

Abstract
Objective. To evaluate the diagnostic performances of 2 recently developed assays, third-generation anti-cyclic citrullinated peptide (anti-CCP3) and anti-mutated citrullinated vimentin (anti-MCV), in comparison to conventional second-generation anti-cyclic citrullinated peptide (anti-CCP2) assay; and to assess a novel fully automated, random-access AxSYM anti-CCP assay for early diagnosis of rheumatoid arthritis (RA).
Methods. A cohort of 176 patients was enrolled in our study; 93 were diagnosed as having RA. The non-RA group consisted of 83 patients including 38 with systemic lupus erythematosus, 17 with primary Sjögren’s syndrome, 11 with osteoarthritis, and 17 healthy controls. All were tested for presence of anti-CCP2, anti-CCP3, AxSYM anti-CCP, anti-MCV, and rheumatoid factor (RF)-IgM according to the manufacturers’ instructions.
Results. Diagnostic performance of the assays revealed the highest area under the curve for the novel AxSYM anti-CCP [89.1; 95% confidence interval (CI) 84.3–93.8], followed by anti-CCP3 (86.7; 95% CI 81.6–91.9), anti-CCP2 (82; 95% CI 75.8–88.3), and anti-MCV (71.9; 95% CI 64.4–79.5). The sensitivities and specificities were 60.2% and 98.8% for anti-CCP2, 61.3% and 97.6% for anti-CCP3, 80.6% and 84.3% for AxSYM anti-CCP, 49.8% and 91.6% for anti-MCV, and 67.8% and 91.6% for RF-IgM, respectively.
Conclusion. At cutoff of 5 U/ml, AxSYM anti-CCP emerged as a highly sensitive first-line early diagnostic tool for RA, with the greatest discrimination power, above 16 U/ml, in case of positive result. Using a single easily performed automated assay at 2 determined decision limits we were able to diagnose 81% of cases of RA and missing only 1.2%.
- AUTOMATION
- CYCLIC CITRULLINATED PEPTIDE AUTOANTIBODIES
- DIFFERENTIATION
- DIAGNOSIS
- EARLY RHEUMATOID ARTHRITIS
- MUTATED CITRULLINATED VIMENTIN
Rheumatoid arthritis (RA) is a common inflammatory disease with an average prevalence of 1%. It affects women twice as frequently as men and is diagnosed mostly between the fourth and sixth decades of life1. Recent studies have shown that therapeutic intervention early in the course of RA can lead to disease control reflected by less joint damage, increased remission rate, and decreased disease related disability2,3. As the newly developed drugs utilized are potentially toxic, it is important to make a diagnosis as early as possible and to develop a rational treatment strategy with respect to the expected disease severity. Extensive variations in the course of the illness ranging from mild to aggressive disease, and the evidence that substantial irreversible damage occurs within the first years of the disease, necessitated RA to be considered as a medical emergency requiring prompt differentiation from other types of arthritis4–6.
Although mainly developed for the classification of the disease, the American College of Rheumatology (ACR) criteria are used as a diagnostic standard for RA in clinical practice. These well known criteria include characteristics that are rare in new-onset RA, and several studies have shown their suboptimal diagnostic sensitivity and specificity, ranging from 40% to 90% and from 50% to 90%, respectively, in subjects with arthritis symptoms of less than 2 years’ duration7–11.
Comprehensive research on the pathophysiologic processes of RA revealed that besides the genetic, environmental, and autoimmune grounds of the illness, citrullination of synovial proteins is an active process taking place during the course of inflammation12,13. It was supposed that citrullination could alter interactions of the primary proteins with its receptors and with growth factors, and contribute by itself to mechanisms of RA pathogenesis such as perturbed angiogenesis and apoptosis. Moreover, the recognition of these citrullinated proteins by autoantibodies already present in the systemic circulation of patients with RA can lead to the formation of immune complexes, complement activation, and further activation of immune system, additionally contributing to the inflammatory process and tissue damage14. Indeed, some of the autoantibodies found in RA are primarily directed against these citrullinated protein epitopes and can be found even before the symptoms of arthritis appear15. Being able to detect these specific antibodies appeared to fulfill the requirement for reliable and specific tests to detect a marker early in the disease that would be useful to identify patients with RA prior to the occurrence of irreversible damage.
