

Abstract
Objective. We tested the hypothesis that “fibromyalgia syndrome” is a biopsychosocial continuum disorder.
Methods. A cross-sectional survey of a representative sample of the German general population with persons ≥ 14 years of age was conducted based on face-to-face contacts. Physical distress was measured by the regional pain scale (RPS) and the Patient Health Questionnaire 15 (PHQ-15), psychological distress by the PHQ-9, and social distress by the Oslo Social Support Scale. Health-related quality of life (HRQOL) was measured by the 12-item form of the Medical Outcome Study Short Form Health Survey. A k-means clustering procedure with 2–8 clusters preset was used to classify the scores of the RPS, PHQ-9, and PHQ-15. The number of clusters retained was based on the stability and interpretability of the clusters. The cluster analysis was first performed with a randomly selected half of the sample and then cross-validated on the second half of the total sample.
Results. A 4-cluster solution produced the most stable and meaningful results. Cluster 1 was very low on all symptom scores. Cluster 2 was low on pain sites, somatic symptoms, and depression. Cluster 3 was high on pain scores, moderate on somatic symptoms, and low on depression. Cluster 4 was high on all symptom scores. The centroids of cluster 4 met the survey criteria of fibromyalgia syndrome. Cluster 4 reported a lower HRQOL and less social support compared to the other 3 groups.
Conclusion. A cluster within the continuum of biopsychosocial distress can be labeled fibromyalgia syndrome.
Only a minority of chronic pain conditions can be explained by specific structural damage1. Chronic nonspecific pain can be categorized as localized, regional, or widespread (axial pain and pain in all 4 extremities2). Chronic wide-spread pain (CWP) is a commonly reported symptom in the general population, with a point prevalence of 10%–23% in Western European countries3 and of 7%–11% in the United States and Canada4. “Fibromyalgia” (FM) has been defined by the American College of Rheumatology (ACR) as CWP and tenderness on palpation in at least 11 of 18 tender points5. Alternative criteria without tender point examination, such as the regional pain scale, have been developed6 for the clinical diagnosis of FM in clinical and survey settings.
Since the definition of FM by the ACR in 1990 there has been controversy about whether FM is a distinct clinical7 or even pathological entity8. There is consistent evidence that the symptoms and signs that make up the FM complex according to the ACR criteria, namely pain sites and tender points, are continuously distributed in community and clinical samples2,9⇓–11. The number of pain sites and tender points is associated with physical and psychological distress12,13. Therefore Wolfe argued that FM is not a distinct but a continuum disorder9, with additional psychological factors being an integral part of the syndrome14.
Studies suggest that multiple pain sites are not only associated with other physical and additional psychological symptoms, but also with social distress. Low social status in childhood as well as in adulthood was a predictor of adult regional and widespread musculoskeletal pain in a British cohort study15. In a representative sample of the general Spanish population, FM was associated with low social class16. Thus the hypothesis can be stated that FM is a syndrome at the end of a physical, psychological, and social (biopsychosocial) continuum of distress.
Clinical entities of continuously distributed biological variables (e.g., blood sugar, blood pressure) as well as psychological variables (e.g., depressed mood, pain sites) can be defined by experts’ consensus and clinical studies17. Statistical methods such as cluster or factor analyses can be used to identify symptom profiles within clinical samples18 or within the general population19. These methods were not used until now to define reproducible and clinically meaningful groups in general population samples studying the number of pain sites and associated distress.
Thus we aimed to test the hypothesis that FM is a continuum disorder. We assumed that the survey criteria of FM as well as other markers of physical and psychological distress are continuously distributed within the general population, that cluster analysis will reveal a group of persons with a symptom profile that meets the survey criteria of FM, and that this symptom profile is characterized by additional high physical and psychosocial distress.
