

Abstract
Objective. To assess the relationship between bone mineral density (BMD) and varus deformity arising from bone structural changes caused by knee osteoarthritis (OA) in postmenopausal women.
Methods. This cross-sectional study involved 135 consecutive postmenopausal female patients who had varus knee OA and a Kellgren-Lawrence grade ≥ 2. Knee radiographs were obtained with the patient standing on one leg, and subjects were classified into 3 tertile groups according to femorotibial angle, which was taken as a measure of varus knee OA severity. We also measured the 3 subangles that make up the femorotibial angle, and focused on the varus inclination of the tibial plateau. BMD was measured in the lumbar spine, femoral neck, and medial and lateral tibial condyles using dual-energy X-ray absorptiometry. Differences between femorotibial angle tertile groups were assessed, and associations between femorotibial sub-angles and BMD values at various points were evaluated.
Results. After adjustment for age and body mass index, there was no significant association between the varus inclination of the tibial plateau and lumbar spine BMD. A weak but statistically significant negative correlation existed between varus inclination of the tibial plateau and BMD at the ipsilateral proximal femur and lateral tibial condyle.
Conclusion. Varus inclination of the tibial plateau was significantly more severe in the femorotibial angle tertile 3 group, and in patients with lower BMD in the ipsilateral lower limb. Varus knee OA may result not only from cartilage loss but also from structural changes of the bone.
The prevailing view is that an inverse relationship exists between osteoarthritis (OA) and osteoporosis1; however, whether osteoporosis affects the initiation or progression of OA remains controversial. Several studies have shown that patients with OA tend to have higher bone mineral density (BMD) than patients without OA2–4. In contrast, in other studies, there was no significant difference in the BMD values of patients with and without OA5,6. In any case, not all patients with OA necessarily have high BMD. Osteoporosis progresses rapidly in postmenopausal women; and, similarly, the prevalence of knee OA rises sharply with age such that, after menopause, it is higher in women than in men7. A cohort study has shown that low BMD influences the progression of knee OA4, which may explain the high prevalence of knee OA among postmenopausal women.
Varus inclination of the tibial plateau has been found to be associated with lower lumbar spine BMD in women8. In postmenopausal women with varus knee OA, low BMD may lead to trabecular microfractures of the medial tibial condyle when subjected to impulse loading9, increase varus inclination of the tibial plateau, and cause OA to progress. Dual-energy X-ray absorptiometry (DEXA) at the lumbar spine and the proximal femur is the “gold standard” for screening and followup of osteoporosis. Information on BMD around the knee in osteoarthritic patients has been published10–14. In the present study, in patients with radiographically confirmed symptomatic knee OA, we measured the BMD at not only the lumbar spine and the proximal femur, but also the proximal tibial condyles, using DEXA. To our knowledge, the relationship between BMD at the ipsilateral lower limb and varus inclination of the tibial plateau in postmenopausal women has not been previously investigated. We wished to determine whether low BMD is associated with varus knee OA arising from bone structural changes in postmenopausal women.
MATERIALS AND METHODS
The study involved 135 consecutive outpatients treated at Yokohama City University Medical Center between April 2005 and March 2007. All patients had primary knee OA; patients with a history of knee injury and those who had received steroid injections were excluded. Patients with hip OA, femoral neck fracture, or hemiplegia, all of which affect proximal femoral BMD, were also excluded. None of the patients was being treated with estrogen, vitamin D3, raloxifene, bisphosphonate, or ipriflavone. To minimize the influence of disuse osteoporosis, patients who could not walk unassisted in their day to day lives were also excluded. Patients were considered to have knee OA if they had a Kellgren-Lawrence grade of ≥ 215. Varus knee OA was defined as a narrowing of the medial femorotibial articular space16 with sclerosis of the subchondral bone or osteophyte formation. All subjects had experienced chronic knee pain for > 3 months. Height and weight were measured with the patients in standing position, and body mass index (BMI) was calculated as an index of obesity.