There has been rapid development of various serological assays measuring antibodies directed against different citrullinated proteins and peptides. Tests to measure artificially designed cyclic citrullinated peptide (CCP) are of special interest, because of their high specificity for early RA and the ability to predict erosive arthritis16. Efforts to improve the sensitivity led to the development of anti-second and more recently anti-third-generation CCP assays (anti-CCP2, anti-CCP3), the studies on which, lately reviewed, all confirmed the rheumatoid factor (RF)-like sensitivity while preserving the high specificity for RA17–19. Similarly, an assay named anti-mutated citrullinated vimentin (anti-MCV), detecting antibodies against another citrullinated protein, vimentin (formerly known as anti-Sa antibodies), which is an intermediate filament widely expressed in mesenchymal cells and also detectable in the synovial fluid of patients with RA, was found to perform comparably well in the diagnosis of RA20–23.
In a clinical laboratory setting, anti-CCP and anti-MCV assays were designed primarily as enzyme-linked immunosorbent assay (ELISA) commercial kits. Recently, a novel fully automated microparticle enzyme immunoassay (MEIA) was adopted for measurement of anti-CCP2 antibodies (AxSYM anti-CCP), which in addition to the preliminary purposes, was also simpler and achieved better test accuracy and precision.
Due to the growing number of different commercial assays and the studies of their utility in diagnosis of RA, a recent study successfully incorporated anti-CCP testing to the established ACR criteria for RA24. Regardless of this, there is no established consensus recommending a single test, other than RF as a part of the ACR criteria, or test combination for the purposes of screening, diagnosis, prediction of disease course, prognosis, or response to treatment that could potentially improve overall management of RA.
Our study evaluated diagnostic performances of 2 newly developed assays, anti-CCP3 and anti-MCV, in comparison to the conventional anti-CCP2, all using ELISA methodology. We also assessed a novel fully automated, randomaccess AxSYM anti-CCP, that can be easily adapted to clinical practice, for any diagnostic improvement over the former 3 assays, allowing for the more convenient technology used. All the assays were associated with the RF-IgM assay as the only test included in ACR criteria.
MATERIALS AND METHODS
Patients and sample design.
A cohort of 176 patients, examined in the rheumatology clinics of 3 different hospitals from January 2006 to September 2007, was enrolled in the study. Ninety-three patients with median age of 52 years (range 26–76 yrs) and male to female ratio of 1:5 were diagnosed as having RA according to ACR criteria25. Eighty-three patients constituted the non-RA group, including 38 with systemic lupus erythematosus (SLE), 17 with primary Sjögren’s syndrome (pSS), 11 with osteoarthritis (OA), and a healthy control group of 17 subjects. The diagnoses of diseased control patients were based on revised ACR criteria for SLE and OA, and proposed European classification criteria for pSS, by 3 different rheumatologists26–28. None of the patients with SLE had erosive joint lesions; also, no hip joint involvement was observed within the OA group as documented by routine radiography. Three patients with OA presented with localized disease (only distal interphalangeal joint involvement), 5 had generalized 3 or more joints or joint group involvement, and finally, 3 patients with OA were diagnosed to have erosive disease with lesions and osteophyte formation of proximal and distal interphalangeal joints. Healthy controls were selected from hospital medical staff after evaluation for family history and presence of any signs or symptoms indicating potential rheumatologic illness. Special emphasis was given to signs and symptoms of OA such as pain and swelling of joints, morning stiffness, deformity formation, and crepitus on motion for the patients over age 40 years, and for exclusion purposes radiological evaluations were performed when appropiate. The study fulfilled guidelines required by the local ethics committee. Written consent was obtained from all patients.
