ILAR criteria for JIA were reclassified using such criteria. Because there were relatively few patients with the ILAR categories of rheumatoid factor-positive polyarthritis, psoriatic arthritis, and undifferentiated arthritis, for the purposes of the analysis patients with these JIA subtypes were classified within the polyarthritis and extended oligoarthritis categories based on the number of joints affected in first 6 months of disease.
The criterion of MTX administration was chosen to identify patients seen in the study units who carried the greatest risk of poor outcome. In the study period it was the authors’ policy to use MTX as drug of first choice in all JIA patients with polyarthritis who failed to respond to a course of nonsteroidal antiinflammatory drugs. Therefore, the study population likely included all the most severe cases of JIA who were at risk of experiencing joint destruction and permanent functional disability. Patients were included in the study if they had started MTX at any time during the disease course.
The design of the study was approved by the independent Institutional Review Board of the Gaslini Institute, Genoa, Italy.
Baseline clinical and radiographic assessment.
Patient information recorded at first observation included onset age, sex, ILAR category, and disease duration. The following clinical and radiographic assessments made at first observation were also recorded: physician’s global assessment of the overall disease activity measured on a 10-cm visual analog scale (VAS; 0 = no activity; 10 = maximum activity); parent’s global assessment of the child’s overall well-being on a 10-cm VAS (0 = very good; 10 = very poor); parent’s rating of the intensity of the child’s pain on a 10-cm VAS (0 = no pain; 10 = very severe pain); count of joints with swelling, tenderness/pain on motion, and restricted motion and count of joints with active disease (i.e., joints with swelling or, if no swelling was present or detectable, with restricted motion and either pain upon movement or tenderness)16; functional ability assessment through the Italian version of the Childhood Health Assessment Questionnaire (CHAQ)17 (0 = best; 3 = worst) or, in the years before 1994 (when the CHAQ was published), through the Modified Lee Index18 or the Juvenile Arthritis Functional Assessment Report (JAFAR)19 (we previously found a high correlation between these 3 questionnaires when administered to the same patient on the same day16; for this reason, scores of the 2 latter instruments were proportionally converted to the 0–3 score of the CHAQ); erythrocyte sedimentation rate (ESR; Westergren method); C-reactive protein (CRP; nephelometry); and, in patients with wrist involvement, Poznanski score of radiographic damage20,21. Briefly, the Poznanski score is based on measurement of the radiometacarpal length (RM), the distance from the base of the third metacarpal bone to the midpoint of the distal growth plate of the radius, and of the maximal length of the second metacarpal bone (M2). For each wrist, the number of standard deviations (SD) between the expected and the observed RM for the measured M2 was calculated. The RM/M2 score, which represents the carpal length and constitutes the Poznanski score, reflects the amount of radiographic damage in the wrist. The more negative the score, the more severe the radiographic damage; a score < –2 units was considered abnormal. For each pair of wrists, the mean score was used in the analyses. All radiographs were read by an investigator (FR) who had specific experience in the assessment of Poznanski score. We previously found a very high interobserver and intraobserver reliability with this method21.
For each patient, the time interval between disease onset and first observation and between disease onset and start of MTX therapy, the duration of MTX therapy in the first 5 years after first observation, and the antirheumatic drugs other than MTX taken in the first 5 years after first observation were recorded. In the study period, it was the policy of the study investigators to start MTX therapy in all patients at the standard dose of 10 mg/m2/week.
Assessment of inactive disease.
At each yearly visit in the first 5 years after first observation, the presence of inactive disease was assessed through the preliminary definition of clinical remission in JIA7. Inactive disease was defined as simultaneous presence of the following criteria: (1) active joint count = 0; (2) physician’s global assessment = 0; (3) absence of systemic symptoms (i.e., fever, rash, hepatosplenomegaly, generalized lymphadenopathy, serositis); (4) no active uveitis; and (5) negative acute-phase reactants (ESR or CRP or both, if both were tested). Patients who had one of criteria 1, 2, and 5 not assessable due to lack of the related measure in the clinical chart were considered as having inactive disease if both remaining criteria were met. Gathering this information was facilitated because in the study period it was the investigators’ policy to make a standardized quantitative assessment of the disease status in each patient every 6 to 12 months16. Based on achievement of the state of inactive disease, patients were divided in 3 groups: (1) patients who never reached inactive disease; (2) patients who reached inactive disease in only 1 visit; and (3) patients who reached inactive disease in 2 or more visits. In patients in group 3, inactive disease could be present in either consecutive or nonconsecutive visits.
