

Abstract
Objective. Early recognition and treatment of pediatric rheumatic diseases is associated with improved outcome. We documented access to pediatric rheumatology subspecialty care for children in British Columbia (BC), Canada, referred to the pediatric rheumatology clinic at BC Children’s Hospital, Vancouver.
Methods. An audit of new patients attending the outpatient clinic from May 2006 to February 2007 was conducted. Parents completed a questionnaire through a guided interview at the initial clinic assessment. Referral dates were obtained from the referral letters. Patients were classified as having rheumatic disease, nonrheumatic disease, or a pain syndrome based on final diagnosis by a pediatric rheumatologist.
Results. Data were collected from 124 of 203 eligible new patients. Before pediatric rheumatology assessment, a median of 3 healthcare providers were seen (range 1–11) for a median of 5 visits (range 1–39). Overall, the median time interval from symptom onset to pediatric rheumatology assessment was 268 days (range 13–4989), and the median time interval from symptom onset to referral to pediatric rheumatology was 179 days (range 3–4970). Among patients ultimately diagnosed with rheumatic diseases (n = 53), there was a median of 119 days (range 3–4970) from symptom onset to referral, and 169 days (range 31–4989) from onset to pediatric rheumatology assessment.
Conclusion. Children and adolescents with rheumatic complaints see multiple care providers for multiple visits before referral to pediatric rheumatology, and there is often a long interval between symptom onset and this referral.
For children ultimately diagnosed with rheumatic disease, there may be several intermediary referrals or logistic delays after contact with their initial primary healthcare provider and before being seen by a pediatric rheumatologist for assessment, diagnosis, and treatment. Yet early detection and intervention are thought to optimize outcome for most rheumatic conditions, ranging from potentially fatal vasculitides to morbidities such as uveitis associated with juvenile idiopathic arthritis (JIA)1,2.
Canadian standards for access to pediatric rheumatology care do not exist. The Canadian Rheumatology Association consensus statement on treatment of early rheumatoid arthritis (RA) advocates early referral to an arthritis specialist3. The Alliance for the Canadian Arthritis Program (an alliance of arthritis patients, volunteer associations, caregivers, healthcare providers, researchers, government, and industry) recently recommended the identification and treatment of any inflammatory arthritis within 4 weeks of seeing a healthcare professional, and provisionally recommended timely access to integrated age- and stage-appropriate healthcare4. This guideline did not explicitly address the issue of rheumatic disease in children. The American College of Rheumatology has developed guidelines for referral to pediatric rheumatologists, but these guidelines do not address referral times1.
Time intervals from symptom onset to initial pediatric rheumatology assessment in Canada are beginning to be described5; however, the route and time delay prior to pediatric rheumatology evaluation in Canada remain poorly delineated. Our study was conducted to document the pathways to pediatric rheumatology subspecialty care for children in British Columbia (BC), Canada. We report an audit of children referred to the pediatric rheumatology clinic at BC Children’s Hospital (BCCH) in Vancouver.
MATERIALS AND METHODS
Patients and data collected
An audit was conducted of all new outpatients seen in the pediatric rheumatology clinic at BCCH during a period of 10 months (May 2006 to February 2007). BCCH is the sole tertiary referral pediatric hospital in the province of BC. Patients were excluded from this study if they had previously seen a pediatric rheumatologist, were seen as inpatient consultation, or were seen in the emergency room. After giving informed consent, parents completed a questionnaire designed for this study through a guided interview at the initial pediatric rheumatology clinic assessment. The questionnaire was administered by a physician assessing the patient.
Information collected included: the month and year of symptom onset, the month and year of first healthcare provider visit, the number of healthcare providers seen for the complaint, and whether the family perceived that there had been a delay in accessing the pediatric rheumatology clinic (Yes or No). The date of referral to pediatric rheumatology (obtained from the referral letter from the referring physician) and the date of initial clinic assessment were recorded. Healthcare provider was broadly defined to include family physicians, specialists, nurse practitioners, physiotherapists, chiropractors, and naturopaths. Referral by a physician is required for evaluation in the pediatric rheumatology clinic. Based on the final diagnosis given by a pediatric rheumatologist, patients were subsequently classified as having rheumatic disease, nonrheumatic disease, or a pain syndrome. Rheumatic diseases included inflammatory and autoimmune diseases such as JIA, reactive arthritis, poststreptococcal arthritis, all forms of vasculitis, systemic lupus erythematosus, sarcoidosis, linear scleroderma, morphea, Raynaud’s disease, and cutaneous lupus. Nonrheumatic conditions included mechanical disorders such as pes planus or patellofemoral pain, and transient symptoms that resolved. Pain syndromes included complex regional pain syndromes and diffuse idiopathic pain syndromes. Baseline data on disease activity, functional disability, or additional interventions required at the initial pediatric rheumatology assessment were not collected during this study.
