

Abstract
In 2003, the first reports describing osteonecrosis of the jaw (ONJ) in patients receiving bisphosphonates (BP) were published. These cases occurred in patients with cancer receiving high-dose intravenous BP; however, 5% of the cases were in patients with osteoporosis receiving low-dose bisphosphonate therapy. We present the results of a systematic review of the incidence, risk factors, diagnosis, prevention, and treatment of BP associated ONJ. We conducted a comprehensive literature search for relevant studies on BP associated ONJ in oncology and osteoporosis patients published before February 2008.All selected relevant articles were sorted by area of focus. Data for each area were abstracted by 2 independent reviewers. The results showed that the diagnosis is made clinically. Prospective data evaluating the incidence and etiologic factors are very limited. In oncology patients receiving high-dose intravenous BP, ONJ appears to be dependent on the dose and duration of therapy, with an estimated incidence of 1%–12% at 36 months of exposure. In osteoporosis patients, it is rare, with an estimated incidence < 1 case per 100,000 person-years of exposure. The incidence of ONJ in the general population is not known. Currently, there is insufficient evidence to confirm a causal link between low-dose BP use in the osteoporosis patient population and ONJ. We concluded BP associated ONJ is associated with high-dose BP therapy primarily in the oncology patient population. Prevention and treatment strategies are currently based on expert opinion and focus on maintaining good oral hygiene and conservative surgical intervention.
Osteonecrosis of the jaw (ONJ) is characterized by the accumulation of dead exposed bone in the oral cavity. Over the past century, it has been associated with tissue damage following head and neck irradiation in cancer patients. Other risk factors for the development of osteonecrosis include underlying malignancy, chemotherapy, corticosteroids, and local infection1-3. Impaired blood supply appears to be an important risk factor for the development of osteonecrosis. Osteoradionecrosis is believed to result from ionizing radiation damage to the microvasculature and to bone cells in the mandible and maxilla. Osteonecrosis is associated with significant morbidity and can be a difficult condition to treat. In 2003, the first reports describing ONJ in patients receiving bisphosphonates were published. High-dose intravenous (IV) bisphosphonate use in the oncology patient population has been recognized as a contributing factor to the development of ONJ. It is, however, not known if low-dose bisphosphonate use in the osteoporosis population is also associated with osteonecrosis. However, due to concerns regarding a possible link between low-dose bisphosphonate therapy in osteoporosis patients and ONJ, patients receiving bisphosphonates have become increasingly concerned regarding potential oral side effects of these agents.
Bisphosphonates currently serve as a cornerstone in the management of osteoporosis and metabolic bone disease4 and are also of proven benefit in reducing skeletal complications of malignancy5-10. The mechanisms whereby bisphosphonates may contribute to the development of osteonecrosis are still not fully understood. Proposed mechanisms include further reduction in osteoclastic activity in an area of bone that may be relatively hypocellular due to previous chemotherapy and/or radiotherapy impairing the ability of the bone to resorb and replace damaged tissue. This may explain the impaired bone healing at sites of dental extraction. Aminobisphosphonates have also been postulated to have antiangiogenic effects11. However, other agents known to have antiangiogenic effects, such as thalidomide, that are also effective agents in myeloma have not been confirmed as contributing factors to the development of ONJ12.
Reid and colleagues recently proposed that bisphosphonates may have toxic effects on oral epithelium overlying areas of high bone bisphosphonate concentrations, decreasing the ability of the oral mucosa to heal following local trauma such as tooth extraction13. Data to support this hypothesis come from the case of contact stomatitis in a patient sucking bisphosphonate tablets14. To understand the pathogenesis of bisphosphonate associated osteonecrosis further prospective data are needed.
The purpose of this systematic review is to provide an organized summary and analysis of the evidence available on the following key areas pertaining to bisphosphonate associated ONJ: (1) diagnostic features, (2) incidence and prevalence, (3) risk factors, (4) prevention, (5) staging, and (6) treatment. We also aimed to identify current knowledge gaps pertaining to bisphosphonate associated ONJ and propose a research agenda for this condition.
MATERIALS AND METHODS
This systematic review is the basis for the Canadian Consensus Practice Guidelines for Bisphosphonate Associated Osteonecrosis of the Jaw15. The Canadian Association of Oral and Maxillofacial Surgeons in association with national and international multidisciplinary societies formalized the Canadian Task Force on Osteonecrosis of the Jaw in 2006. The multidisciplinary task force included representatives from the relevant societies representing the disciplines of oral surgery, endocrinology, dentistry, oral pathology and oral medicine, rheumatology, and oncology. The task force identified 6 research questions to be addressed by the review: (1) What are the diagnostic features of bisphosphonate associated osteonecrosis of the jaw? (2) How common is bisphosphonate associated osteonecrosis of the jaw? (3) What are the risk factors for bisphosphonate associated osteonecrosis of the jaw? (4) Can we prevent bisphosphonate associated osteonecrosis of the jaw? (5) How do we stage established bisphosphonate associated osteonecrosis of the jaw? (6) What are the current treatment strategies for bisphosphonate associated osteonecrosis of the jaw?
