

Abstract
Objective. To investigate whether fatigue is an inflammatory (rheumatoid arthritis; RA) variable, the contributions of RA variables to fatigue, and the levels of fatigue in RA compared with osteoarthritis (OA) and fibromyalgia (FM).
Methods. We studied 2096 RA patients, 1440 with OA, and 1073 with FM in a clinical setting, and 14,607 RA, 3173 OA, and 2487 patients with FM in survey research. We partitioned variables into inflammatory and noninflammatory factors and examined variable contribution to fatigue (0–10 visual analog scale).
Results. Factor analysis identified Disease Activity Score-28 (DAS28) and swollen (SJC) and tender joint count (TJC) as a physician-inflammation factor, and patient global assessment, pain, Health Assessment Questionnaire, and fatigue as patient components. Fatigue demonstrated weak correlations with erythrocyte sedimentation rate (ESR; r = 0.071) and SJC (r = 0.112), weak to fair correlations with TJC (r = 0.294), physician global assessment of RA activity (r = 0.384), and DAS28 (r = 0.399), but strong correlation with patient global assessment of severity (r = 0.567). In hierarchical regression analysis, patient global explained 43.1% of DAS28 fatigue variance; when SJC, TJC, and ESR were entered, the explained variance increased to 43.7%. In reverse order, SJC, TJC, and ESR explained 9.2% of the variance, but explained variance increased to 43.7% when patient global was added. The mean clinic fatigue scores were RA 4.9, OA 4.8, FM 7.6; mean survey scores were RA 4.5, OA 4.4, FM 6.3. Adjusted for age and sex, RA and OA fatigue scores were not significantly different.
Conclusion. Inflammatory components of the DAS28 contribute minimally to fatigue. RA and OA fatigue levels do not differ. Fatigue is not an inflammatory variable and has no unique association with RA or RA therapy.
Fatigue is a common symptom, although its prevalence and severity differ according to definition and setting. In a US population-based study of 56,146 adults aged 18 to 69 years, 9.4% of the population were identified as having fatigue for 1 month or longer1. In The Netherlands 22% of 12,095 working adults were fatigued according to an assessment that used a scale cutoff to determine fatigue2. Among patients within the case mix of 2 adult primary care clinics, Kroenke, et al noted fatigue that was a major problem in 24% of 1159 consecutive patients surveyed3. Bates and colleagues found that, of 995 primary care patients, 27% complained of at least 6 months of unusual fatigue that interfered with their daily lives4, and in 6 UK general practices, consisting of 31,651 persons aged 18–45 years, 18.3% reported substantial fatigue lasting 6 months or longer5.
With respect to patients with chronic illnesses in rheumatology clinics, Wolfe, et al studied 1488 consecutive patients with rheumatic diseases6. Fatigue measured by a 0–3 visual analog scale (VAS) was present in 88%–98% of patients, but clinically important levels of fatigue (> 2.0) were present in more than 41% of patients with rheumatoid arthritis (RA) or osteoarthritis (OA), and in 76% of those with fibromyalgia (FM).
Fatigue is an important symptom to patients with rheumatic diseases, where it associates with illness severity, psychological distress, and reduced quality of life, and is an important and distressing symptom in and of itself7. However, fatigue took on a special meaning in RA when the American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR) consensus panel recommended that all clinical trials should report on fatigue8. This recommendation was based on the knowledge that “patient-reported measures correlate cross-sectionally and longitudinally with measures of disease activity” and the recommendation of “working groups”9 of patients. The committee indicated that “some studies suggest that one limitation of the assessment of fatigue in clinical trials could be that fatigue is potentially secondary to other disease characteristics, and thus not an independent attribute” [of RA activity].
In addition to the importance attributed to fatigue by patient groups10 and some clinicians11, fatigue is clearly associated with treatment response in clinical trials12,13. However, all studies that have examined the direct association between inflammatory activity and fatigue have failed to find a clinically important relationship6,14,15.