MATERIALS AND METHODS
Design and subjects
A representative sample of the German general population was selected with the assistance of a demographic consulting company (USUMA, Berlin, Germany). The random selection was based on sampling with 3 stages, according to the typical random selection procedure in national surveys in Germany. First, 258 sample point regions were randomly drawn from the last political election register, covering rural and urban areas from all regions in Germany. The second stage was a selection of households using the random route procedure (based on a starting address). The third stage was a random selection of household respondents with the Kish selection grid. The sample was meant to be representative in terms of age, gender, and education for the general German population. The inclusion criteria for the study were age at least 14 years and the ability to read and understand the German language. All participants were informed about the study procedures and signed an informed consent form. For minors, informed consent was given by their parents. The population-based survey met the ethical guidelines of the international Code of Marketing and Social Research Practice by the International Chamber of Commerce and the European Society for Opinion and Marketing Research20. The study was reviewed and approved by the institutional ethics review board of the University of Leipzig and the German Society of Psychology.
All subjects were visited by a study assistant informed about the investigation. Self-rating questionnaires were presented. The subjects were instructed that several rating scales would follow, without informing them about the special focus of the study. The assistant waited until participants answered all questionnaires, and offered help if participants did not understand the meaning of questions.
Data collection took place between May and June 2008. A first attempt was made for 4153 addresses, of which 4064 were valid. If the subject was not at home, a maximum of 3 attempts were made to contact the selected person. The initial sample consisted of 4064 subjects, of whom 2524 (62.1%) participated fully. Reasons for dropping out included 3 unsuccessful attempts to contact the household or selected household member (7.7%), the household or selected household member declined to participate (15.8%), or the household member was on holiday (4.1%). Further, 1.2% of the participants were excluded because they were not able to follow the interview because of illness. A total of 9.0% refused to finish the interview.
Assessment instruments
Data on marital status, education status, current professional status, and family income per month were assessed using a sociodemographic questionnaire. We used a slightly modified social class index that is used in rehabilitation care and surveys in Germany. By summing the scores of the level of education (1, no graduation or graduation from primary school; 2, graduation from secondary school; 3, university entry diploma or graduation from university), the lifetime working status (1, never worked or manual laborer; 2, employee or clerk; 3, self-employed), and the actual available net family income/month (1, < 1250 Euros; 2, 1250–2500 Euros; 3, > 2500 Euros), a social class index (3, lower; 4–6, middle; > 6, upper) was calculated21.
The regional pain scale (RPS) was developed for survey research and clinical diagnosis of FM. FM is diagnosed by an RPS score ≥ 8/19 (right and left jaw, shoulder, upper arm, lower arm, hip, upper leg, and lower leg; upper back, lower back, chest, abdomen, and neck) together with a fatigue score ≥ 6 on an 11-point visual analog scale ranging from 0 to 10 (the so-called survey criteria of FM6). The concordance of ACR and survey criteria was κ = 72.3% within the setting of a rheumatological practice22. We used the German version of the RPS, which has been validated by a multicenter study (Häuser, et al, unpublished data).
The Oslo Social Support Scale (OSS-3) is a 3-item scored rating scale for the measurement of social support. The total score is calculated by summing individual item scores and ranges from 3 to 14, higher scores indicating higher social support. A total score of 3–8 is considered poor social support; 9–11, moderate; and 12–14, strong. The OSS-3 scale has been used in several studies, confirming the feasibility and predictive validity with respect to psychosocial distress23. We used a German translation of the OSS-3.
The Patient Health Questionnaire (PHQ) is a self-administered version of the Primary Care Evaluation of Mental Disorders diagnostic instrument for common mental disorders. The PHQ-15 contains 15 somatic symptoms. Each symptom is scored from 0 (not bothered at all) to 2 (bothered a lot). PHQ-15 scores of 5, 10, and 15 represent cutoff points for low, medium, and high somatic symptom severity, respectively. The PHQ-15 is therefore best characterized as a measure of somatic symptom severity rather than a diagnostic instrument for somatoform disorders. If somatic diseases are excluded, a summary score ≥ 6 indicates a somatoform syndrome. The usefulness of the PHQ-15 in screening for somatization and in monitoring somatic symptom severity in clinical practice and research has been demonstrated in numerous studies24.
