

Intraosseous lipoma is an extremely rarely diagnosed benign bone tumor. In most cases diagnostic imaging techniques, namely computed tomography (CT) and magnetic resonance imaging (MRI) are sufficient to reach a diagnosis, which in some cases is confirmed by postsurgical or postmortem histological examination. We describe 2 cases of intraosseous lipoma that were identified by practising rheumatologists at our rheumatology clinic.
A 38-year-old man presented with pain in his right foot, ankle, knee, and first metatarsophalangeal joint. His history featured trauma-induced fractures of the left ankle and the right 6th rib. He did not recall any recent infection, travel, exertion, or other illness. Examination including musculoskeletal examination yielded no significant findings. Laboratory tests including metabolic panel and parathyroid hormone values were normal. Conventional radiographs of the right ankle and foot revealed a round, translucent, cystic lesion in the right calcaneal diaphysis in the trabecular bone, with areas of calcification (Figure 1a). CT scan of the lesion showed complete resorption of bone within the lesion, with the remaining tissue showing a fat attenuation level (–77 Hounsfield units; Figure 1b). The presence of fat within the lesion ruled out the diagnosis of intraosseous gouty tophus. On T1-weighted MRI scans the well delineated lesion appeared to be isointense with subcutaneous fat (Figure 1c), while significantly lower signal intensity was observable on T2-weighted images (Figure 1d).