Anteroposterior radiographs of both knees were obtained with the patient standing on one leg. All patients had bilateral knee OA, and the more progressive side was deemed to be the affected site. The femorotibial angle was used to indicate the severity of varus knee OA, and was defined as the lateral angle between the femoral and tibial shaft axes17. To assess intraobserver repeatability and interobserver reproducibility, 135 radiographic measurements were repeated 2 times by 2 observers. The intraclass correlation coefficients (ICC) for intraobserver agreement were 0.998 and 0.997, respectively. The ICC for interobserver was 0.996. Subjects were classified into 3 tertile groups according to the femorotibial angle. The 3 sub-angles8 that together make up the femorotibial angle were also measured (Figure 1): the femoral condylar–femoral shaft (FCFS) angle was defined as the lateral angle between the tangents to the femoral condyles and the femoral shaft axis; the femoral condylar–tibial plateau (FCTP) angle was defined as the angle between the tangents to the femoral condyles and the tibial plateau marginal line; and the tibial plateautibial shaft (TPTS) angle was defined as the lateral angle between the tibial plateau marginal line and the tibial shaft axis.

Measurement of femorotibial angle and 3 sub-angles: femoral condylar-femoral shaft (FCFS) angle, femoral condylar-tibial plateau (FCTP) angle, and tibial plateau-tibial shaft (TPTS) angle8.
BMD values at the lumbar spine, femoral neck, and proximal tibial condylar regions were measured using a QDR-4500 bone densitometer (Hologic Inc., Waltham, MA, USA) with a dual-energy X-ray source (70 and 140 kVp), using standard positioning as recommended by the manufacturer of the bone densitometer. The posteroanterior lumbar spine BMD was a mean value of measurements taken at L2 to L4. The femoral neck BMD was analyzed by using standard software, and there was no significant association between the ipsilateral and contralateral femoral neck BMD (p = 0.211). BMD measurements for the proximal tibia were performed with the patient in the supine position on the scanning table. The knee was flexed at an angle of 20°, and the axis of the tibia was parallel to the scanning table. For estimating BMD at the proximal tibial condyles, 5 square regions of interest were marked on the frontal view of the knee. To achieve this, a line at the level of the tibial plateau, was marked on the DEXA image of the knee. This line extended to the lateral and medial edges of the tibia. The line was then divided into 5 equal lengths, and 5 squares were marked underneath. The BMD value for the 2 medial squares combined was taken as the value for the medial tibial condylar region, and the BMD value for the 2 lateral