The PHQ-9 is the depression module of the PHQ, which scores each of the 9 DSM-IV criteria of depression as 0 (not at all) to 3 (nearly every day). PHQ-9 scores of 0–4 indicate no depressed mood; 5–9, slightly depressed mood; 10–14, moderately depressed mood; 15–19, moderately to severely depressed mood; and 20–27, severely depressed mood. PHQ-9 scores ≥ 10 indicate a major depressive syndrome, and scores of 5–9 indicate another depressive syndrome25. Validity has been assessed against an independent structured mental health professional interview. A PHQ-9 score ≥ 10 had a sensitivity of 88% and a specificity of 88% for major depression. We used the validated German versions of the PHQ26.
The 12-item Short Form Health Survey (SF-12) is a generic measure of health-related quality of life (HRQOL). It has been developed to provide a shorter yet valid alternative to the SF-36. Physical and mental health composite scores (PCS, MCS) are computed using the scores of 12 questions and range from 0 to 100, where 0 indicates the lowest level of health measured by the scales and 100 indicates the highest. The reliability and validity of the SF-12 have been proved in numerous studies27. We used the validated German version of the SF-1227.
Statistical analyses
Cluster analysis was performed to identify symptom profiles among respondents28. A k-means clustering procedure was used. It allocates data points into a specified number of clusters based on the centroids of each data point. The k-means technique aims to group subjects so that the distance between subjects within a group is minimized and the distance between the group centers is maximized. That is, the algorithm seeks to minimize within-cluster variance and maximize variability between clusters.
The total sample was randomly divided into 2 samples. The cluster analysis was first performed on sample 1 (n = 1247) and then cross-validated on sample 2 (n = 1235). The k-means clustering procedure was conducted with 4 symptom scores as the clustering variables (order of entry into cluster analysis: RPS pain sites score, RPS fatigue score, PHQ-15, and PHQ-9 total scores) with iterations of 2, 3, 4, 5, and 6-cluster solutions. The number of clusters retained was based on the stability and clinical utility of the clusters. A solution was considered stable if the centroids (the mean scores of the clustering variables for each cluster) produced in sample 2 were within half a standard deviation (SD) of the centroids produced in sample 1. The clinical utility of the cluster analysis was tested by significance tests that compared the clusters on a set of relevant clinical variables (sex, age, social class, social support, and HRQOL). Clinical utility was assumed if the alignment of the clusters was in accord with recent classification of chronic unspecific pain2 and the results of epidemiological studies on pain sites and associated biopsychosocial distress2,11⇓–13.
Following determination of cluster groups, results of the cluster analysis were validated on sample 1 through significance tests that compared groups defined by the cluster solution on a set of relevant clinical variables29. Chi-square analysis was used for categorical variables and analysis of variance with post-hoc 2-group comparisons using Scheffe tests on continuous variables. All tests were 2-tailed, with the α-value set at 0.05. All analyses were conducted with the SPSS Version 15.0 software.
RESULTS
Sociodemographic and clinical characteristics of the study sample
The final sample consisted of 2524 persons; 52% were women. The mean age was 49 years. A total of 50.3% had 10 or more years of education. The sample was comparable to the German population in terms of sex, age, and level of education (51% women, mean age 49 years, 48% with secondary school as their highest degree30). The scores of physical and psychological distress were continuously distributed in the total sample (Figure 1).