Analysis
Data analyses were performed using the Statistical Package for the Social Sciences v10 (SPSS Inc.). Time intervals for date of symptom onset to first healthcare provider visit, first healthcare provider visit to referral, and referral to first pediatric rheumatology clinic visit were calculated. Only month and year of symptom onset, and month and year of initial healthcare provider contact could be recalled reliably. Thus for the purposes of this study, the date of onset of symptoms was assumed to be the 1st of the month, and the date of initial healthcare provider visit was assumed to be the 15th of the month, unless a referral letter had been received prior to the 15th of the month, in which case the date of receipt of the referral letter was recorded as the date of first healthcare provider visit. Time intervals are reported as median number of days, with ranges. Timeto-event curves were calculated with Kaplan-Meier survival analysis methods, and the log-rank test was used to compare time to event among different diagnostic categories. The Mann-Whitney test was used to compare median time intervals for patients with JIA versus other rheumatic diseases. Kruskal-Wallis testing was used for exploratory analyses of time intervals according to referral source, and p values for these analyses were not corrected for multiple comparisons due to the exploratory design.
RESULTS
Study population
A total of 124 out of 203 eligible new patients (61%) participated. The mean age at initial pediatric rheumatology assessment was 11.0 ± 4.5 years; 73% were female. Rheumatic disease was diagnosed in 53 patients (43%), nonrheumatic condition in 57 (46%), and a pain syndrome in 14 (11%). The distribution of age, sex, and diagnostic categories did not differ between study participants and nonparticipants (data not shown). Among the patients diagnosed with a rheumatic disease, 35 (66%) were diagnosed with JIA. Due to small patient numbers, data were not analyzed by JIA subtype.
Healthcare contacts prior to pediatric rheumatology assessment
Patients saw a median of 3 different healthcare providers (range 1–11) for a median of 5 visits (range 1–39) before seeing a pediatric rheumatologist. This did not differ significantly among patients with rheumatic diseases, nonrheumatic diseases, and pain syndromes. Although healthcare provider was broadly defined to include chiropractors, naturopaths, and others, parents invariably reported the date of first physician contact as the date of their child’s first healthcare provider visit.
Time intervals in the referral process
The median number of days between points in the referral process from symptom onset to the first pediatric rheumatology assessment are shown in Figure 1. A median time of 14 days (range 3–3513) elapsed from symptom onset to first healthcare provider visit; and 107 days (range 0–4956) from first healthcare provider visit to pediatric rheumatology referral. There was a median of 42 days (range 3–175) from referral to attending the pediatric rheumatology assessment. Overall, the median time interval from symptom onset to pediatric rheumatology assessment was 268 days (range 13–4989), and the median time interval from symptom onset to referral to pediatric rheumatology was 179 days (range 3–4970). The distributions of the first 360 days of these time intervals are shown in Figure 2. There were significant outliers in both the time from symptom onset to first healthcare provider visit and the time from first healthcare provider visit to pediatric rheumatology referral.

Median time intervals, days (range), for all patients for each point in the referral process from symptom onset to first pediatric rheumatology assessment. HCP: healthcare provider.

Distributions of time intervals in the referral process. Data from the first 360 days of each time interval are shown. A. Time from symptom onset to first healthcare provider visit (6 patients had an interval > 360 days). B. Time from first healthcare provider visit to pediatric rheumatology referral (33 patients had an interval > 360 days). C. Time from referral to pediatric rheumatology assessment (all patients were seen within 360 days of referral).