Study identification.
As the amount of literature on the topic is limited, a wide literature search was utilized. The electronic search was conducted in Medline (1966 to October 2007) and Embase (1980 to October 2007) using OVID. A search strategy was developed for each database by combining medical subject headings and/or text words from 4 categories: interventions (bisphosphonates), population (oncology and osteoporosis), areas of interest for the review (diagnosis, incidence, risk factors, treatment), and outcome (osteonecrosis of the jaw). All searches were limited to human studies published in the English language. The electronic search was updated January 26, 2008. The results of both database searches were combined and duplicate articles were excluded. We also searched the Cochrane Database of systematic reviews. A manual search of the bibliography of key published articles was also performed. In order to obtain additional unpublished data, personal communication with relevant experts was conducted and pharmaceutical companies were invited to submit relevant information. An electronic search of meeting abstracts of the American Society of Clinical Oncology and American Society of Hematology was also conducted.
Study selection.
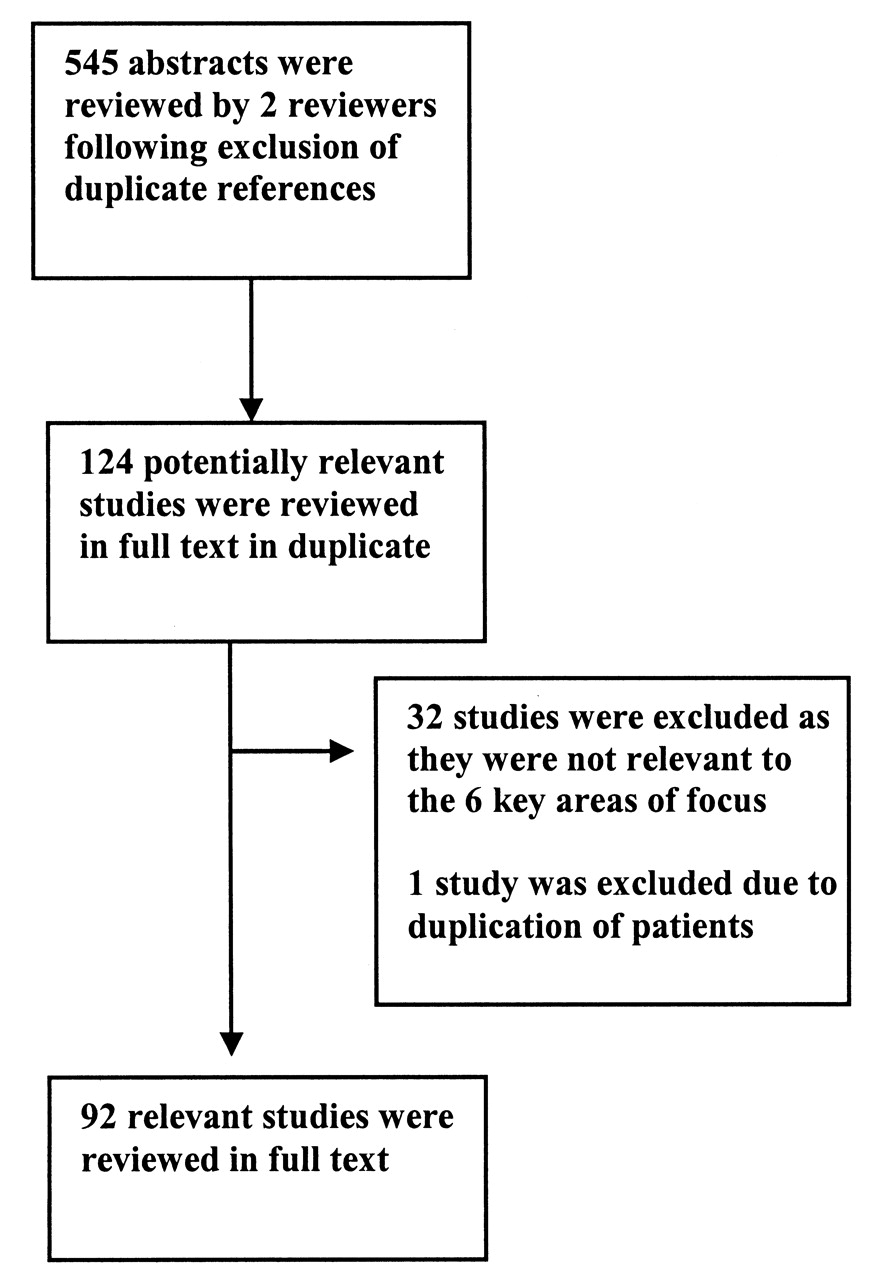
The search results were screened independently by 2 reviewers (FA, MA) using the title and abstracts. All the articles considered potentially relevant by either of the two reviewers were evaluated in full text. All original studies evaluating bisphosphonate associated osteonecrosis of the jaw in either the oncology or osteoporosis patient population of any age were included. Reviews and editorials addressing bisphosphonate associated osteonecrosis of the jaw were also included. Studies that were clearly not related to the 6 specific areas of interest were excluded. Study design was not used as a criterion for exclusion due to the paucity of high quality studies. Figure 1 summarizes the study selection process.