Collection and handling of serum samples were performed according to the National Committee for Clinical Laboratory Standards recommendations, and samples were frozen and stored at –20°C until analysis. For each sample, testing for anti-CCP2, anti-CCP3, AxSYM anti-CCP, anti-MCV, and RF-IgM was performed within the same 24-h freeze-thaw cycle.
Analytical methods.
Serum samples from all patients and the control groups were analyzed in duplicate for levels of anti-CCP2, anti-CCP3 (Inova Diagnostics, San Diego, CA, USA) and anti-MCV (Orgentec Diagnostika GmbH, Mainz, Germany) using ELISA, performed according to the manufacturers’ recommendations. RF-IgM levels were measured quantitatively by means of particle-enhanced immuno-nephelometry using BN system technology (Dade Behring GmbH, Marburg, Germany). The novel AxSYM anti-CCP assay (Abbott Diagnostics Europe, Wiesbaden, Germany), planned to be primarily evaluated, was performed utilizing MEIA technology for semiquantitative determination of the IgG class of autoantibodies specific to CCP2, preliminarily designed by Axis-Shield Diagnostics (Dundee, UK) and subsequently implemented on the fully automated random-access AxSYM system.
Statistical analysis.
Data were analyzed using statistical software packages Analyze-it Method Validation Edition for Microsoft Excel 2007 (version 1.62) and SPSS for Windows (version 15; SPSS Inc., Chicago, IL, USA). Values were tested for normal distribution by Shapiro-Wilk test. Kruskal-Wallis nonparametric analysis of variance, Mann-Whitney U-test, chi-squared test, and Pearson’s rank correlations were performed to compare assay values among the groups. Two-tailed p value < 0.05 was considered statistically significant. Sensitivity and specificity values of assays were obtained from receiver-operating characteristic (ROC) curve analysis, a global measure of the diagnostic performance of a test, that was carried out considering total RA group (n = 93) versus total non-RA group (n = 83) data29. Additional ROC curve analyses of RA group versus non-RA inflammatory disease subgroup (SLE and pSS) and non-RA noninflammatory disease subgroup (OA and controls), separately and in combination, were also performed. Z-test was performed to compare areas under the curve (AUC) for the different assays obtained from ROC analysis.
RESULTS
Descriptive and clinical characteristics of the study groups.
Demographic, clinical, and serological records of patients at the time of serum sample collection were compared. Median ages were equivalent among the groups except for SLE, composed of patients of statistically significant younger age, and OA, composed primarily of older subjects. Male to female ratios of patients for each disease group were consistent with the literature. Fifteen patients with RA were found to have early disease with less than 6 months after onset of symptoms (average 3.7 mo) and 78 had established RA, with an average time after diagnosis of 4.6 years (range 7 mo to 26 yrs). Forty-four percent of patients with RA were diagnosed to have active disease considering Disease Activity Score-28 (DAS-28) ≥ 5.1. In the RA patient group, highest positivity ratio of all autoantibodies tested was observed with AxSYM anti-CCP (88.5% for early and 77.6% for established RA), followed by RF-IgM and anti-CCP3. Autoantibody false-positivity ratios of non-RA patients peaked within the pSS group, with the exception of anti-CCP2 and anti-CCP3, which were not observed in any of the pSS patients. The second most frequently antibodypositive non-RA group was the SLE group, which was highest in the AxSYM anti-CCP and anti-MCV (15.8% and 13.2%, respectively). The OA patient group showed positivity only with RF-IgM (9.1%), while in contrast, the average autoantibody presence measured by assays was found to be as low as 4.7% for control subjects, who were all negative for anti-CCP2 and anti-MCV (Table 1).
Demographic, clinical, and serological characteristics of the study groups.
Analytical performance of the assays.