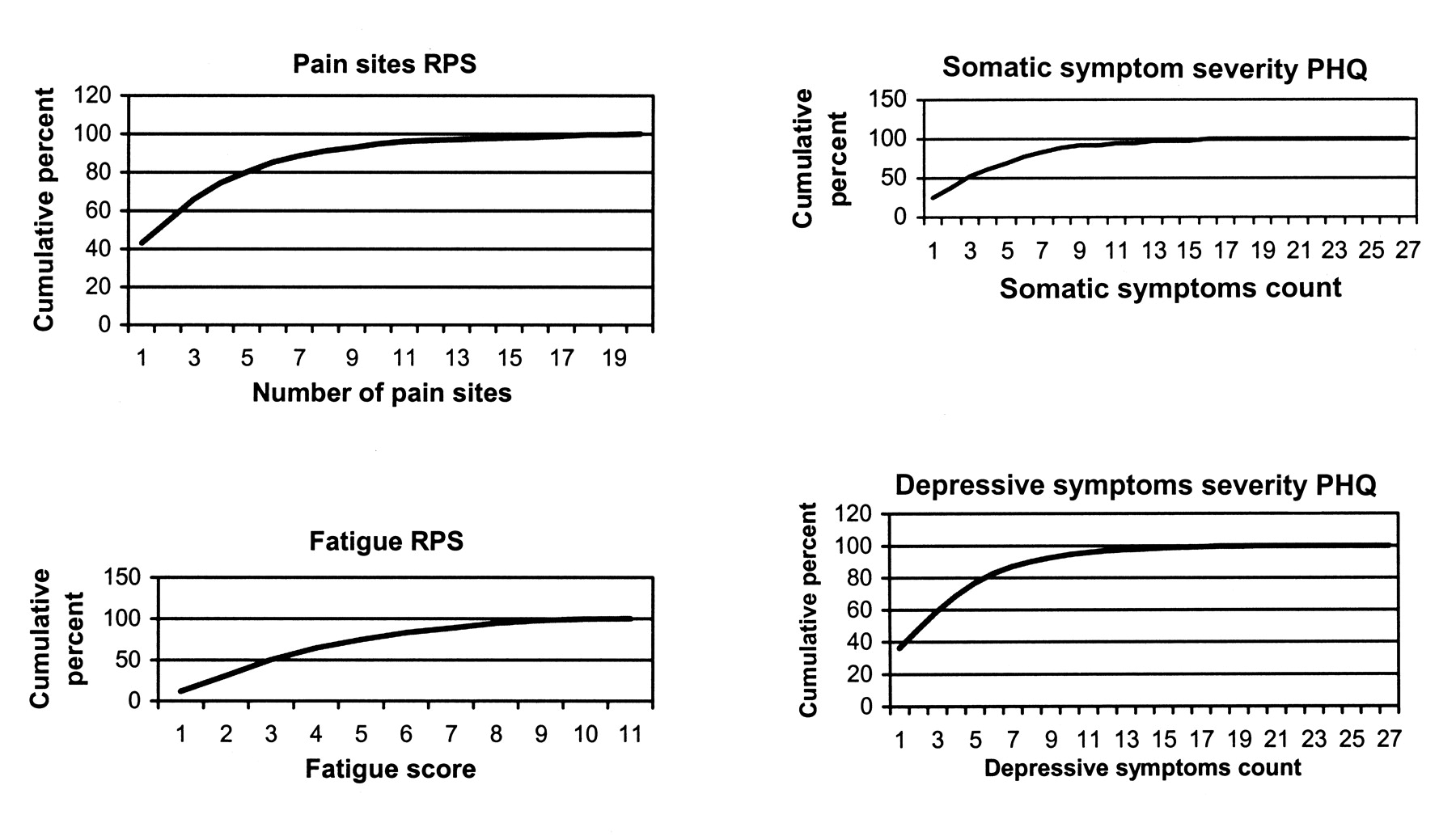
Cumulative distribution of scores of physical and psychological distress in the general population, using the regional pain scale (RPS) and the Patient Health Questionnaire (PHQ) (total study sample). RPS: regional pain scale; PHQ: Patient Health Questionnaire.
The 2 randomly selected subsamples did not differ in any sociodemographic or clinical variable (Table 1).
Demographic and clinical characteristics of the whole study sample and the 2 randomly selected halves of the sample. Some discrepancies between the number of persons in the 3 groups (first row) and the number of persons in the following rows are due to missing items.
A 4-cluster solution produced the most stable and meaningful results. The comparison of the means of the centroids indicated that the means of the centroids of sample 2 were within half the SD of the means of sample 1, with the exception of the summary score of the PHQ-9 of the two clusters 4. Yet both means were above the cutoff point of 10 that indicated a major depressive syndrome (Table 2).
Final cluster centers for symptom domains by cluster group for sample 1 (n = 1247) and sample 2 (n = 1235).