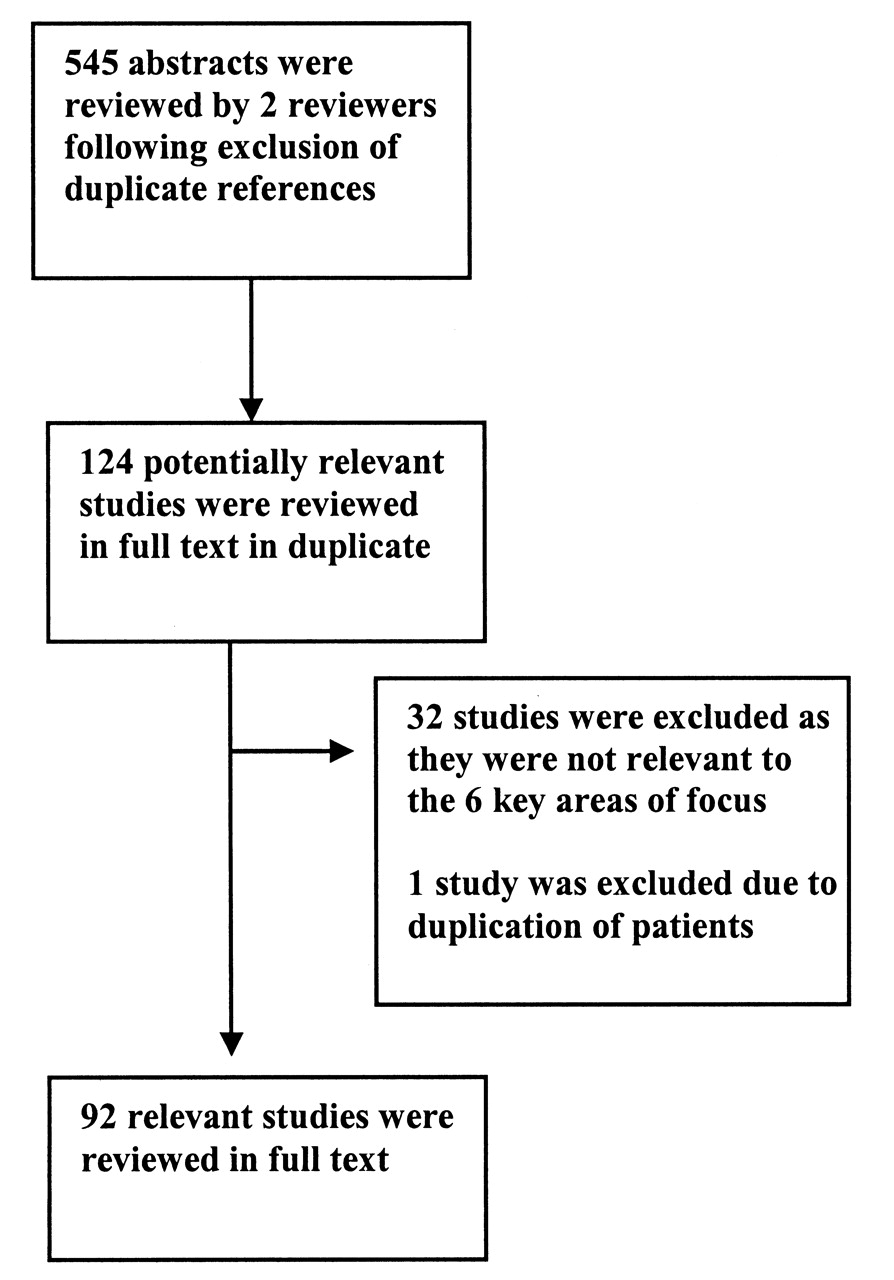
The article selection process.
Data synthesis and analysis.
The articles were sorted according to their corresponding key area of focus. Data abstraction was carried out independently by 2 reviewers (F. Amin, M. Alsahli) in duplicate. Disagreements were resolved by consensus, and when consensus could not be reached, by a third adjudicator (A. Khan). Studies were classified by their study design.