With the increasing importance of fatigue in RA, we revisit fatigue and inflammation for a new perspective. We use separate settings, clinical care, and survey research, to investigate whether fatigue levels and correlates differ by setting. We compare patients with RA, OA, and FM to understand whether fatigue levels are higher in an inflammatory disorder such as RA compared with a noninflammatory disorder like OA, and we investigate the contributions of RA activity to fatigue scores using new methods and longitudinal analyses.
MATERIALS AND METHODS
We evaluated fatigue using 2 types of data: clinical practice data and survey (research) data. Clinical practice data were obtained from several sources. The multiphysician Arthritis and Rheumatology Clinic of Kansas (ARCK)16 and a solo rheumatology practice in Pennsylvania (PENN; Dr. Bergman) provided serial data on patients with RA, OA, and FM. In these clinics all patients underwent the same evaluations at every clinic visit. The clinics provided measurements of VAS fatigue (0–10)15, tender and swollen joint counts (0–28), erythrocyte sedimentation rate (ESR), VAS for patient global severity (0–10), VAS for physician global RA activity (0–10), VAS physician non-RA global severity (0–10), VAS pain (0–10), Health Assessment Questionnaire II (HAQ-II; 0–3)17, Disease Activity Score-28 (DAS28)18, and the Clinical Disease Activity Index (CDAI)19. VAS scales (0–10) asked the following questions and were anchored as follows. Fatigue: “How much of a problem has fatigue or tiredness been for you in the past week?” Fatigue anchors: “Fatigue is no problem, fatigue is a major problem.” Pain: “How much pain have you had because of your illness in the past week?” Pain anchors: “No pain, severe pain.” Patient global: “Considering all of the ways that your illness affects you, rate how you are doing on the following scale.” Patient global anchors: “Very well, very poor.” Physician’s global: “Physician’s assessment of global disease activity.” Physician’s global anchors: “None, severe.”
Data were collected in 2006 through 2008. We also used clinical practice data from the 592 patients in the Rheumatoid Arthritis Evaluation Study (RAES)20, a multiphysician, single-time observation of RA patients. RAES data collection occurred in 2004. DAS28 and tender and swollen joint data were not collected on non-RA patients. From all these data sets (ARCK + PENN + RAES) there were 1577 patients with RA with 3521 observations, 249 OA patients with 2027 observations, and 227 patients with FM with 1863 observations.
In some analyses we also included clinical practice data from the Wichita Arthritis Center (WAC). Data from these patients did not include DAS28 scores or swollen joint counts. The WAC provided data on 519 RA patients (10,205 observations), 1191 OA patients (2716 observations), and 846 FM patients (2008 observations). Data collection occurred from 1990 through 2004. Patients who were members of both ARCK and WAC were counted only once, resulting in 276 fewer RA patients in Table 1. Dual membership occurred because some WAC patients were cared for at ARCK after closure of the WAC.
Demographic and clinical characteristics of study patients. Values are expressed as mean (SD) unless otherwise indicated.
Overall, there were 1577 RA patients from ARCK, PENN, and RAES who contributed DAS and fatigue data for the analyses in Tables 2 and 3 and Figure 1. In the longitudinal analyses of Table 4 only the 2 RA clinical sites with longitudinal DAS data were studied (ARCK and PENN: N = 985). In the comparative analyses described in the text and shown in Figure 2, all RA clinical patients were used (ARCK, PENN, RAES, and WAC: N = 2096).

Factor loadings for RA variables. Arrows indicate components of DAS-28. Fatigue clusters with patient variables, not with inflammatory (physician) variables. SJC: swollen joint count; TJC: tender joint count; ESR: erythrocyte sedimentation rate; DAS28: Disease Activity Scale-28; MD global: physician global assessment of RA; Pt global: patient global severity; HAQ2: Health Assessment Questionnaire II.