All 176 serum samples were run in duplicate for the presence of anti-CCP2, anti-CCP3, AxSYM anti-CCP, anti-MCV, and RF-IgM autoantibodies. Verification data of the assays are shown in Table 2. Values exceeding measuring ranges were obtained by either manual or automatic predilution (for AxSYM anti-CCP) of relevant samples. The average reproducibility data at 2 different concentrations for each assay did not exceed overall values stated by the manufacturers. Comparison analyses in relation to RF-IgM assay, although not excellent, revealed best Pearson correlation for anti-CCP3 and AxSYM anti-CCP (r = 0.472 and r = 0.423, respectively), all statistically significant (p < 0.001). Correlation among the 4 anti-CCP assays was highest between anti-CCP2 and anti-CCP3 (r = 0.873), followed by anti-MCV, which correlated well with both anti-CCP3 and anti-CCP2 (r = 0.729 and r = 0.713, respectively). AxSYM anti-CCP correlated best with anti-MCV (r = 0.667), followed by anti-CCP2 (r = 0.568) and anti-CCP3 (r = 0.491).
Analytical performance characteristics of the assays.
Diagnostic performances of the assays.
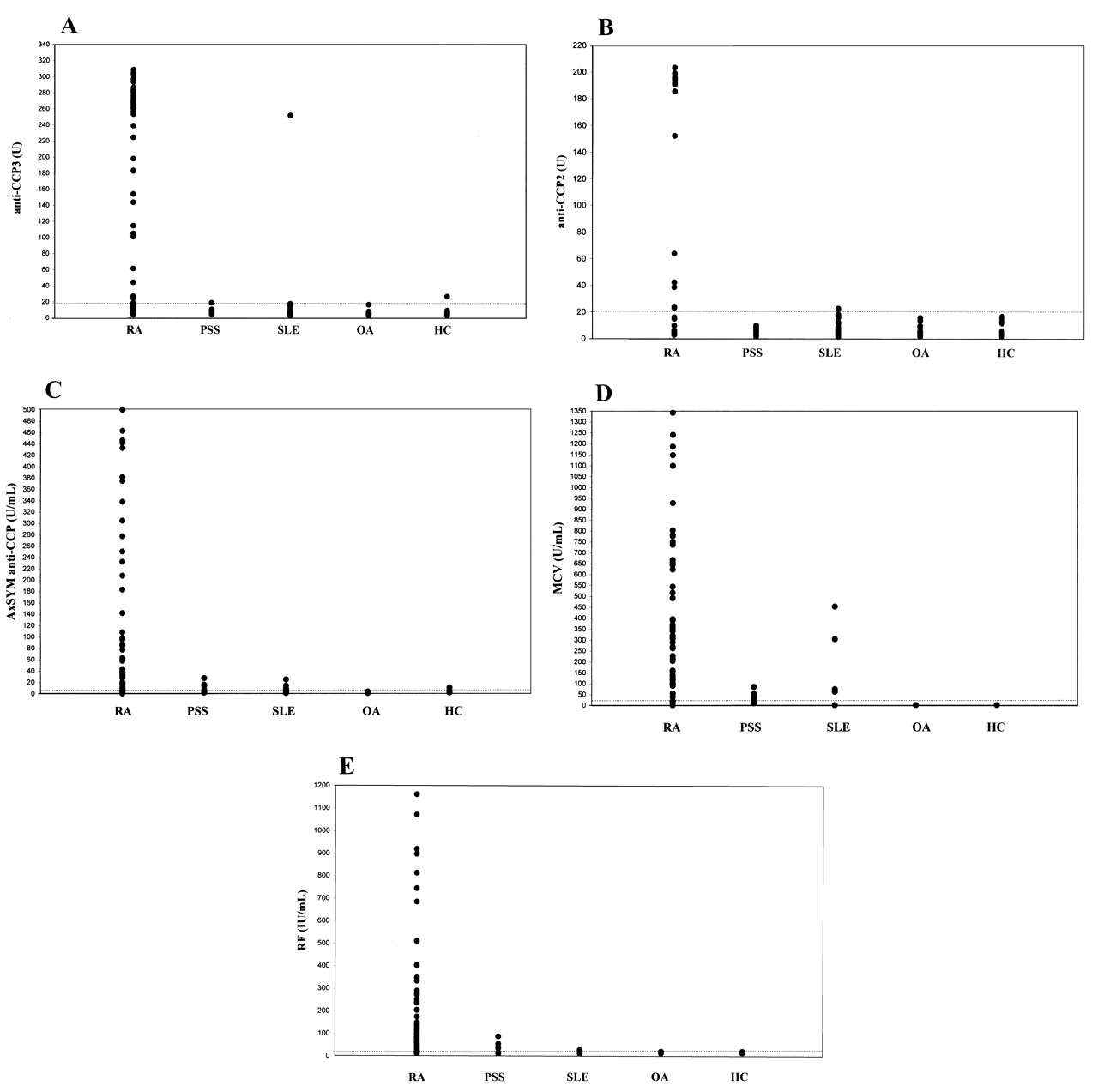
Distributions of all assay values among the study groups were analyzed (Figure 1). Mean concentration values of all assays were found to be significantly higher in the RA group compared to values of disease controls and healthy controls, denoting comparable efficacy in critical disease-state differentiation (p < 0.001, Table 3). None of the tests was able to distinguish early from established RA, indicating similar performances for both cases (p > 0.05, data not shown).

Scatter plots of anti-CCP3 (A), anti-CCP2 (B), AxSYM anti-CCP (C), anti-MCV (D), and RF-IgM (E) assays; the manufacturers’ cutoffs are shown as broken line.
Quantitative assay value distribution between the study groups.