RESULTS
Ninety-two studies were included, consisting of 34 reviews, 18 case series, 16 case reports, 10 editorials, 2 prospective observational studies, 2 surveys, 8 comments and letters to editors, and 2 clinical guidelines.
DISCUSSION
There are very limited prospective data evaluating the true incidence of and the risk factors contributing to the development of bisphosphonate associated ONJ. The quality of evidence of many of the case reports is poor, and important patient information pertaining to risk factors and diagnosis was not included in the publication. Evidence regarding risk factors related to the development of ONJ is very weak at this stage and further study is required. The underlying pathogenesis resulting in the development of osteonecrosis with bisphosphonate use is not well defined at this stage. The incidence of osteonecrosis in the general population is currently not known. The incidence is estimated to be 1% to 12% in the oncology patient population receiving high-dose IV bisphosphonates, and appears to be dependent on dose and duration of bisphosphonate therapy. In the osteoporosis population, bisphosphonate associated ONJ is rare, with an estimated incidence of less than 1 case per 100,000 personyears of exposure. Conservative management addressing local infection, pain control, and maintaining adequate nutrition and hydration are advised. These recommendations are based on expert opinion due to the lack of prospective high quality data to guide recommendations for therapy.
What are the diagnostic features of ONJ associated with bisphosphonate therapy?
We identified 18 case series, 13 case reports, 2 surveys, and 2 clinical guidelines presenting the clinical features of bisphosphonate associated osteonecrosis at the time of diagnosis. The diagnosis is made clinically in the presence of exposed bone in the maxillofacial region for more than 8 weeks in the absence of radiotherapy to the jaw16. If the exposed bone has been present for less than 8 weeks, it should be followed to confirm that soft tissues close; such a case would be described as a suspected case of osteonecrosis16.
Clinical characteristics.
As the blood supply to the cortex is derived from the periosteum, the exposed bone is indicative of underlying necrotic bone. Sites of osteonecrosis can become secondarily infected and patients can present with local pain as well as soft tissue swelling and inflammation. The condition can progress to more severe lesions with development of draining fistulas; pathologic fractures may also occur17. The clinical diagnosis of osteonecrosis does not require histopathologic evaluation or radiographic features in order to confirm the diagnosis.
Role of diagnostic imaging in the diagnosis of bisphosphonate associated ONJ.
A retrospective study18 evaluated the radiographic features of bisphosphonate associated ONJ with dental panoramic radiographs and spiral computerized tomography (CT). Radiographic features may include sclerotic lamina dura around individual teeth, sclerotic bone over the mylohyoid ridge, widened periodontal ligaments, and/or regions of mottled bone in the jaw, most frequently in the molar/premolar regions19,20. There are no studies that indicate that these features are specific for the diagnosis of bisphosphonate associated ONJ20. ONJ is an imperfectly characterized syndrome, and the radiological findings represent a diverse spectrum.
In radiation induced ONJ, investigators had found few radiological signs of diagnostic or prognostic value. Epstein, et al21 studied the role of radiographic and nuclear imaging in evaluating postradiotherapy ONJ. Radiographic changes did not correlate with the clinical status of patients. All bone scans were abnormal at the time of diagnosis of osteonecrosis, but remained abnormal irrespective of treatment success or failure. Gallium-67 uptake did not aid in diagnosis, but persisting positive gallium scans seemed to indicate the need for surgery following hyperbaric oxygen therapy21.
Bisdasa, et al22 examined 32 patients with suspected bisphosphonate associated ONJ with unenhanced CT and contrast enhanced magnetic resonance imaging (MRI), and correlated their findings with surgical specimens. Osteonecrosis with Actinomyces infection was identified in the mandible of 18 patients, in the maxilla of 8 patients, and in both jaws in 6 patients. The CT findings were of mixed osteolytic and sclerotic regions in the jaws with or without periosteal new bone formation. The marrow space in the jaws was reduced. The T1 weighted MRI signal was hypointense in nearly all cases. The gadolinium enhanced MRI images revealed intensity changes in the cortical and subcortical bone structures in all patients. The T2 weighted MRI signal was hypointense on the affected side in 28 of 32 patients. Abnormal gadolinium enhancement was observed in the neighboring soft tissues, in all patients. A local reactive lymphadenopathy was also uniformly present. The authors concluded that bisphosphonate induced ONJ presents a wide variety of CT and MRI features that are readily recognized and help to determine the extent of the disease; however, they are not specific for the disease.
Similar findings have been reported by Phal, et al23, with the less common addition of poorly or nonhealing extraction sockets, periapical radiolucent areas, widening of the periodontal ligament space, osteolysis, sequestra, oroantral fistulae, soft tissue thickening, and periosteal new bone formation23.