In sample 1, cluster 1 included 724 persons (58.0%) with no pain, minimal fatigue, no somatic symptom intensity, and no depressed mood [perfect health (PH)]. Cluster 2 was composed of 357 (28.6%) persons with few pain sites, moderate fatigue, low somatic symptom intensity, and borderline depressed mood [regional pain with slight physical distress (RP)]. Cluster 3 included 94 (7.5%) persons with multiple pain sites, moderate fatigue, low somatic symptom intensity, and no depressed mood. Because the number of pain sites exceeded 8, but the fatigue score was less than 6 (thus not meeting the survey criteria of FM6), this group could be labeled “widespread pain with slight physical distress (WP).” The remaining 72 (5.8%) persons formed the fourth group, with multiple pain sites, high fatigue, moderate somatic symptom intensity, and moderately depressed mood. The mean of pain sites and fatigue score of this cluster met the survey criteria of FM6.
To explore the potential clinical utility of these 4 clusters, significance tests were conducted that compared the clusters obtained in sample 1 on variables of clinical importance (Table 3). There was an overall significant difference between the 4 clusters in sex (chi-square = 11.1; p = 0.01), age (F [3,1243] = 47.7; p < 0.01), social class index (chi-square = 53.9; p < 0.001), physical (F [3,1230] = 236; p < 0.001) and mental HRQOL (F [3,1230] = 233; p < 0.001) as well as in social support (F [3,1239] = 34.4; p < 0.001). Post-hoc results indicated the FM group and the WP group were older than the PH group and the RP group. The female:male ratio in the FM group was 1.5:1, in the WP group 1.2:1, in the RP group 1.4:1, and the PH group 1:1 (all comparisons nonsignificant). The frequency of persons with low social class index was not different between the WP and FM groups (chi-square = 0.07; p = 0.80). The frequency of persons with low social class index was higher in the FM group compared to the RP group (chi-square = 7.4; p = 0.007) and the PH group (chi-square = 25.8; p < 0.001). The physical HRQOL was the lowest in the FM group, then successively higher in the WP group, RP group, and PH group (p < 0.01 for all). The mental HRQOL was the lowest for the FM group, then successively higher in the WP and RP groups and the PH group (p < 0.01 for all). The perceived social support was the lowest for the FM group, then successively higher in the WP and RP groups and the PH group (p < 0.01 for all).
Clinical characteristics by cluster group for sample 1. Some discrepancies between number of persons in the 4 groups (second row) and the number of persons in the second and third rows are due to missing items.
DISCUSSION
We aimed to test the hypothesis that FM is a clinical entity at the end of a continuum of biopsychosocial distress in a cross-sectional survey of a representative sample of the German general population. The hypothesis was confirmed. The markers of physical and psychological distress were continuously distributed among the general population. The taxonomy of chronic unspecific pain based on the number of pain sites (no pain, local pain, widespread pain) could be reproduced by cluster analysis. Two clusters with WP were identified: 1 cluster without moderate psychological distress and 1 with it. The cluster with WP and moderate psychological distress met the survey criteria of FM.
Continuum of physical and psychological distress
Our results confirm the data from population-based studies that there is a continuum of somatic and psychological symptoms in the general population: 30%–40% of the population did not report any pain at the time of the survey and 11%–17% reported local pain, and most persons with pain reported multiple pain sites2,31. Several population-based studies in different countries have demonstrated a continuous distribution of physical, anxiety, and depressive symptoms32,33.
Somatic and psychological distress in CWP and FM
Our findings are in agreement with previous studies. Not only in clinical settings but also in population-based studies, persons diagnosed with FM report higher levels of somatic and psychological symptoms, more often fulfill the criteria of mental disorders such as somatoform or depressive syndromes, and report lower HRQOL than persons with CWP not meeting the FM criteria or persons with regional pain or no pain2,13,34.