Assessment of disease outcome.
In each patient, disease outcome was evaluated by recording the following clinical assessments made at last followup visit: count of joints with restricted motion, CHAQ, Poznanski score of radiographic damage, and Juvenile Arthritis Damage Index (JADI)22. Briefly, the JADI is composed of 2 parts, one devoted to assessment of articular damage (JADI-A) and one to assessment of extraarticular damage (JADI-E). In the JADI-A, 36 joints or joint groups are assessed for the presence of damage and the damage observed in each joint is scored on a 3-point scale (0 = no damage; 1 = partial damage; 2 = severe damage, ankylosis, or prosthesis). In individual joints, contractures and other joint deformities are scored only when they are completely explained by prior damage, are not due to currently active arthritis, and are present for at least 6 months. The maximum total score is 72. The JADI-E includes 13 items in 5 different organs/systems. Extraarticular damage is defined as persistent change in anatomy, physiology, pathology, or function, which may occur since the disease presentation, may result from previous disease activity or its treatment, and is present for at least 6 months. Each item is scored as 0 or 1 if damage is absent or present, respectively. Due to the relevant effect of ocular damage on the child’s health, for each eye a score of 2 is given in case the patient has had ocular surgery and a score of 3 in case the patient has developed legal blindness. The maximum total score is 17.
Statistics.
Descriptive statistics were reported in terms of medians and quartiles and non-outlier ranges for continuous variables and in terms of absolute frequencies and percentages for categorical variables. Outliers were defined as the values that lie outside the interval (calculated as ± 1.5 × box length) drawn from the upper and lower values of the box. Comparisons of quantitative variables among groups were made by means of the nonparametric analysis of variance (Kruskal-Wallis test); Dunn’s test was chosen as a posteriori test to assess the statistical significance of differences between pairs of patient groups. Comparison of qualitative data was by chi-squared test, or Fisher’s exact test in case of expected frequencies less than 5. Bonferroni’s adjustment was applied as a correction for multiple comparisons to explore post-hoc differences between pairs of patient groups.
Multivariate logistic regression was applied to explore in more depth the potential predictors of achievement of inactive disease identified with the univariate tests. The following 2 outcomes were assessed with multivariate tests: (1) patients who never achieved inactive disease versus patients who achieved inactive disease in 1 visit or in 2 or more visits, and (2) patients who achieved inactive disease in 2 or more visits versus patients who never achieved inactive disease or achieved inactive disease in 1 visit. The following explanatory variables were entered in the 2 models: ILAR category (polyarticular/systemic/oligoarticular extended), swollen joint count (> 4/ ≤ 4), tender joint count (> 2/ ≤ 2), active joint count (> 5/ ≤ 5), interval from first to last observation (> 8/ ≤ 8 yrs), duration of MTX therapy (> 4/ ≤ 4 yrs), and cyclosporine treatment during the first 5 years of followup (yes/no). Quantitative predictors were dichotomized according to the best threshold obtained from the receiver-operating characteristic (ROC) curve analysis. Statistical significance of the variables in the models was tested by means of the likelihood ratio test. All statistical tests were 2-sided; a p value less than 0.05 was considered statistically significant. The statistical package Statistica (StatSoft Corp., Tulsa, OK, USA) was used for univariate analyses and Stata release 7 (Stata Corp., College Station, TX, USA) for multivariate analyses.