Considering all patient groups, ROC analysis of the 4 assays in comparison to RF-IgM revealed the highest AUC for the novel AxSYM anti-CCP [89.1; 95% confidence interval (CI) 84.3–93.8], statistically superior to all remaining assays except for anti-CCP3 (86.7; 95% CI 81.6–91.9, p = 0.386). Next, anti-CCP2 performed with lower but not statistically different AUC (82; 95% CI 75.8–88.3) compared to anti-CCP3 (p = 0.104) and again was not significantly higher than the RF-IgM assay (80.8; 95% CI 74.2–87.3; p = 0.705). Finally, anti-MCV (71.9, 95% CI 64.4–79.5), with the lowest AUC, was statistically inferior to all the remaining assays (p < 0.002; Figure 2). Accordingly, at the manufacturers’ preset cutoff values the AxSYM anti-CCP had the maximum sensitivity value of 80.6%, reflecting the greatest assay ability in the diagnosis of RA. However, the 84.3% specificity of the assay was considerably lower compared to all the other assays including RF-IgM, demonstrating decreased power of the test to discriminate RA from non-RA cases at this cutoff. At the manufacturers’ cutoffs anti-CCP2 and anti-CCP3 performed with the greatest specificity (98.8% and 97.6%, respectively, not statistically different from each other), followed by RF-IgM and anti-MCV with the same specificity value of 91.6%. Attempts to determine the optimal performance cutoffs via calculating the highest sum of sensitivity and specificity values for each assay verified the same decision levels for RF-IgM, anti-CCP2, and AxSYM anti-CCP, as proposed by the manufacturers. On the other hand, anti-CCP3 performed optimally at the level of 11.7 U, with sensitivity of 67.7% and specificity of 92.8%, and anti-MCV had a sensitivity of 45.2% and specificity of 97.6% at the optimal 82.3 U/ml cutoff limit (Table 4). At the observed highest specificity value of 98.8% determined for anti-CCP2, revealing the highest disease differentiation ability, diagnostic performance characteristics of all assays were compared (Table 5). At this most clinically relevant specificity value, corresponding to a cutoff of 27.1 U, anti-CCP3 performed with the same sensitivity as anti-CCP2 (both 60.2%), followed by the AxSYM anti-CCP, with a sensitivity value of 57% at a 16 U/ml cutoff limit. RFIgM reflected sensitivity of 48.4%, and finally the lowest sensitivity, 29%, was observed with anti-MCV.