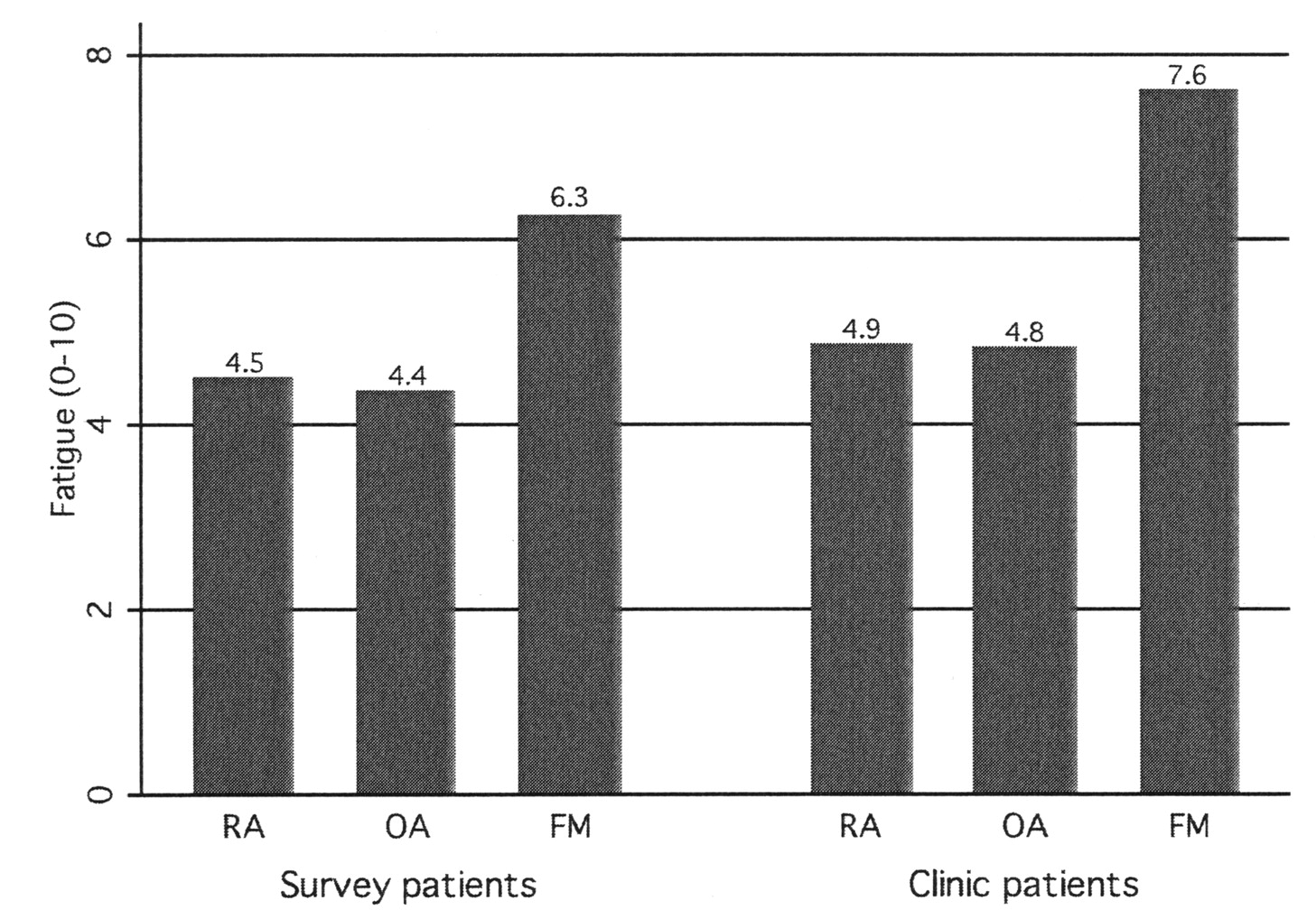
Fatigue scores in rheumatoid arthritis (RA), osteoarthritis (OA), and fibromyalgia (FM) in study sites. Differences between RA and OA patients are not statistically significant after adjustment for age and sex.