RESULTS
Of the 237 patients with JIA who started taking MTX in the study period, 123 had a followup of at least 5 years and had received a yearly assessment from first observation to 5 years, and so were eligible for the study. A total of 114 patients were excluded because they had a followup shorter than 5 years (n = 88) or did not have the yearly assessments or the minimum set of variables required to assess the state of inactive disease (n = 26). At the time of first observation at the study center, the clinical features of patients included and excluded were comparable, with the sole exception of a higher physician’s global assessment value in excluded patients (Table 1).
Comparison of baseline clinical features between patients included and not included in the study. Values are medians (first and third quartiles) unless otherwise indicated.
Assessment of inactive disease.
In the first 5 years after first observation, 62 patients (50.4%) were observed not to have inactive disease at their yearly visit, 40 patients (32.5%) were observed to have inactive disease only once, and 21 patients (17.1%) were observed to have inactive disease in 2 or more visits. Table 2 compares clinical features at first observation among the 3 patient groups. All clinical features were comparable, with the exception of a higher swollen, tender, and active joint count in patients with ≥ 2 episodes of inactive disease than in patients with 1 episode of inactive disease. Patients who never achieved inactive disease had more frequently received cyclosporine therapy, compared with patients who had achieved inactive disease on 2 or more occasions. There was a nonsignificant trend toward a longer duration of MTX in patients who had not reached the inactive disease state. The time intervals between disease onset and first observation at the study centers and between disease onset and start of MTX therapy were comparable among the 3 study groups. Multivariate logistic regression analysis (Table 3) confirmed that lack of achievement of inactive disease was associated with a greater likelihood of cyclosporine administration and with longer MTX therapy, and that achievement of inactive disease in 2 or more visits was associated with a higher swollen joint count at baseline.
Baseline clinical features, followup duration, and antirheumatic medications among patients who achieved or did not achieve the state of inactive disease in the first 5 years after baseline. Values are medians (first and third quartiles) unless otherwise indicated.
Best-fitting models of logistic regression analysis.
Assessment of outcome.
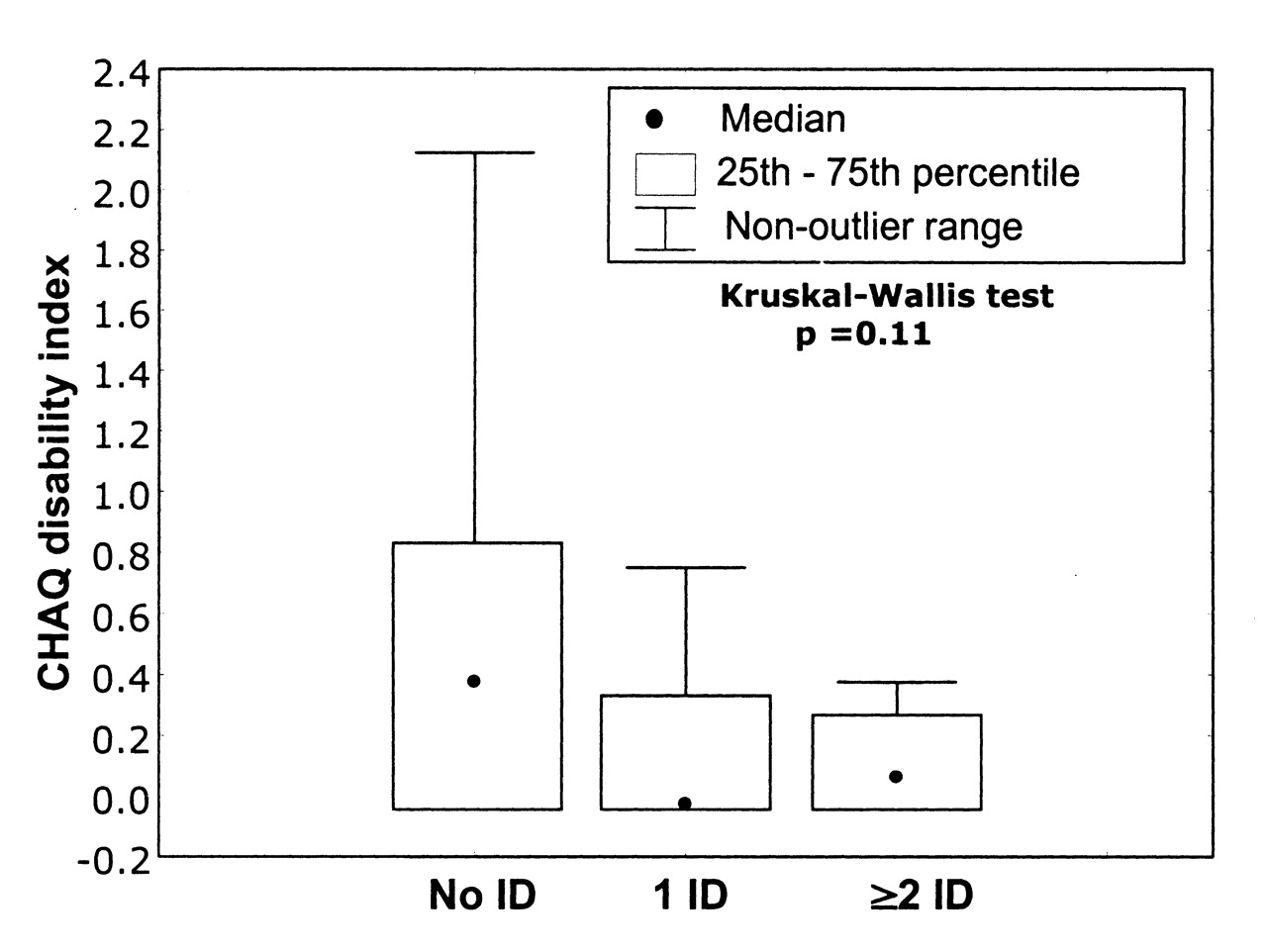
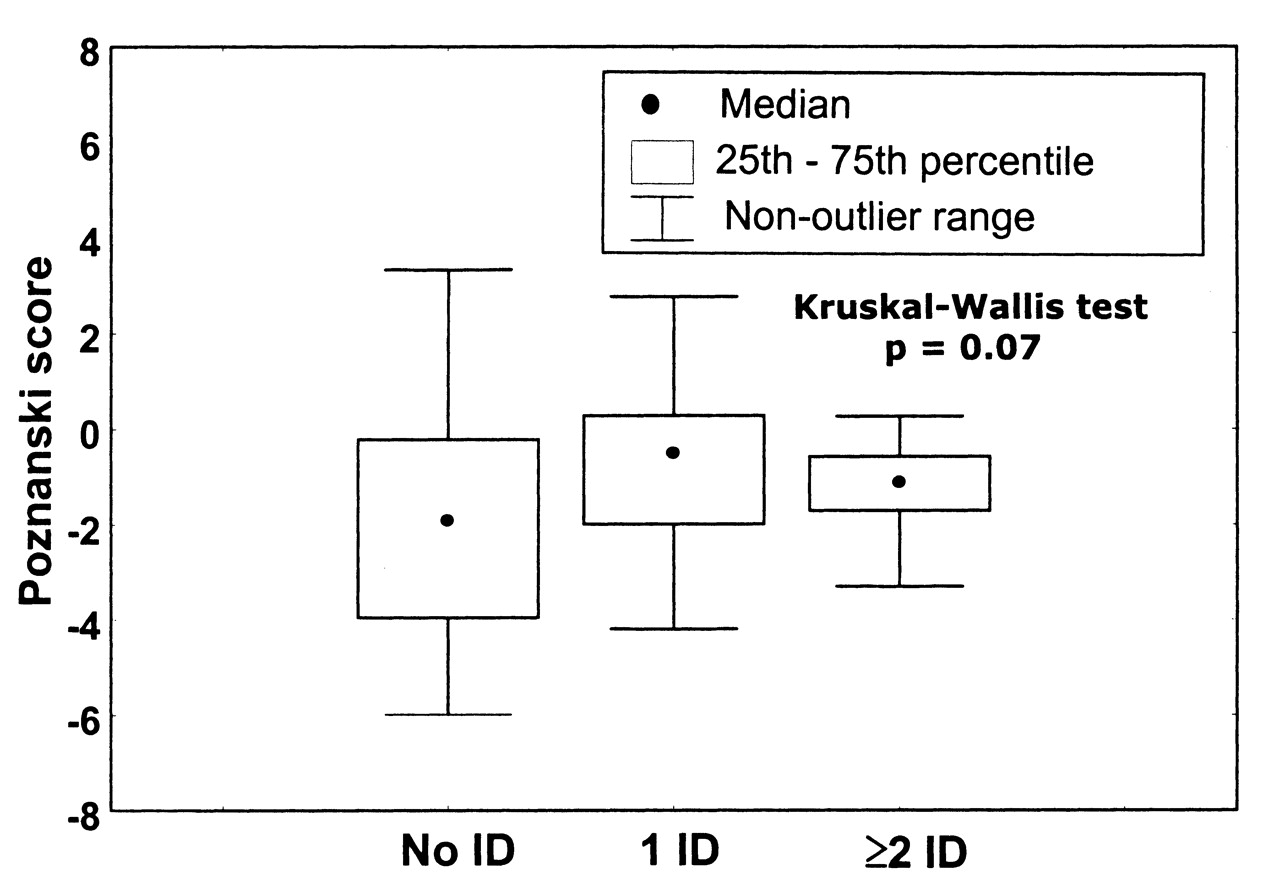
Figures 1 to 4 show the comparison of the restricted joint count, the CHAQ score, the JADI-A score, and the Poznanski score of radiographic damage in the 3 patient groups at last followup visit, 6 to 18 years (median 7.1 yrs) after first observation. Patients who achieved the state of inactive disease 1 or more times in the first 5 years had a lower restricted joint count (p = 0.007) and JADI-A score (p = 0.004) at followup observation than those who never entered such a state. A similar trend (not significant) was observed for the CHAQ score and the Poznanski score of radiographic damage. It is notable that the amount of joint damage, as measured with the JADI-A score, was significantly lower in patients who achieved the state of inactive disease 2 or more times in the first 5 years than in patients who entered such state only once. Although the duration of followup was longer in patients with no inactive disease than in those with 1 or more episodes of inactive disease, the difference was not significant (Table 2).

Median values (first and third quartiles) of the restricted joint count at last followup visit in patients who did not achieve (No ID), achieved only once (1 ID), or achieved 2 or more times (≥ 2 ID) the state of inactive disease in the first 5 years after first observation.

Median values (first and third quartiles) of the Juvenile Arthritis Damage Index (JADI)-Articular at last followup visit in patients who did not achieve (No ID), achieved only once (1 ID), or achieved 2 or more times (≥ 2 ID) the state of inactive disease in the first 5 years after first observation.

Median values (first and third quartiles) of the Childhood Health Assessment Questionnaire (CHAQ) disability index at last followup visit in patients who did not achieve (No ID), achieved only once (1 ID), or achieved 2 or more times (≥ 2 ID) the state of inactive disease in the first 5 years after first observation.