squares combined was taken as the value for the lateral tibial condylar region (the value for the central square was not used in the calculations). The BMD of the medial and lateral tibial condyle was calculated as the bone mineral content over 2 areas, respectively (Figure 2). Previous data show that this method is adequately precise: in a previous study, the coefficients of variation for BMD measurements of the medial and lateral tibial condylar regions using this method were 2.53% and 2.49%, respectively10.
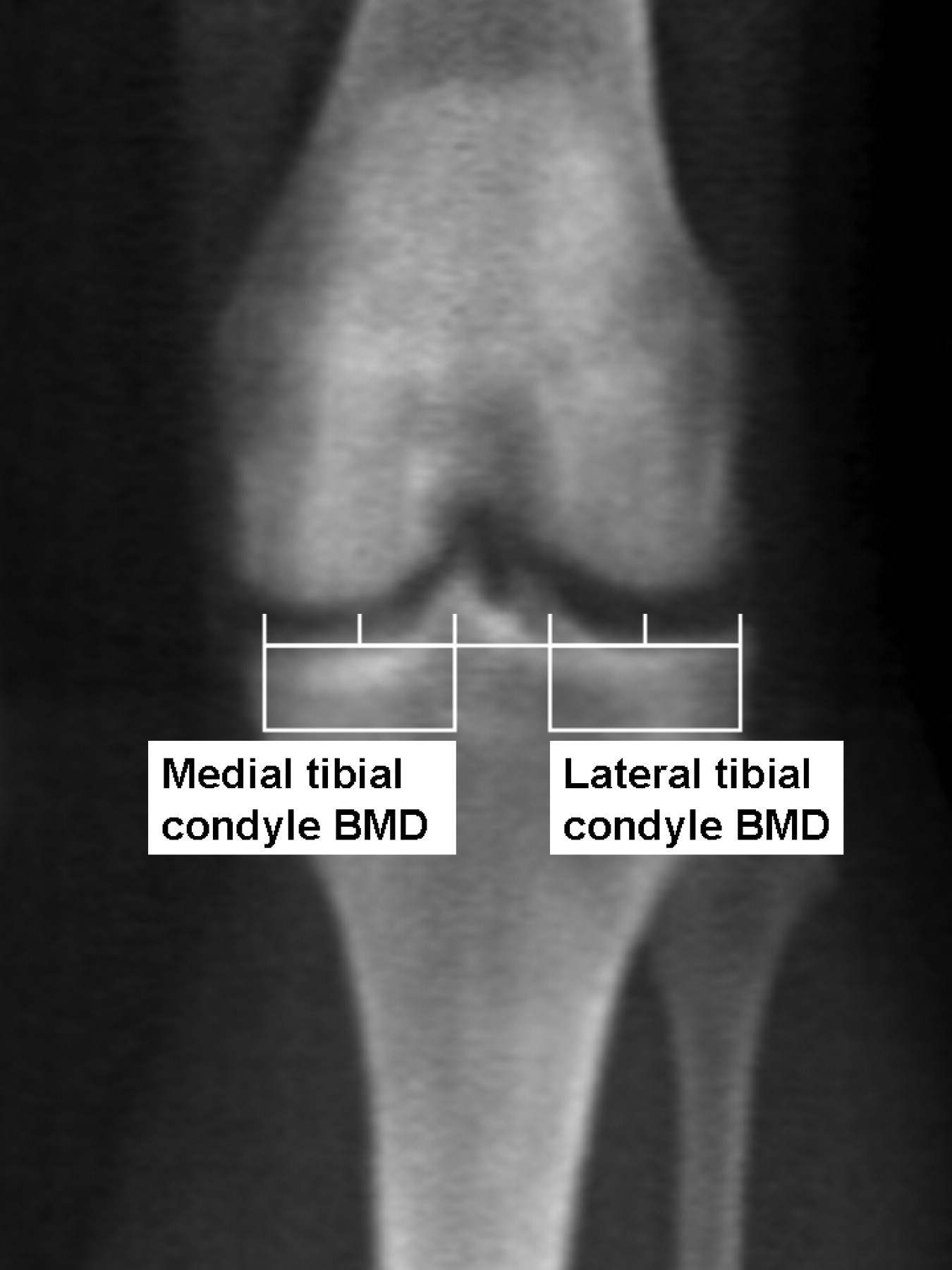
Defining region of interest in knee OA radiograph. Bone mineral density of the medial and lateral tibial condyle was calculated as bone mineral content per the medial and lateral tibial condylar areas.
SPSS for Windows (release 11; SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Data are expressed as means ± standard deviations. Differences between femorotibial angle tertile groups were assessed using analysis of variance (ANOVA). The associations between each of the 3 sub-angles and BMD at various sites were assessed using partial correlation coefficients and linear regression. Significance was set at p < 0.05. All subjects provided informed consent to participate.
RESULTS
Subject characteristics and femorotibial angle.
The subjects’ mean age was 70.4 ± 7.4 years (range 51–87) and mean height was 150.9 ± 6.5 cm (range 130.0–164.0). Mean weight was 55.9 ± 9.0 kg (range 36.0–82.0) and mean BMI was 24.6 ± 3.7 kg/m2 (range 15.9–34.3). The mean femorotibial angle was 182.3° ± 5.2° (range 173.3°–198.5°). Patients were divided into femorotibial angle tertile groups. The subjects’ ages and BMI are shown in Table 1 according to femorotibial angle tertile group. There was no significant difference in the mean age of patients in different tertile groups, but significant differences did exist for mean BMI (p = 0.002). A higher BMI was associated with greater varus deformity. The mean lumbar spine, femoral neck, medial tibial condyle, and lateral tibial condyle BMD values were 0.845 ± 0.141 g/cm2 (range 0.537–1.282), 0.593 ± 0.096 g/cm2 (range 0.417–0.865), 0.894 ± 0.228 g/cm2 (range 0.463–1.472) and 0.596 ± 0.137 g/cm2 (range 0.333–1.068), respectively. The BMD values (for the 4 regions) adjusted for age and BMI are shown in Table 2 according to femorotibial tertile group. There were no significant differences in the mean BMD values at the femoral neck and lateral tibial condyle in different tertile groups, but there was a significant difference between tertile groups with respect to mean BMD at the lumbar spine and medial tibial condyle (p = 0.003, p = 0.005, respectively): higher BMD values at the lumbar spine and medial tibial condyle were associated with more severe varus deformity.