Diagnostic analysis with the AUC for the AxSYM anti-CCP (89.1; 95% CI 84.3–93.8), anti-CCP (86.7; 95% CI 81.6–91.9), anti-CCP2 (82; 95% CI 75.8–88.3), anti-MCV (71.9; 95% CI 64.4–79.5), and RF-IgM (80.8; 95% CI 74.2–87.3) assays.
Diagnostic performance of the assays at manufacturers’ and optimal decision levels.
Qualitative assay performance characteristics at the highest specificity decision level.
Results of additional ROC analyses using either the non-RA inflammatory disease subgroup (SLE and pSS) or the non-RA noninflammatory disease subgroup (OA and healthy controls) as a control group, separately and in combination, are presented in Table 6. Generally, the data reflected a performance characteristic pattern identical to that of the original ROC analysis of all patient groups taken together. Considering the assays’ sensitivity values, there was no prominent difference between the inflammatory and noninflammatory disease subgroups; however, specificity values were found to differ among the groups. Except for anti-CCP3 and mostly for the AxSYM anti-CCP and anti-MCV assays, typically specificities were observed to be significantly lower for the inflammatory compared to noninflammatory disease control subgroup. It was also observed that when patients with pSS were considered a separate disease control group, the specificity values of AxSYM anti-CCP and RF-IgM assays in particular worsened (from 84.2% for SLE to 70.6% for pSS and from 97.4% for SLE to 76.5% for pSS control groups, respectively). In contrast, specificities of anti-CCP2, anti-CCP3, and anti-MCV assays were not affected and remained significantly high by use of either SLE or pSS patient groups separately. When only the noninflammatory disease control subgroup (OA + healthy controls) was used for ROC analysis, specificities of anti-CCP2 and anti-MCV assays reached the ideal 100%, followed by anti-CCP3 (96.4%), AxSYM anti-CCP, and RF-IgM (both 92.9%) assays.
Diagnostic performance of the assays at manufacturers’ decision levels considering different non-RA control subgroups for receiver-operator characteristic (ROC) analysis.
DISCUSSION
Our study aimed at assessment of diagnostic performances of 4 assays, measuring antibodies against different citrullinated proteins, in comparison to conventional RF-IgM assay, for early diagnosis and differentiation of RA. When we verified technical and analytical characteristics of the assays for lower detection level, measuring range and imprecision limits were found to be concordant with statements of the manufacturers. While far below the allowable 15% total coefficient of variation (CV), the AxSYM anti-CCP assay displayed the highest total intraassay and interassay CV. Still, this was not significant for the intraassay CV, and could be explained with the presence of minor sample to sample carryover within the AxSYM system. Such a limitation, in contrast to the manual ELISA conveying only a single measure for a given time, is potentially observed with any fully automated random-access device designed to simultaneously measure multiple parameters and patient samples. The method of comparison analysis established statistically significant but rather weak correlations of each of the 4 assays in relation to the RF-IgM assay. However, good correlation was observed among anti-CCP2, anti-CCP3, anti-MCV, and to a lesser extent the AxSYM anti-CCP assays. Although utilizing the same citrullinated synthetic anti-CCP2 antigen, application of different conjugate and substrate reagents and more importantly the particular assay design (MEIA versus ELISA methodology) could be potential reasons for the rather lower correlation between the AxSYM anti-CCP and anti-CCP2 assays30. However, even with the absence of standardized reference material essential for method harmonization, the overall acceptable technical performances of assays enabled their comparative evaluation for disease diagnosis purposes.