In a radiological-pathological correlative study by Bedogni, et al, CT scans again showed increased bone density, periosteal reaction, and bony sequestrations in advanced disease24. Using MRI, exposed areas were found to have a low signal in T1 and T2 weighted and inversion recovery (IR) images, which suggests low water content, and histopathologically were correlated with acellularity and ischemia. Unexposed diseased bone was characterized by T1 hypointensity and T2 and IR hyperintensity, which suggests high water content and inflammation, associated with hypercellularity, osteogenesis, and hypervascularity resembling osteomyelitis. Thus, diseased bone extended beyond the limits of the bone exposed in the oral cavity. Histopathologic examination correlated well with CT and MRI scans, which are the choice for evaluation of bisphosphonate associated jawbone osteonecrosis, although the findings are not specific.
Since MRI and radionuclide bone scanning are effective in the early diagnosis of aseptic necrosis of the femoral head, before structural changes result, there was reason to hope that early imaging of the jaws might be productive in ONJ. This has not yet proved to be the case. When the disease is established the radiological findings are variable and nonspecific. The exposed and infected bone is of itself good evidence of ONJ so that for the present, pending some innovative approaches16, the best imaging method seems to be inspection with radiological techniques used to examine disease extent and potential complications.
Role of the histopathological examination.
The histopathologic examination can easily confirm the presence of necrotic bone. A tissue biopsy should be completed if metastatic disease is a potential diagnosis; however, it is not necessary for the clinical diagnosis of ONJ. The criteria for confirming ONJ in the setting of current or previous bisphosphonate use include the presence of exposed necrotic bone in the maxillofacial region for more than 8 weeks in the absence of a history of radiotherapy to the jaw16. Of note, this definition does not distinguish between lesions related to high-dose IV bisphosphonates in the oncology patient population and the lower doses given orally or intravenously in the osteoporosis population.
Differential diagnosis.
An important differential to consider in patients presenting clinically with ONJ is the “spontaneous sequestration” or “lingual mandibular sequestration with ulceration” that resolves spontaneously, which was identified in the pre-bisphosphonate era25–29. This is a less aggressive and self-limited pathologic process that develops without any obvious eliciting factor and is characterized by exposed necrotic bone involving the lingual mandible at the level of the mylohyoid ridge. Cases of lingual mandibular sequestration clinically appear similar to mild forms of bisphosphonate associated ONJ20. In addition to the similar clinical appearance, lingual mandibular sequestration has a propensity to develop in the posterior/lingual mandible similar to bisphosphonate associated ONJ26–31. Lingual mandibular sequestration and ulceration (LMSU) was first described in 1993 and reports of this condition indicate that it spontaneously resolves within a few days up to 12 weeks25. None of the patients with lingual mandibular sequestration have been taking bisphosphonates. The histopathologic examination has shown nonvital bone with zones of irregular resorption and associated bacterial masses. It appears, therefore, that there may be an overlap of cases of LMSU and bisphosphonate associated ONJ. The sites for the development of many cases of bisphosphonate associated ONJ are also similar to LMSU, being in the area of the mylohyoid ridge32. Further, as with LMSU, bisphosphonate associated ONJ may occur spontaneously without an inciting event in up to 25% of cases17.
Necrotic bone in bisphosphonate associated ONJ has been reported to show a paucity of Howship’s lacunae and reversal lines. These features are present in zones of bone resorption33. Additionally, the vital bone at the edge of necrotic zones has been found to exhibit enlarged osteoclasts with increased numbers of nuclei. This feature has also been observed in iliac crest bone biopsies from patients with osteoporosis treated with bisphosphonates34. Local infection with osteomyelitis can also present with exposed bone, as can periodontal disease, gingivitis, and local malignant lesions. A biopsy is recommended if local malignancy is a clinical consideration.
How common is bisphosphonate associated ONJ?
In a systematic review of bisphosphonate associated ONJ, Woo, et al identified at least 368 cases up to January 200635. Table 1 summarizes the existing reports. Use of high-dose IV bisphosphonate in oncology patients appears to be associated with a significantly greater risk of ONJ in comparison to the lower doses used in patients with metabolic bone disease (i.e., osteoporosis or Paget’s disease). For this reason, a separate analysis on the incidence of ONJ for each population was performed.
Reports on cases of osteonecrosis of the jaw.
Incidence of bisphosphonate associated ONJ among cancer patients.