Factor analysis of clinical variables in 1577 patients with rheumatoid arthritis.
Survey data contained fatigue and patient global results, but did not have results of ESR, swollen or tender joint counts, or DAS28 scores. We used survey data to compare fatigue scores among RA, OA, and FM patients, and to measure within-patient change in fatigue over time. Survey data were provided by the National Data Bank for Rheumatic Diseases (NDB), Wichita, Kansas. NDB participants are diagnosed by US rheumatologists and are recruited from their practices. Patients are followed prospectively with semiannual, detailed, 28-page questionnaires, as described21⇓–23. Patients were enrolled continuously beginning in 1999. Rheumatic disease diagnoses were made or confirmed by the patient’s rheumatologist. Study variables were assessed at entry into the NDB and at every subsequent semiannual questionnaire. There were 14,607 RA patients (110,205 observations), 3173 with OA (27,810 observations), and 2487 with FM (17,781 observations) who contributed survey data. To avoid biasing the analyses with more severe RA, we excluded all patients who joined the NDB as part of biologic safety registries as patients in those registries were selected for severity.
Statistical methods
Analyses for Tables 1–3 and Figures 1 and 2 utilized one randomly selected observation per patient. To adjust fatigue scores by age and sex, we used least-squares regression analysis. For regression analyses that examined difference in fatigue by diagnoses, we adjusted for age and sex and clustered on the study sites described above. The relationship between fatigue and DAS and patient global was modeled using longitudinal fixed-effect (within-patient) regression and the robust Huber/White/sandwich estimator (Table 4)24. Correlation analysis used the Pearson method. Factor analysis retained 2 factors based on eigenvalues, and was followed by varimax rotation. Statistical significance was declared at the 0.05 level. Data were analyzed using Stata (Stata Corp., College Station, TX, USA) version 10.1.
RESULTS
Table 1 displays the demographic and clinical characteristics of the patient groups. Clinical RA patients include the 1577 with DAS28 data and the WAC group that did not contain DAS28 data. OA patients were older and FM patients were younger than those with RA. Otherwise, clinical values were not different from expected for these disorders.
Is fatigue an inflammatory variable?
To explore these issues we first performed factor analysis of variables commonly used in evaluating RA using the 1577-patient pooled clinical data sets that contained DAS28 data (Table 2A). A 2-factor model was identified. The first factor (Patient factor) included strong loadings for pain, patient global, fatigue, and HAQ-II. The second factor had strong loadings for swollen joint count, physician global inflammatory activity, and tender joint. Note that erythrocyte sedimentation rate (ESR) did not have associations with either factor. This analysis shows that fatigue is a component of the patient factor.
We next performed the same factor analysis, but included DAS28 in order to understand its position, and we plotted the loadings of factor 1 against factor 2 (Figure 1). This analysis shows that DAS28 and physician global have intermediate positions along the factor 1 axis, but that the patient variables are distinct from the physician-inflammation variables. ESR has weak loadings for both factors.
Correlation analysis of fatigue and DAS28 (Table 2B) indicates very weak correlations between fatigue and ESR (r = 0.071) and swollen joint count (r = 0.112), and weak to fair correlations between fatigue and tender joint count (r = 0.294), physician global (r = 0.384), and DAS28 (r = 0.399).
Correlation analysis of fatigue and DAS28 and clinical variables in 1577 patients with rheumatoid arthritis.