Considering antibody prevalence in the RA group at the manufacturers’ cutoff levels, the AxSYM anti-CCP followed by RF-IgM and anti-CCP3 assays showed significantly higher frequency compared to the remaining assays. Evaluation of positive cases in non-RA patient groups revealed high antibody presence especially for pSS and SLE patient groups, demonstrated by the AxSYM anti-CCP (29.4% and 15.8%, respectively), anti-MCV (11.8% and 13.2%), and RF-IgM (23.5% and 2.6%) assays, but found very low antibody presence for SLE and absence for pSS with the anti-CCP2 and anti-CCP3 assays. This observation was further highlighted by the additional ROC curve evaluations, revealing particularly for the AxSYM anti-CCP and RF-IgM assays prominent decreases in specificity values, when the non-RA inflammatory disease control subgroup and especially when only pSS patients were taken into account (Table 6). It could be supposed that pSS and to a lesser extent SLE non-RA inflammatory joint diseases are harder to differentiate from RA, especially with the AxSYM anti-CCP, anti-MCV, and RF-IgM assays. Although the false-positive rate appears to be assay-dependent in our study, this does not exclude the previous reports of the association of citrullinated protein antibody presence with pSS and SLE, suggesting possible disease progression to RA in the former group and a pathogenic role in major erosions resulting in clinical features that overlap SLE with RA31,32. In contrast, however, these studies focused primarily on the prevalence of citrullinated protein antibody in general, with only one assay tested, rather than comparing different assay systems, allowing us to make this observation. Moreover, none of the non-RA inflammatory disease control patients in our study had erosive arthritis, selected especially to overcome the problem in question. The overall false-positive ratios within non-RA groups (14.3% for AxSYM anti-CCP, 10.3% for RF-IgM, 6.3% for anti-MCV, 2.1% for anti-CCP3, and 0.7% for anti-CCP2 assays) were notably different for the different citrullinated peptide antibody assays. At this point, combining the high antibody detection capability for the RA group and the low false-positive results in the non-RA patient groups, our findings pointed to the anti-CCP3 assay as the most suitable candidate for diagnosis of RA, while the highest antibody falsepositivity rate observed for non-RA patient groups at the proposed manufacturer’s cutoff value seemed to disqualify the AxSYM anti-CCP assay from doing so (Table 1).
ROC analysis for assessment of diagnostic relevance of the assays revealed acceptable performance for the RF-IgM assay, with considerable sensitivity (67.8%) and specificity (91.6%) values. In particular, the high specificity for the RF-IgM assay could be explained by the presence of a higher number of established (84%) compared to early RA cases, and preferably selecting patients with definite diagnoses for the non-RA groups in our patient population. Contrasting all other assays against the RF-IgM assay in terms of sensitivity and specificity revealed the highest sensitivity value for the AxSYM anti-CCP assay (80.6%) and specificity value for the anti-CCP2 assay (98.8%), at the manufacturers’ cutoffs. Because we were equally interested in diagnosing RA with a high ability to differentiate from other arthritis cases, we further compared the sensitivity values of the assays at the maximum specificity value observed for the anti-CCP2 assay.
Although it correlated well with the remaining anti-CCP assays, generally the anti-MCV assay added no further advance over the RF-IgM assay in terms of specificity, and performed with lower sensitivity at the predefined manufacturer’s cutoff. Further, at the highest specificity range the assay revealed the lowest sensitivity value, a finding that appears to be in agreement with previous reports, including comparison of the same assay systems for anti-CCP2 and anti-CCP3 carried out by Bizzaro, et al30. Contrasting the diagnostic validity measures of the anti-MCV assay with recent studies generally revealed similar specificity, but lower sensitivity values, for our study20–22. A possible explanation might be the predominance of RF-positive patients with RA in our group, diminishing the value of the anti-MCV assay, considered primarily useful in diagnosis of RA in patients who are RF- and anti-CCP2-seronegative22. However, the absence of such a relationship in our study prevents us from suggesting combined application of the anti-CCP2 and anti-MCV assays to improve the laboratory diagnosis of RA, as was recommended by the subjected report. Moreover, controversial studies exist about the anti-MCV assay and disease activity: Innala, et al33 found anti-MCV to be associated with more severe disease in contrast to both anti-CCP2 and anti-CCP3 antibodies; and due to observed poor correlation, Ursum, et al34 concluded that anti-MCV is not a useful assay to monitor RA disease activity.