We identified 6 studies assessing the incidence of bisphosphonate associated ONJ in the oncology patient population where it was possible to extract incidence data; a summary is given in Table 2. Estimates for the incidence of bisphosphonate associated ONJ varied substantially among the different studies, the cumulative incidence ranging from 1% to 12% at 36 months. Differences in study design may have contributed to the heterogeneity of these results. In order to evaluate incidence, the ideal study design is the prospective cohort study. There are only 2 such studies to date39,68, and a substantial number of cases were reported in duplicate in both studies. In addition, 3 studies estimated the incidence of bisphosphonate associated ONJ using survival analysis instead of providing raw incidence data. Thus, currently available incidence data for bisphosphonate associated ONJ are limited. As well, due to the lack of a standard definition and diagnostic criteria for bisphosphonate associated ONJ, it was difficult to assess its true incidence. It was only in July 2007 that the American Society of Bone and Mineral Research task force published a formal definition of bisphosphonate associated ONJ16. With the availability of a standard definition and the initiation of prospective studies, the incidence of bisphosphonate associated ONJ in oncology patients will be evaluable.
Cumulative incidence of bisphosphonate associated osteonecrosis of the jaw in the oncology patient population.
Incidence of bisphosphonate associated ONJ among patients with osteoporosis.
Roughly 4% to 5% of all cases of bisphosphonate associated ONJ reported in the literature have occurred in patients receiving oral bisphosphonates, as the majority have been in patients with cancer receiving high-dose IV bisphosphonates72. Due to the low incidence of bisphosphonate associated ONJ, it is challenging to assess its true incidence. Three studies37,38,73 estimating the incidence of this condition in the osteoporosis population were identified. In addition, postmarketing data for alendronate and risedronate were obtained by personal communication with industry officials.
A recent German study73 estimated the incidence of bisphosphonate associated ONJ in the non-oncology population as being less than 1 in 100,000. The denominator for this estimate, derived from a prescription database, encompassed all patients living in Germany who were prescribed bisphosphonates. The numerator consisted of all reported patients whose cases had been adjudicated by a single expert73. Recently, the incidence of ONJ was evaluated retrospectively from data assessing the effectiveness of IV zoledronate, a potent bisphosphonate, in the prevention of fracture in osteoporosis patients37. The incidence of ONJ was similar in the zoledronic acid and placebo groups, with only one case in each group (n = 3889 in placebo, n = 3876 in zoledronic acid) over a period of 3 years. These reports were validated by an adjudication committee.
A review of 114 cases of bisphosphonate associated ONJ in Australia noted that 72% of cases occurred in patients with bone malignancies38. In 73% of cases, the main trigger was a dental extraction. The frequency of ONJ in patients receiving bisphosphonates for osteoporosis was 0.01%–0.04%. After taking dental extractions into consideration in these patients, the frequency of bisphosphonate associated ONJ was found to be 0.09%–0.34%. In patients with bone malignancy, the frequency of ONJ was 1 in 87 (0.33%–1.15%) and in those who also had a recent dental extraction, 6.7%–9.1%38. It should be noted that the reported cases of ONJ in that study were identified by means of a retrospective postal survey, with no adjudicated diagnosis; this may have affected the accuracy of case ascertainment and the resulting incidence estimate. Postmarketing data regarding the incidence of bisphosphonate associated ONJ with alendronate use suggest an incidence of less than 1 in 100,00074. Similar estimated incidence data are reported for risedronate, at less than 1 per 100,00075. Following the market introduction of bisphosphonates, over 225 million total prescriptions have been dispensed in the US for alendronate, risedronate, and ibandronate, with 74% of these being for alendronate74. In summary, the incidence of bisphosphonate associated ONJ in the osteoporosis population appears to be substantially lower than that seen in the oncology population. However, as the number of patients taking bisphosphonates for osteoporosis and other metabolic bone diseases is much greater than the number of patients with cancer, even a low incidence of ONJ in osteoporosis may be significant and requires further evaluation. Thus, it is necessary to obtain prospective incidence data with stratification of risk factors for ONJ in osteoporosis patients. This also applies to the pediatric population, as currently being evaluated76.
Currently, there are no published incidence data for ONJ in Canada. A survey directed to all registered Ontario oral surgeons is currently in process; the study will provide urgently needed information on estimating the incidence of this condition in Ontario. Results are expected to be available in 2009.
What are the risk factors for bisphosphonate associated ONJ?
Our review identified 7 retrospective studies, 18 case series, 2 case reports, and 2 prospective observational studies describing risk factors for bisphosphonate associated ONJ. However, evaluation of risk factors for ONJ in these studies is limited to descriptive analyses. Therefore, the absolute and relative importance of the risk factors in bisphosphonate associated ONJ remain unknown.
Risk factors for osteonecrosis of the jaw.
Classical risk factors for development of ONJ include head and neck radiotherapy, periodontal disease, trauma, dental extraction, malignancy, chemotherapy, and glucocorticoid and high-dose IV bisphosphonate therapy. Local dental risk factors include areas of bone in the oral cavity that protrude and are covered by a relatively thin mucosa. These areas include mandibular or palatal tori1,17,25,77, exostoses, and the mylohyoid ridge1,17,25. In addition, ONJ has been reported to occur twice as often in the mandible in comparison to the maxilla1. Other dental risk factors are listed in Table 3. Risk factors for osteonecrosis include systemic conditions that may impede local vascularity (Table 4).