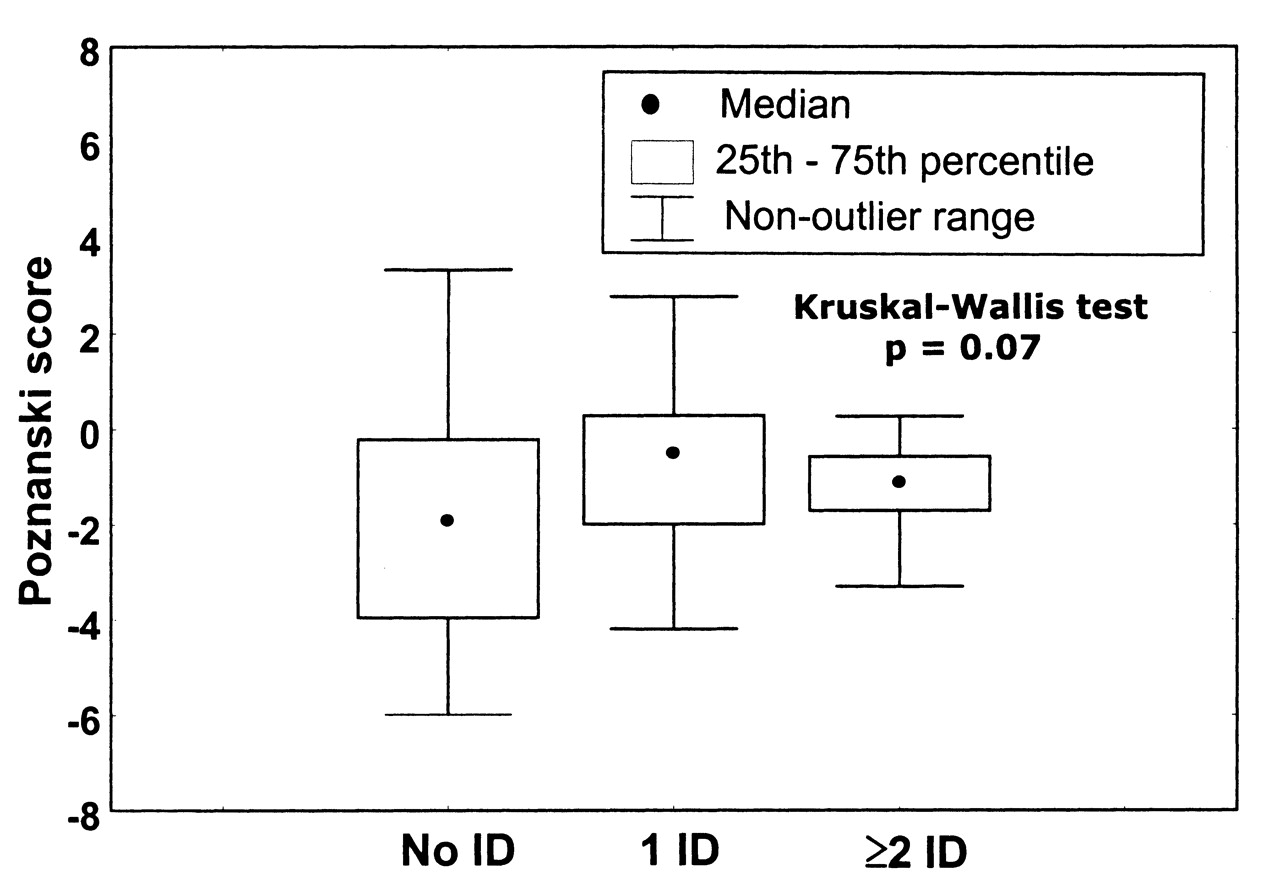
Median values (first and third quartiles) of the Poznanski score of radiographic damage at last followup visit in patients who did not achieve (No ID), achieved only once (1 ID), or achieved 2 or more times (≥ 2 ID) the state of inactive disease in the first 5 years after first observation.
DISCUSSION
The aim of our study was to investigate the relationship between the achievement of the state of inactive disease in the first 5 years and the disease outcome in 123 JIA patients with polyarthritis who were candidates for treatment with MTX. Because during the study period it was our policy to start MTX in all JIA patients with polyarthritis who failed to respond to a course of nonsteroidal antiinflammatory medications, the study population is representative of the most severe cases of JIA who are given a second-line drug therapy in a tertiary care pediatric rheumatology setting.
Patients who reached the state of inactive disease 1 or more times in the first 5 years after first observation were found to have a significantly lower number of restricted joints and significantly less cumulative articular damage, as measured with the JADI, at last followup assessment (6 to 18 yrs after first observation) than those who did not. Patients who achieved inactive disease also showed a tendency toward a better outcome in terms of functional disability and radiographic damage. Patients in the inactive disease state on 2 or more yearly visits developed less cumulative articular damage than those in such a state in only 1 visit.