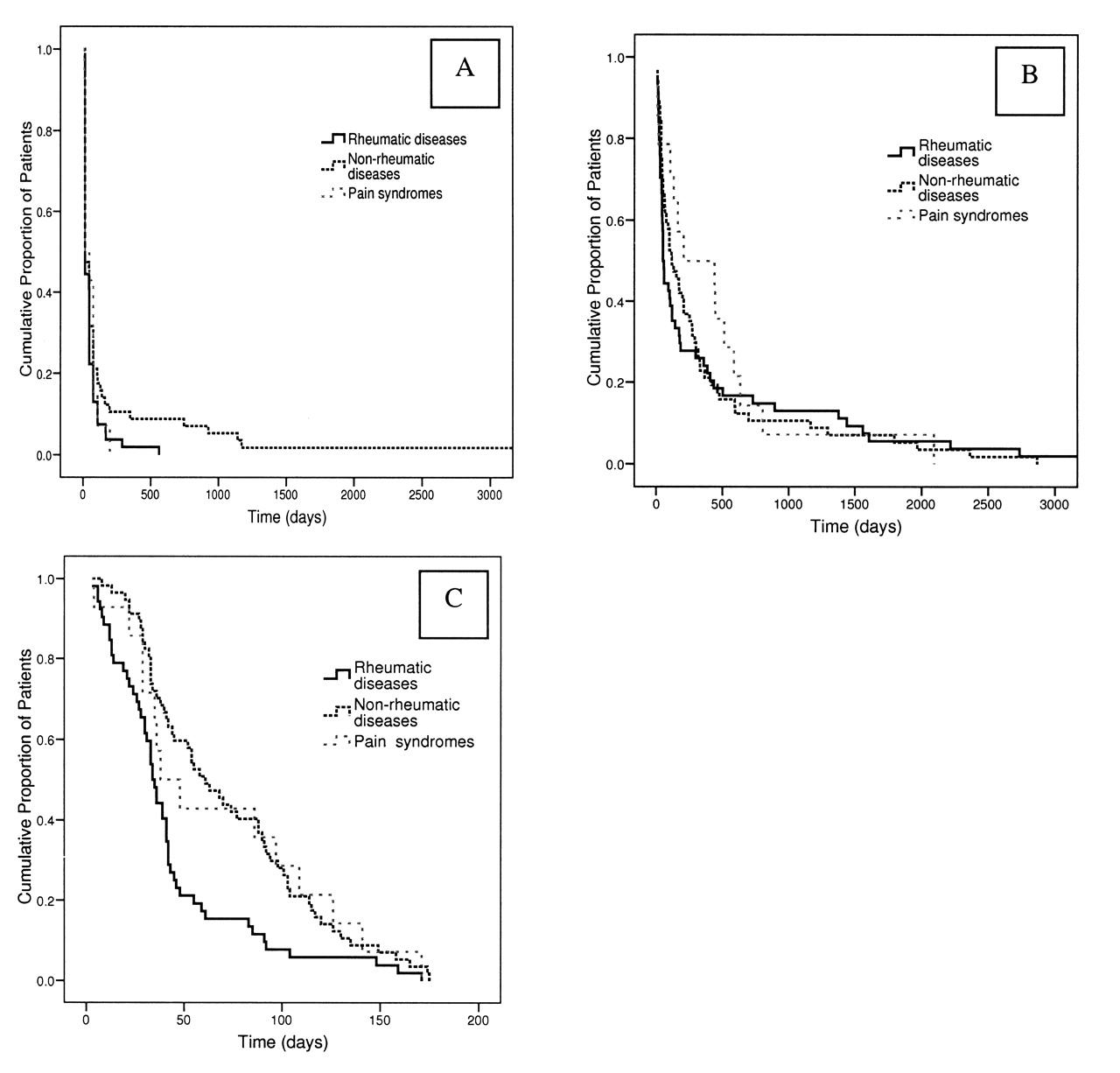
These time intervals were compared among the diagnostic categories (Table 1). Among patients ultimately diagnosed with rheumatic diseases, there was a median of 119 days (range 3–4970) from symptom onset to referral, and 169 days (range 31–4989) from onset to pediatric rheumatology assessment. Log-rank survival analysis did not show any difference among diagnostic categories for the time from symptom onset to first healthcare provider visit or time from first healthcare provider visit to pediatric rheumatology referral (Figure 3A, 3B). There was a significant difference among the diagnostic categories for the time interval from referral to pediatric rheumatology assessment (Figure 3C), with patients diagnosed with rheumatic diseases seen earlier than those with nonrheumatic complaints or with pain syndromes. This difference for the time interval from referral to pediatric rheumatology assessment was the same for patients included in the study and eligible patients who did not complete the study (data not shown).