Dental risk factors for osteonecrosis of the jaw (ONJ).
Systemic and other risk factors for osteonecrosis of the jaw (ONJ).
Future studies, including post-hoc regression analysis of the different risk factors reported to date, are needed in order to determine which risk factors are more strongly associated than others in the development of ONJ and bisphosphonate associated ONJ.
Risk factors for bisphosphonate associated ONJ among oncology patients receiving high-dose IV bisphosphonate therapy.
By definition, all patients with bisphosphonate associated ONJ have been treated with a bisphosphonate. Studies indicate that the risk of ONJ appears to be related to the potency, dose and duration of bisphosphonate therapy2,3,17,38,39,40,68. For example, the incidence of ONJ was significantly higher in patients using zoledronic acid alone than in patients treated with other IV bisphosphonates or combinations16,38,40.A number of studies indicate that highdose IV zoledronic acid may be more closely associated with osteonecrosis of the jaw than use of pamidronate, other IV bisphosphonates or combinations39,48,66,68,83. The duration of bisphosphonate treatment also appears to affect the risk of ONJ. This is supported by the increase in the cumulative incidence of ONJ over time in studies evaluating the incidence at different points (Table 2). In addition, Bamias and colleagues, in a prospective cohort of 252 patients with metastatic bone disease, found that the median number of infusions of pamidronate or zoledronic acid were significantly higher (35 infusions) in patients who developed ONJ than in those who did not (15 infusions)39.
Risk factors for bisphosphonate associated ONJ among patients with osteoporosis receiving low-dose bisphosphonate therapy.
The ONJ lesions in this population appear to be less severe and more likely to resolve than those found in the oncology patient population receiving high-dose IV bisphosphonate therapy. In the osteoporosis population, it is not known if the incidence of ONJ differs from that seen in the general population17,19,84,85. Hence, it remains unclear whether the lower dose of bisphosphonates used in the management of osteoporosis results in any increase in the risk of ONJ beyond what is observed in the general population. At this time there is insufficient evidence to confirm a causal link between the doses of bisphosphonates used for osteoporosis treatment and ONJ.
Can we prevent bisphosphonate associated ONJ?
Currently, there is insufficient evidence to answer this question. Published data addressing the relationship between suspected risk factors and ONJ are weak. It is not known how those risk factors that have been identified interact, making it difficult to develop prevention strategies. Prospective data will enable the development of evidence based recommendations and stratification of risk. Two guidelines containing recommendations for prevention have been published86,87.
How do we stage established bisphosphonate associated ONJ?
There are no published studies addressing staging of bisphosphonate associated ONJ. Although staging criteria have been proposed by a number of experts1,17,19,32, these have been based on case studies or case series as there are no randomized clinical trials available to assist in outlining staging criteria or establishing recommendations for management of this condition.
The American Association of Oral and Maxillofacial Surgeons 3-stage criteria for bisphosphonate associated ONJ are based upon patient symptoms and clinical findings1. Limitations of this system are that it does not take into account the size of the lesion or any variation that may exist in the number of lesion sites. The proposed treatment strategies do not take into consideration the presence of clinical risk factors affecting the development of ONJ, such as the dose of the bisphosphonate, the presence of mobile segments of bony sequestrum, symptomatic dentition issues within the region of ONJ, or systemic conditions permitting cessation of drug therapy. Although early progress has been made toward developing a useful staging system for ONJ, it is clear that there is a need for controlled clinical studies, in order to provide clinicians with appropriate guidelines applicable to clinical practice. One such proposal would include a multifactorial staging system taking into account cumulative dose and duration of therapy (oral vs IV bisphosphonates), the site(s) of the lesion(s), overall size (cm) of the lesion(s), and clinical symptoms. This type of staging criteria then would allow development of a more specific treatment regimen for easy use by clinicians. Until such data are available to allow development of a more useful staging system, the Canadian ONJ Task Force recommends that physicians adopt these recommendations1.
How should we treat established bisphosphonate associated ONJ?
Today, the published recommendations are based solely on expert opinion and anecdotal experience. Conservative treatment approaches have proven to be most effective1,17,18. It must be emphasized, in all cases, that management of patients diagnosed with established ONJ should be provided by an appropriate dental specialist, such as an oral and maxillofacial surgeon17. The goals of treatment are 3-fold.
(1) To educate and reassure each patient regarding potential ONJ complications; dietary counselling and advice regarding appropriate supplements and/or tube feeding for patients with limited ability to eat due to the oral lesions.