Social distress in CWP and FM
Our finding that WP and FM are more frequent in persons living in the lower social class is in line with previous findings. In a review of population-based studies, a strong inverse gradient with level of education and development of CWP and FM was reported in 5 studies. Similarly, at least the development of FM was associated with a low level of income in 2 studies, being divorced in 2 studies, living in a socially compromised housing area in 1 study, and being an assistant, nonskilled, lower-level employee or a manual laborer in 1 study4. An increased risk for FM patients to have a lower social class level was demonstrated in a population-based study of women aged 35–74 years in Germany35 as well as in Spanish and Norwegian studies16,31. For the first time we have shown that FM is also associated with less perceived social support.
Limitations
First, our findings are limited by difficulties associated with studying physical and psychological symptoms in a general population survey. Even though the response rate (62.1%) was comparable to that of other German health surveys32 and other population-based studies on CWP and FM4, 37.9% of persons addressed were nonresponders. We do not know if there were relevant differences between the survey participants and those who did not participate.
Second, the design of the study precluded an independent medical assessment.
Third, the definition of WP cases and FM cases was not identical to most previous population-based studies, which used the ACR criteria. Most importantly, the ACR criteria require a 3-month duration of pain5, while the survey criteria ask for pain in the last 7 days6. Yet the pain score of the RPS was stable over time in 9582 patients who had a paired survey observation 6 months before, with a mean RPS difference between the surveys of 0.106. Moreover, our prevalence of WP according to the RPS criteria was comparable to that of other recent studies not using the ACR criteria for the definition of WP. A Norwegian study assessed musculoskeletal pain sites in 10 different body regions by the Nordic questionnaire in 3325 adults aged 24–86 years in a community setting. A total of 4.3% of participants reported at least 6 pain sites in the last 7 days31. In a representative west European population sample with subjects > 15 years old, 10%–13% met the 4-pain criteria of the London Fibromyalgia Epidemiology Study Screening Questionnaire3.
The sex ratio of WP cases differed slightly from other recent population-based surveys. In our sample, the ratio of women to men reporting WP was 1.2:1 and in FM cases, 1.5:1. The sex ratio in CWP patients in the Swedish study was 1.6:12 and in the population-based Norwegian study, 1.8:131. The average sex ratio in a study in 5 west European countries of FM was 1.5:13. We conclude that the prevalence and sex ratio rates indicated by the RPS do not differ substantially from those assessed by other instruments.
Finally, not all persons in cluster 4 met the survey criteria of FM.
Taxonomy of chronic unspecific pain
There is uncertainty whether a cluster within a continuum of somatic and psychological symptoms that cannot be attributed to distinct pathophysiology should be considered a clinical entity or a disease17. Yet the markers of some somatic diseases of known pathophysiology, such as blood sugar in diabetes mellitus or blood pressure in arterial hypertension, are continuously distributed as well. For the purpose of taxonomy as well as of definition of clinical entities for diagnosis and therapy, the definition of cutoff points of continuously distributed variables is necessary. Considering the continuum of biopsychosocial distress, we agree with Wolfe that there is no discrete point where FM exists9. FM is not a discrete disorder that one has or does not have, such as a myocardial infarction. But this statement is also valid for diabetes mellitus or arterial hypertension. Because persons diagnosed with FM using either the ACR or survey criteria differ significantly from persons diagnosed with CWP without fulfilling the FM criteria by their levels of psychosocial distress and HRQOL, we think it is justified to consider FM as a recognizable clinical entity7,9. Because FM according to the ACR criteria is defined by symptoms and clinical findings5 and according to the survey criteria by symptoms and not by distinct organ damage6, the notion “fibromyalgia syndrome” appears to be more appropriate than the term “fibromyalgia”, suggesting a distinct disease — even though some diseases do not include distinct organ damage, e.g., migraine.
Psychological symptoms are an integral part of the fibromyalgia syndrome complex14. Assessment and therapy of WP and FM should target the whole spectrum of symptoms, not only the pain36.
Further studies are necessary to test the specificity and sensitivity of the RPS for the clinical diagnosis of fibromyalgia syndrome. Whether tender point examination is essential for the clinical diagnosis of fibromyalgia syndrome is under debate37,38.
- Accepted for publication July 23, 2009.








{kind=link}