a. Plain radiograph. b. CT scan. c. T1-weighted MRI scan. d. T2-weighted MRI scan of the right ankle. Arrows show the lesion.
The second patient, a 61-year-old man, had a history of sport-related injuries culminating in meniscectomies carried out on both knees. He also suffered a trimalleolar fracture of the right ankle in 2002, but presented at our clinic in 2003 with pain in the left hip. He reported slight difficulty walking. Examination including musculoskeletal examination yielded no abnormality, but the anteroposterior radiograph of the pelvis revealed a round lesion in the other femoral head (diameter 30 mm; Figure 2a), where he had not complained of symptoms. Laboratory tests including metabolic panel and parathyroid hormone values were normal. The lesion resembled a “black hole” when viewed under CT (Figure 2b), with a main Hounsfield unit of –63 that corresponded to adipose tissue. The lesion appeared to be isointense with subcutaneous fat on T1-weighted MRI scans and exhibited low signal intensity with fat suppression on T2-weighted images (Figure 2c, 2d).
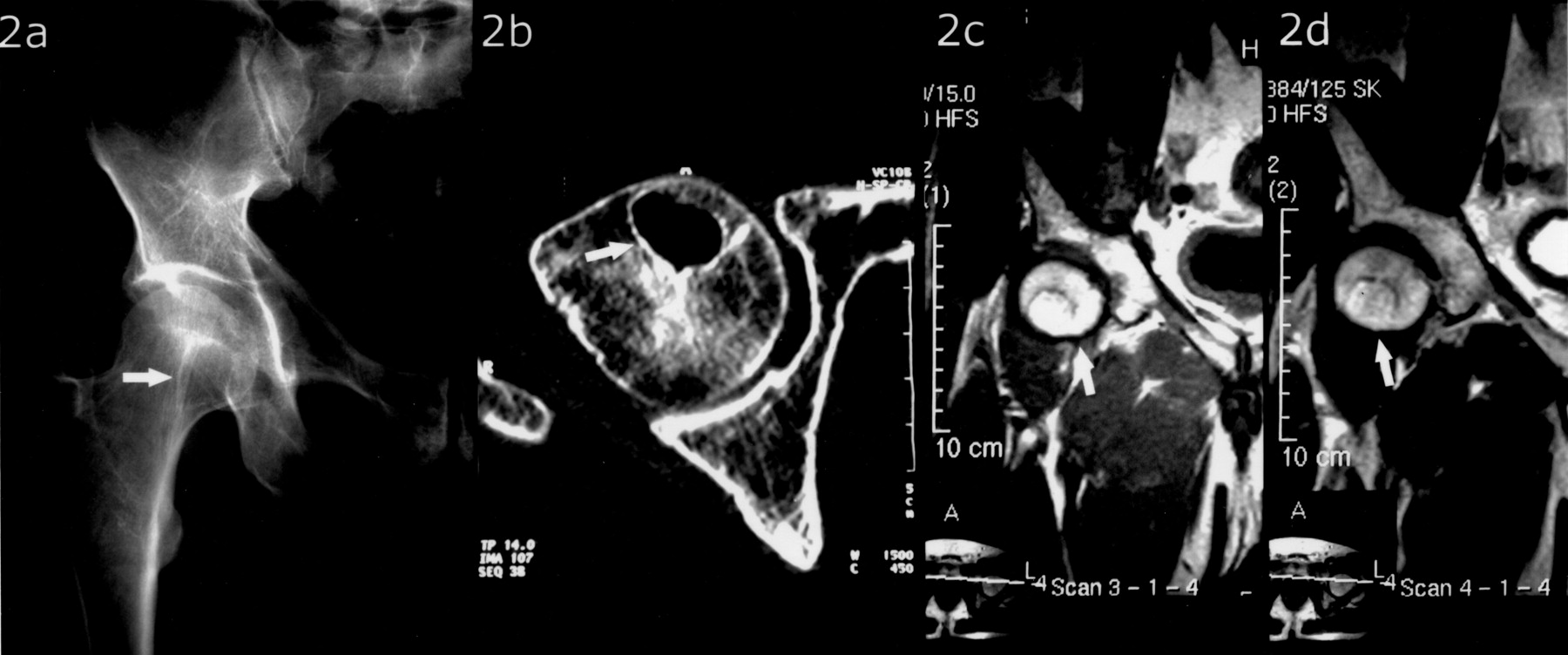
a. Plain radiograph. b. CT scan. c. T1-weighted MRI scan. d. T2-weighted MRI scan of the right femoral head. Arrows show the lesion.
Intraosseous lipomas are rare benign neoplasms that represent proliferation of fat tissue within the marrow of normal trabecular bone1. Intraosseous lipomas occur primarily in the long bones of the lower extremities (i.e., femur, tibia, calcaneus), which are characterized by a scarcity of trabecular bone. They can also occur in the flat bones, pelvis, and other locations2,3. Milgram classified intraosseous lipomas according to the degree of involution (necrosis, calcification, cyst formation, and reactive ossification) observable in the lesion. Based on this classification intraosseous lipomas were categorized into 3 types — Stage 1 tumors consisting of viable fat cells; Stage 2 tumors composed partly of viable fat cells also demonstrating fat necrosis and calcification; and Stage 3 lesions with full range of involution: necrotic fat, calcification of necrotic fat, variable degrees of cyst formation, and reactive woven bone formation4. Typically, plain radiographs suggest the diagnosis, which is subsequently confirmed by CT or MRI with fat-suppression sequences5.
In both of our cases plain radiographs showed round, translucent, cystic lesions with sclerotic margins. A classical appearance of intraosseous lipoma of the calcaneus is the presence of central calcification within a well defined lytic lesion resembling a cockade. The calcaneal lesion seen in Patient 1 also showed similar areas of increased radiographic density due to fat calcification. CT scans showed complete resorption of bone within the lesions, with the remaining tissue showing a fat attenuation level (–77 and –63 Hounsfield units, respectively). A hypointense rim was observable surrounding both lesions, consistent with reactive sclerosis. Both lesions appeared to be isointense, with subcutaneous fat on T1-weighted MRI scans exhibiting low signal intensity with fat suppression on T2-weighted images. The 2 cases correspond to stage 2 and stage 1 intraosseous lipomas, respectively, according to Milgram’s classification.
Modern imaging techniques have proven to be reliable in the diagnosis of intraosseous lipoma6. In some cases fatty involution of an aneurysmal bone cyst, or bone infarct, may not be ruled out unequivocally7; malignant tumors and the malignant transformation of benign lesions should also be considered8. In such cases a guided biopsy is required for the correct diagnosis. Complete removal is indicated in cases leading to potential pathological fractures. In the majority of cases lipomas run an indolent course, and can be followed by a wait and scan approach9. Due to the unequivocal diagnosis based on imaging modalities and lack of clinical progression over a course of more than 5 years, our 2 cases did not require biopsy or surgery, with followup consisting of regular scans.








{kind=link}
{kind=link}