The diagnostic performance of the anti-CCP2 ELISA assay appeared to be generally in agreement with other studies, recently evaluated by a metaanalysis35. The assay revealed the highest specificity of 98.8% among all the other assays, with considerable sensitivity of 60.2% at the manufacturer’s cutoff. Although developed with the primary aim of increasing sensitivity while preserving high specificity, in our study, exactly the same values were obtained for the anti-CCP3 assay at a slightly higher cutoff value, which also accounted for the maximal specificity value (Table 5). Few studies have compared anti-CCP2 and anti-CCP3 assays for their diagnostic efficacies, and generally these demonstrated slightly but not significantly higher sensitivities and specificities, ranging between 51.5% and 79% and 93%–98.5%, respectively, for anti-CCP3, and 54.8%–77% and 90%–98.5%, respectively, for anti-CCP2, either at the manufacturer’s optimal or maximal specificity cutoff values19,30,36–38. However, with the combined higher antibody prevalence for the RA group and lower false-positive results for the non-RA group, as discussed, the anti-CCP3 assay appears to be a better diagnostic candidate than the anti-CCP2 assay.
We also evaluated, for the first time to our knowledge, the diagnostic properties of a new fully automated randomaccess AxSYM anti-CCP assay. There have been earlier automated anti-CCP assay evaluation studies, but all used different ELISA methodology and were performed on the UniCAP100 instrument (Phadia, Freiburg, Germany) with no random-access properties19,30,38,39. In addition to a clinically confirmed diagnostic value of any assay, its application in an automated, analytically proven highly sensitive method, and random-access availability for samples, allowing fast testing with minimal user-associated errors, is a very important criterion for general practical use. This feature of the AxSYM anti-CCP assay, coupled with the very high sensitivity value (80.6%) at the manufacturer’s cutoff, not observed with any of the other nonautomated anti-CCP assays and very similar to the alternative automated ELISA anti-CCP assay (80%), was one significant result of our study39. Unfortunately, at the manufacturer’s proposed cutoff, the specificity of the assay was found to be significantly lower than for all other assays tested, including the RF-IgM assay (Table 4). However, when considering the highest (98.8%) specificity value set at a higher 16 U/ml cutoff limit, the 57% sensitivity of the AxSYM anti-CCP assay was comparable to both anti-CCP2 and anti-CCP3 assays (60.2%, Table 5). Considering the advancement of automation, with a preserved specificity of 98.8%, the slightly lower but generally comparable sensitivity for the novel AxSYM anti-CCP could be disregarded, without losing much of the assay’s overall diagnostic performance.
Consistent with the main methodological limitation observed in the comparative metaanalysis35 of various studies over the diagnostic accuracy of the different assays for RA, our results indicated that meaningful comparison of different citrullinated protein antibody assays is only possible with the introduction of universally applied standardized reference material, which is crucial for method harmonization. Then more reliable technical and analytical assessment studies can be performed; otherwise subsequent reports on the subject will not achieve the desired result, namely discovering the most appropriate diagnostic marker for RA.
Bearing in mind the limitations of our study, at a cutoff level of 5 U/ml, the AxSYM anti-CCP assay emerges as a highly sensitive first-line early RA diagnostic tool, with the added advantage of achieving greatest discrimination power when the potential positive result measures above the determined most specific cutoff level of 16 U/ml. Allowing for this, using the automated assay at 2 determined decision limits, almost 81% of cases will be accurately diagnosed, missing only 1.2% of actual RA cases.
Acknowledgments
We thank Fehime Ozdal, Ilkay Bostanci, Ipek Z. Seven, and Yasemin Ozturk for their excellent technical assistance.
Footnotes
- Accepted for publication September 15, 2008.








{kind=link}
{kind=link}