Kaplan-Meier analysis of time intervals in the referral process comparing patients ultimately diagnosed with rheumatic diseases, nonrheumatic diseases, and pain syndromes. A. Time from symptom onset to first healthcare provider visit. B. Time from first healthcare provider visit to pediatric rheumatology referral. C. Time from pediatric rheumatology referral to first pediatric rheumatology assessment. There were no differences among diagnostic categories in A (log-rank p = 0.203) and B (logrank p = 0.675). There was a significant difference among diagnostic categories in C (log-rank p = 0.003), in keeping with our triage system.
Median time intervals in days (range) by diagnostic category for each point in the referral process from symptom onset to first pediatric rheumatology assessment. HCP healthcare provider.
The time intervals between symptom onset and pediatric rheumatology assessment for children with JIA did not differ from those of children with other rheumatic diseases. Two patients with JIA were taking disease modifying antirheumatic drugs at the time of their initial pediatric rheumatology appointment, both of whom had inflammatory bowel disease. A third patient had previously been treated with a short course of hydroxychloroquine. Only one patient with JIA (enthesitis-related arthritis) had seen an ophthalmologist prior to the first pediatric rheumatology assessment.
Exploratory analysis (Kruskal-Wallis testing) showed that neither the overall median time from symptom onset to pediatric rheumatology assessment for all study patients, nor the time from initial healthcare provider assessment to pediatric rheumatology referral differed among patients referred by general practitioners, pediatricians, or other physicians (data not shown). However, there was a significant difference in the time from referral to first rheumatology assessment according to the referral source (p = 0.001). The median number of days from referral to pediatric rheumatology assessment for patients referred by general practitioners was 86 days (range 7–175), for those referred by pediatricians this interval was a median of 35 days (range 3–174), and for those referred by other physicians this median time was 43 days (range 12–165).
Exploratory analysis was also performed on the subset of patients ultimately diagnosed with a rheumatic disease (n = 53) according to whether the patient was referred by a general practitioner (GP), pediatrician, or other physician. There was a significant difference (p = 0.044) in the median time interval from symptom onset to first pediatric rheumatology assessment: among GP 269 days (range 51–4989), pediatricians 96 days (range 31–2790), and other physicians 298 days (range 57–2476). There was also a significant difference (p = 0.029) in the median time interval from symptom onset to initial healthcare provider visit: in GP 14 days (range 14–560), pediatricians 14 days (range 3–287), and other physicians 45 days (range 14–1170). There was no significant difference in the median time interval from initial healthcare provider visit to pediatric rheumatology referral: GP 121 days (range 0–4956), pediatricians 45 days (range 0–2736), and other physicians 126 days (range 0–2217).
Perception of delay
Thirty-six percent of all families surveyed felt that there had been an undue delay at any point prior to their first pediatric rheumatology appointment. The perception of delay was not correlated with longer time from onset to first pediatric rheumatology assessment, or with diagnostic category (data not shown).
DISCUSSION
Our study shows that children and youth with rheumatic diseases in BC wait a median of 119 days (about 4 months) from symptom onset before being referred to pediatric rheumatology care, and see a median of 3 healthcare providers during that time. Some children saw as many as 11 healthcare providers before a definitive rheumatic diagnosis was given.
There are multiple steps affecting the referral process contributing to the time interval between symptom onset and a subspecialist appointment. The family or caregiver must recognize the symptoms and have sufficient concern to visit a healthcare provider. For patients with RA in the UK, patient-related factors resulting in delays presenting to primary care providers contribute significantly to long intervals prior to subspecialist appointments6. Ease of access to a healthcare provider at this stage could potentially further contribute to a decision as to when to seek the advice of a healthcare provider.
Poor physician competence or confidence in assessing for rheumatic diseases may delay the referral process. Many physicians at all levels of training do not feel skilled at performing pediatric musculoskeletal examinations7–9. Studies from Canada5, the United Kingdom10, and Australia11 have documented the interval from symptom onset to evaluation by a pediatric rheumatologist. In Saskatoon, Canada, 61.2% of 836 children and adolescents referred to the pediatric rheumatology clinic were seen within 2 months of symptom onset, 22.8% between 3 and 6 months, 11.3% between 7 and 12 months, and 4.7% after 12 months. The mean interval between symptom onset and first rheumatology assessment was 2.57 months when outliers with an interval > 12 months were excluded5. In the UK, a retrospective 3-year study documented a median time interval of 20 weeks from onset to first pediatric rheumatology appointment among patients with JIA10. An audit of newly diagnosed patients with JIA in Western Australia showed a mean time interval of 39.9 weeks from onset to first pediatric rheumatology subspecialty appointment11.