Characteristics of patients with knee OA, according to femorotibial angle tertile group (n = 135). Patients with varus knee OA were classified into 3 tertile groups based on the femorotibial angle. Values are mean ± SD.
Adjusted BMD values at various locations for femorotibial angle tertile groups 1–3. Values were adjusted for age and body mass index. Patients with varus knee OA were classified into 3 tertile groups based on the femorotibial angle. Values are mean ± SD.
Contributions of femorotibial sub-angles to varus deformity.
The mean FCFS, FCTP, and TPTS angles were 81.8° ± 2.0° (range 77.1–88.7), 5.3° ± 3.5° (range 0.1°–17.5°), and 95.2° ± 2.8° (range 89.3°–103.3°), respectively. After the values were adjusted for age and BMI, there were significant differences in FCTP and TPTS angles between femorotibial angle tertile groups (p = 0.009, p < 0.001, respectively), but no significant differences for FCFS angle (Table 3). These findings show that the differences between femorotibial angle tertile groups were chiefly due to medial joint space narrowing and varus inclination of the tibial plateau.
Adjusted FCFS, FCTP, and TPTS angles for femorotibial angle tertile groups 1–3. Values were adjusted for age and body mass index. Patients with varus knee OA were classified into 3 tertile groups based on the femorotibial angle. Values are mean ± SD.
Relationships between femorotibial sub-angles and BMD values.
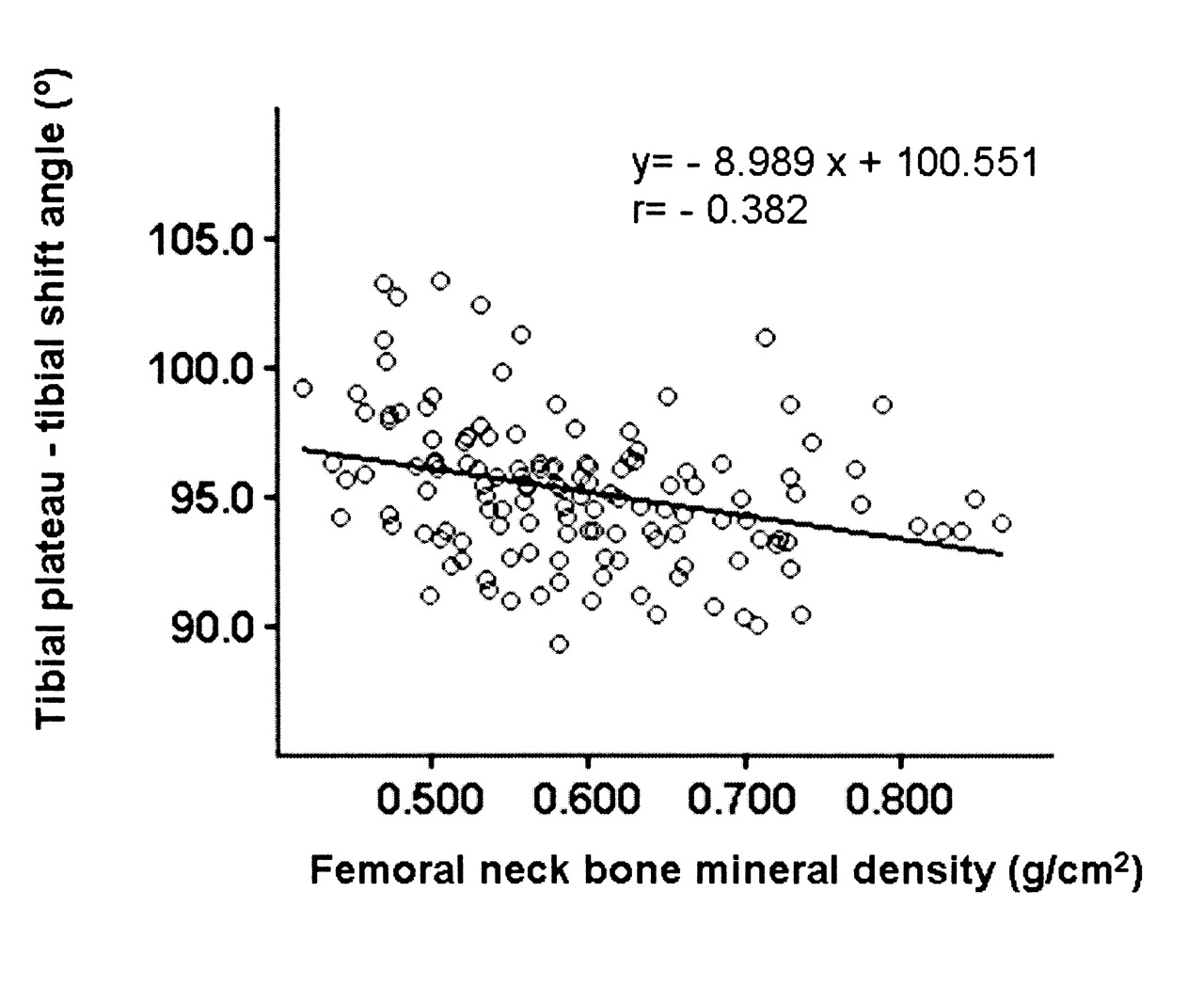
After values were adjusted for age and BMI, partial correlation coefficients were calculated for the association between the femorotibial sub-angles (FCFS, FCTP, and TPTS angles) and lumbar spine, femoral neck, and medial and lateral tibial condyle BMD (Table 4). Lumbar spine BMD was significantly correlated with FCTP angle (r = 0.249, p = 0.004), but not with the FCFS and TPTS angles. Femoral neck BMD was significantly correlated with the FCFS and the TPTS angles (r = 0.184, p = 0.034, and r = –0.382, p < 0.001, respectively), but not with the FCTP angle. Medial tibial condyle BMD was significantly correlated with the FCTP angle (r = 0.569, p < 0.001), but not with the FCFS and TPTS angles. Lateral tibial condyle BMD was significantly correlated with the TPTS angle (r = –0.240, p = 0.005), but not with the FCFS or the FCTP angles. Linear regression analysis of the TPTS angle on femoral neck BMD is shown in Figure 3. This figure shows that low BMD at the ipsilateral proximal femur is weakly but significantly correlated with the varus inclination of the tibial plateau.