The clinical indicators of JIA severity at baseline were comparable across the 3 patient groups (i.e., patients who did not achieve inactive disease, patients who achieved inactive disease in only 1 visit, and patients who achieved inactive disease in 2 or more visits), with the sole exception of difference in the swollen, tender, and active joint counts, which were, however, higher in patients who experienced a more benign course. This indicates that both the disease course and the outcome could not be predicted by the baseline features. This observation is in keeping with our previous finding that the potential for progression or therapeutic response that the disease displays in its early stages may be more important in predicting longterm outcome than the clinical characteristics at onset15. The patient groups were also comparable for the time interval between disease onset and first observation and between disease onset and start of MTX treatment, and they were all started with the same initial MTX dose. The greater frequency of adjunctive cyclosporine therapy and the longer duration of MTX administration in patients who did not achieve inactive disease is not surprising, as patients who experience continued disease activity are more likely to receive additional or more prolonged therapeutic interventions. The relatively low frequency of etanercept administration is explained by most patients having been treated prior to the availability of biologic medications in Italy. The reason why patients with 2 or more episodes of inactive disease, who ended up with better outcome, had a greater severity of joint disease at baseline is unclear. This phenomenon might be explained by differences in the distribution of JIA subtype or in the susceptibility to therapeutic interventions between groups.
The observation that achievement of the state of inactive disease at least once in the first 5 years was associated with less longterm joint damage and functional impairment suggests that targeting remission in patients with continued disease activity through aggressive therapeutic interventions may provide a better outcome. Further, it highlights the critical need for therapies or therapeutic strategies that have the capacity to induce sustained, complete control of the disease. Another important implication of the study findings lies in the demonstration that achievement of the state of inactive disease has prognostic significance, which adds to the validity of the criteria for clinical remission in JIA7,23.
A number of potential limitations to our study must be acknowledged, the first being its retrospective and noncontrolled design. A retrospective study is subject to missing and possibly erroneous data. However, most of the data, particularly regarding JIA outcome measures (physician and parent global assessments, joint counts, functional questionnaires, etc.), were collected prospectively. It has been our policy since 1986 to make a standardized assessment of the above measures every 6–12 months in all children with JIA seen in the inpatient and outpatient units. We could not assess the importance of differences in damage and functional outcomes when inactive disease was achieved at earlier timepoints (i.e., at 6 months or at 1, 2 or 3 years) and not only at 5 years. We recognize that our decision that one of the categories of the inactive disease criteria could be missing was arbitrary and represents a violation of the original criteria set. This interpretation had to occur because of missing data in about 20% of the instances. A derivation of inactive disease criteria lacking one of its components (e.g., physician global assessment = 0) has been applied previously24. The choice of the 5-year cutoff was also made arbitrarily. Survival analysis should be carried out in future surveys to choose the optimal threshold of disease duration that needs to be assessed in outcome prediction studies. The period for patient inclusion in this study (1986–2002) reflects in large part a past era in the treatment of JIA, when low-dose MTX was the only available second-line medication whose efficacy had been demonstrated in a controlled trial2, and incorporates only in part the recent therapeutic advances, particularly the introduction of biologic response modifiers, that are likely to have much improved the control of disease activity in children with the most severe forms of JIA. Additional limitations are sampling only one visit per year for each patient, lack of assessment of length of time in remission, and lack of classification of some patients into their true JIA category. Nevertheless, our study is the first to investigate the relationship between the attainment of inactive disease and the outcome in JIA, and provides important clinical information that is useful to assess and interpret the effectiveness of the next generation of drugs proposed for use in children with JIA.
The achievement of the state of inactive disease at least once in the first 5 years after first observation was found to be associated with less longterm joint damage and functional impairment. This finding indicates that management of children with JIA should be aimed at remission7 or at least minimal disease activity25, and highlights the critical need to develop new therapies or therapeutic strategies that have the capacity to induce sustained, complete control of the disease.
Footnotes
- Accepted for publication October 7, 2008.








{kind=link}
{kind=link}
{kind=link}
{kind=link}