In our study, the median time from symptom onset to first rheumatology assessment was 268 days for all patients (38.3 weeks). The Saskatoon study included patients seen in a variety of hospital settings in Saskatoon, including inpatients and the emergency department. Inpatients and emergency room consultations are seen quickly, and our longer time interval from onset to the initial pediatric rheumatology appointment is partly explained by the fact that our study was restricted to outpatient referrals. Similar to results for patients with JIA from the UK, our patients ultimately diagnosed with rheumatic disease had a shorter, but still suboptimal, median time interval of 169 days (24.1 weeks) from symptom onset to subspecialty appointment, and this time interval did not differ in our patients with JIA. Additionally, in the UK, children with JIA saw multiple specialists prior to pediatric rheumatology assessment, yet had not received appropriate and critical services needed for the care of their JIA, such as ophthalmology screening, occupational therapy, or physiotherapy. Consistent with these findings, only one of our newly referred patients with JIA had seen an ophthalmologist.
The interval between the primary healthcare visit and the referral to pediatric rheumatology is of particular interest. Ideally, this period should be short for patients with rheumatic diseases, if their diagnoses were promptly recognized by a primary healthcare provider. Delay in referral to a pediatric rheumatologist may be influenced by the travel distance required to obtain the consultation and accessibility of other specialties such as adult rheumatology. For example, in the United States, adult rheumatologists often treat pediatric rheumatic diseases in areas where pediatric rheumatology subspecialty care is lacking12,13. Local availability of rheumatologists was associated with increased utilization of musculoskeletal-related services in a cohort of adult patients with arthritis and rheumatism-related complaints14. Comparable data are not available for children with pediatric rheumatic diseases in Canada. Interestingly, exploratory analysis of our data showed a significant difference in time from symptom onset to initial pediatric rheumatology assessment according to referral source for patients ultimately diagnosed with rheumatic diseases; however, we did not collect information about the specific order of healthcare provider contacts seen prior to pediatric rheumatology clinic assessment, and thus cannot draw conclusions about the specific pathways leading to a referral to our subspecialty clinic.
Once a referral is made to our clinic, patients are triaged based on the information provided by the referring physician into one of 3 categories, with the goal that “urgent” patients are seen within 1–2 weeks, “semi-urgent” patients are seen within 4–6 weeks, and “non-urgent” patients are seen within 4–6 months. Triage occurs through an informal weekly review of all new patient referrals by the attending pediatric rheumatologist on service. Although insufficient referral information may potentially delay referral of children ultimately diagnosed with rheumatic disease, in our setting such children were seen sooner than children without rheumatic disease, supporting the continued use of our triage process.
Limitations of this study include the relatively small number of subjects, particularly in the idiopathic pain category, and the potential inaccuracies associated with parental recall bias. Results may be skewed because not all new patients were identified in this study during the data collection period; although neither the distribution of patients among the 3 disease categories (rheumatic diseases, nonrheumatic diseases, and pain syndromes) nor the time from referral to initial pediatric rheumatology assessment by diagnostic category differed between study subjects and nonparticipants. We do not know how many primary healthcare providers or other specialists care for children with rheumatic disease without referring them to pediatric rheumatology at BCCH, but we suspect the number is small. It is not known whether the long time interval prior to subspecialty assessment is part of a global problem for access to subspecialty care for children in BC because data are not available for other subspecialties.
Our study documents a long time interval from symptom onset to subspecialty assessment in pediatric patients with rheumatic complaints in BC. The times are well in excess of the standards proposed by the Canadian Arthritis Program for inflammatory joint disease. Further study is needed to delineate appropriate time intervals for access to pediatric rheumatology care, and to identify modifiable risk factors for delay in subspecialty referral.
Acknowledgments
We thank Dr. Jaime Guzman for his comments on this report and the presentation of the results, and Dr. Sajdi Al-Mutairi and Dr. Gun Phongsamart for their help collecting data.
Footnotes
- Accepted for publication September 26, 2008.








{kind=link}
{kind=link}
{kind=link}