Correlation between ipsilateral femoral neck bone mineral density (BMD) and tibial plateau-tibial shaft (TPTS) angle. Values were adjusted for age and body mass index. Low BMD at the ipsilateral proximal femur significantly correlated with the varus inclination of the tibial plateau represented by TPTS angle, although significance was weak.
Partial correlation coefficients for associations between the FCFS, FCTP, and TPTS angles and BMD values at various locations. Values were adjusted for age and body mass index. Femorotibial angle was divided into 3 components.
DISCUSSION
It has previously been shown that varus inclination of the tibial plateau in varus knee OA is associated with low BMD at the lumbar spine8. However, degenerative spinal diseases tend to be associated with increased lumbar spine BMD, potentially confounding the data; therefore, femoral neck BMD might be more appropriate than lumbar spine BMD18 when assessing correlations between BMD and varus inclination. Consequently, we investigated the potential relationship between low BMD at the ipsilateral lower limb and any of the 3 femorotibial sub-angles in postmenopausal women. To our knowledge, this study is the first to address this topic. We found that varus inclination of the tibial plateau is associated with low BMD of the ipsilateral lower limb.
The Kellgren-Lawrence grade is the most widely used indicator of radiographic severity worldwide, but it overemphasizes the importance of osteophytosis relative to joint space narrowing19. In contrast, severity assessed on the basis of joint space narrowing can identify articular cartilage degeneration but not structural changes in bone. As an alternative, varus alignment can serve as a marker of disease severity or progression20. In our study, to evaluate both articular cartilage and bone, the radiographic severity of varus knee OA was estimated using the femorotibial angle. Several studies have demonstrated a strong correlation between data obtained from full-limb measurements of the mechanical axis and short radiographic measurements of the anatomic axis21,22; therefore, we used knee radiographs to estimate valgus–varus alignment, because these smaller images are more convenient to obtain than full-limb measurements.