(2) To eliminate discomfort, pain, and secondary infection: baking soda with water or an antimicrobial mouth rinse to clean and irrigate the exposed sites is advised. Microbiological culture for secondary infection has been suggested35. Treatment for ONJ stage 2 or higher should focus on pain control and on preventing the progression of exposed bone. Recommendations include a 3-week course of penicillin V potassium (Pen V-K) with the addition of metronidazole as necessary, in addition to 0.12% chlorhexidine mouth rinse. Clindamycin, doxycycline, and erythromycin also have been used in patients who are allergic to penicillin1.
(3) To attempt to arrest the progression of bone exposure: for this purpose it is recommended that one eliminate sharp and ragged bone surfaces with surgical debridement, thereby minimizing trauma to adjacent soft tissues. Mobile or readily identifiable sequestrae should be removed, so that uninvolved bone is not exposed. Extraction of symptomatic teeth in the necrotic zone is not believed to exacerbate established ONJ. Aggressive debridement otherwise is contraindicated. Segmental resection may be required to remove large portions of necrotic or pathologically fractured bone, along with immediate reconstruction using a reconstruction plate. Bone grafting may be problematic, due to potential bone necrosis at the recipient site. Protecting the site by means of a removable prosthesis has also been suggested88. Biopsy is advised only if metastasis is suspected. There are limited data regarding the value of hyperbaric oxygen therapy in the management of bisphosphonate associated ONJ89–94. This treatment modality may be of benefit in achieving regrowth of oral mucosa over previously exposed bone; however, this requires further prospective study. Interruption of bisphosphonate therapy has also been suggested1. Discontinuation of IV bisphosphonate therapy in cancer patients with ONJ has been associated with healing in case reports, suggesting that resolution of ONJ in these patients may be accelerated by cessation of bisphosphonate therapy95. In a recent review of 60 cases of ONJ, 7 patients demonstrated improved outcomes with cessation of bisphosphonate therapy over at least 6 months89. As current data are insufficient to support or refute this recommendation, any decision regarding interruption of bisphosphonate therapy (IV or oral) should be made in consultation with the treating oncologist or physician.
Future directions for reeasrch
Prospective data are urgently needed for the development of a comprehensive understanding of the pathophysiology of bisphosphonate associated ONJ. It is also necessary to improve our knowledge of the incidence of ONJ in the general population, as well as in the population exposed to both low- and high-dose bisphosphonate therapy. The effects of longterm administration of high-dose bisphosphonates require further study in the oncology population, with review of current guidelines addressing bisphosphonate use in the oncology population. Prospective data will enable stratification of the risk factors leading to osteonecrosis, and enable a more accurate assessment of prognosis. New imaging modalities may be of value in identifying the condition early, allowing targeted intervention, and this requires further study.
Diagnostic coding specifically indicating ONJ with sub-codes for users and nonusers of bisphosphonates is recommended. This would be of great value in improving the recording of this condition in healthcare databases, allowing further analysis of incidence, risk factors, and prognosis. A registry of all new cases in Canada is recommended and is being planned by the Canadian task force on bisphosphonate associated ONJ. International collaboration with a standardized and unified approach to research is necessary for the development of a successful diagnostic and management strategy for this uncommon condition.
Conclusions
This systematic review indicates that high-dose IV bisphosphonate use in the oncology population is associated with an increased risk of osteonecrosis that appears to be dependent on dose and duration of therapy. A similar link has not been confirmed with lower-dose bisphosphonate therapy in the osteoporosis population. The incidence of ONJ in the general population is not known. ONJ can occur in the absence of bisphosphonates or other important risk factors such as radiotherapy, chemotherapy, and glucocorticoid use. In these circumstances, ONJ appears to resolve spontaneously and appears to be a benign process. Further studies are needed to fully understand the pathogenesis and incidence of bisphosphonate associated ONJ. The agreed-upon definition of bisphosphonate associated ONJ for both suspected and confirmed cases will be of value in improving the homogeneity of future studies. Current management strategies include addressing pain control and local infection, and maintaining hydration and adequate nutrition. Conservative management of oral lesions is recommended, with surgery being limited to removal of loose sequestra, smoothing of rough bone edges, and removal of necrotic debris. Further research will build on current knowledge and enable the development of more sophisticated and effective management plans.
Appendix 1. Search strategy

Footnotes
-
Supported by the Foundation for Continuing Education and Research of the Canadian Association of Oral and Maxillofacial Surgeons, the Oral and Maxillofacial Surgery Foundation of Canada, and the Calcium Disorders Clinic, St. Joseph’s Healthcare, Hamilton, McMaster University, Hamilton, Ontario, Canada.
- Accepted for publication August 19, 2008.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.
- 7.
- 8.
- 9.
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.
- 28.
- 29.↵
- 30.
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.
- 91.
- 92.
- 93.
- 94.↵
- 95.↵








{kind=link}