There are several limitations to our study design. First, the patients had symptomatic knee OA and had been referred to our hospital, and all had Kellgren-Lawrence grades of ≥ 2. There were few postmenopausal women among our subjects who did not experience knee pain, had a Kellgren-Lawrence grade ≥ 2, and had a normal femorotibial angle. Therefore, we could not define a control group. Second, the subjects included patients with more advanced knee OA relative to the total population of people with knee OA.
In agreement with our findings, previous studies also found that a higher medial tibial condyle BMD is associated with more severe varus deformity in knee OA12,13. In our study, there was no association between lateral tibial condyle BMD and femorotibial angle tertile group. In patients who are able to walk unaided in their day to day lives, lateral tibial condyle BMD would not be influenced by disuse osteoporosis with more severe varus deformity (corresponding to a higher femorotibial angle tertile group), and would probably better reflect BMD at the knee than medial tibial condyle BMD. Thus, we propose that the lateral tibial condylar region yields a more accurate estimate of BMD at the ipsilateral knee.
After adjustment for age and BMI, we found a positive association between the FCTP and TPTS angles and the femorotibial angle tertile group, which indicates that both medial joint space narrowing and varus inclination of the tibial plateau contribute to disease severity. This strongly suggests that varus deformity in knee OA is characterized not only by articular cartilage loss, but also by structural changes in bone tissue.
Terauchi, et al8 identified a significant relationship between low BMD at the lumbar spine and varus inclination of the tibial plateau. In contrast, our findings showed that varus inclination of the tibial plateau correlated with only ipsilateral femoral neck and lateral tibial condyle BMD, not lumbar BMD. A possible reason for this discrepancy is that a larger number of cases were involved in the present study.
In a cross-sectional study, Atalar, et al23 found that BMD at the lumbar spine and femoral neck was not associated with the severity of knee OA in postmenopausal women. However, these researchers measured disease severity using the Kellgren-Lawrence grade, which as noted overemphasizes osteophytosis19, so the differences between the findings of Atalar, et al and our study may be due to the different ways that disease severity was assessed.
Cartilage degeneration is accompanied by periarticular changes including osteosclerosis of the subchondral bone and osteophyte formation16. When assessed using microcomputed tomography, subchondral bone in patients with knee OA reportedly has mechanical weaknesses24 and reduced mechanical properties, which indicate poorer bone quality than in individuals without OA25, suggesting that microfractures due to mechanical loading might occur in patients with knee OA and varus inclination of the tibial plateau. In addition, previous experimental data show that, in patients with varus knee OA, medial bone marrow edema lesions identified using magnetic resonance imaging (MRI) are associated with varus deformity26. It is not known whether bone marrow edema affects the structural changes that occur with knee OA. If medial bone marrow edema accompanies microfractures, these previous experimental data might support our findings, suggesting that varus inclination of the tibial plateau follows the occurrence of microfractures at the medial tibial condyle.
In a prospective study, Hart, et al4 found that low BMD at the femoral neck was weakly associated with progression of radiographically confirmed knee OA. Our studies of postmenopausal women with knee OA showed that an increase in the varus inclination of the tibial plateau is associated with a lower BMD at the ipsilateral lower limb, which may explain Hart’s findings. Our findings may allow clarification of which factors contribute to varus deformity, and help to determine what is influenced by low BMD in the ipsilateral lower limb. Recently, Carbone, et al27 reported that use of both alendronate and estrogen is associated with significantly less subchondral bone attrition; in turn, maintaining high BMD may be an effective approach for preventing progression of varus knee OA.
Our results show a weak but significant negative correlation between varus inclination of the tibial plateau and BMD at the ipsilateral proximal femur and lateral tibial condyle in postmenopausal women with varus knee OA. We speculate that low BMD may contribute to increasing varus deformity via structural changes of the proximal tibial bone.
Footnotes
- Accepted for publication October 31, 2008.








{kind=link}
{kind=link}
{kind=link}