We next explored the relation between physician and patient DAS components in multivariable analyses in which variables are entered in blocks. Table 3 indicates that patient global explains 43.1% of fatigue variance, but when swollen joint count, tender joint count, and ESR are entered, the explained variance only increases to 43.7%. When the analysis is performed in the reverse order, swollen joint count, tender joint count, and ESR explain 9.2% of the variance, but explained variance increases to 43.7% when patient global is added. These observations indicate that physician/laboratory components of the DAS28 contribute minimally to fatigue scores.
The separate contributions of inflammatory, physician, and patient components of the Disease Activity Score-28 on the fatigue regression model in 1577 patients with rheumatoid arthritis.
Are fatigue scores more abnormal (higher) in RA compared with other rheumatic conditions?
We investigated the hypothesis that patients with RA would have more abnormal fatigue scores than those without RA (Figure 2). Among clinical patients, including data from WAC, the means (standard deviations) of fatigue scores were RA4.9 (2.9), OA 4.8 (2.9), and FM 7.6 (2.2). Among survey patients these values were RA 4.5 (3.0), OA 4.4 (2.9), and FM 6.3 (2.7). Adjusted for age and sex, among clinic patients the fatigue scores were 0.04 (95% CI 0.76 to 0.85) units greater in the 2096 patients with RA than in the 1440 patients with OA (p = 0.874). Similarly adjusted analyses in survey participants show that the mean fatigue score in 14,607 patients with RA was 0.09 (95% CI −0.03 to 0.20) units higher than in 3173 patients with OA (p = 0.132). These data indicate that, regardless of setting, there are no clinically significant differences in fatigue between patients with RA and patients with OA. Fatigue scores were substantially higher in those with FM.
What is the effect of a change in DAS28 and patient global scores on fatigue scores?
As shown in Table 4, a 1-unit increase or decrease in DAS score results in a 0.54-unit change in fatigue, while a 1-unit change in patient global (a component of the DAS) results in a 0.46-unit change in fatigue. Among patients with OA, the effect is slightly less, 0.38 units for a 1-unit change in patient global.
Fixed-effect models of Disease Activity Score-28 (DAS28) and patient global on fatigue in RA and of patient global in OA. Values are adjusted for age and sex. The robust Huber/White/sandwich estimator is used. RA models are based on data from PENN and ARCK, a mean of 3.6 observations per patient during a mean of 0.92 years. OA models are based on data from PENN, ARCK, NDB, and WAC, a mean of 7.7 observations per patient over a mean of 4.0 years.
DISCUSSION
Despite the recommendation of the ACR-EULAR committee8 and patient support groups9, no study has shown an independent association between RA inflammatory activity and fatigue. In our current report we show, in a clinical sample of 1577 patients with RA, that the correlation between fatigue and swollen joint count is 0.112, and between fatigue and ESR is 0.071 – essentially no correlation at all (Table 2). We also found that the correlation with the DAS28 was 0.399, but almost all of that correlation was explained by patient global (Table 3). In fact, in hierarchical models, swollen and tender joint count and ESR explained 9.2% of fatigue variance. Adding patient global to that result increased the explained variance to 43.7%. Further, the level of fatigue did not differ between RA and OA patients in either the clinical or research setting (Figure 2). If it is inflammation that drives fatigue, we would expect that fatigue scores would be higher in RA compared with OA.
Wolfe, et al showed in 1996 in 628 clinic RA patients that fatigue was poorly correlated with ESR (r = 0.074) and tender joint count (0.079), and that RA and OA patients did not differ in fatigue levels6. In 1998, Huyser, et al studied 77 RA patients in a US Veterans Administration hospital outpatient setting25. They found a correlation between fatigue and tender joint count of 0.09 and with ESR of 0.02. Pollard and colleagues addressed fatigue in 2 cohorts of 238 and 274 RA patients14. They concluded that pain, not inflammation, explained fatigue, in agreement with earlier studies6,15. In addition, they found correlations between fatigue and DAS28 to be 0.48 and 0.47 in the overall cohorts, and at levels of 0.69 and 0.43 in subsampled treatment studies of the 2 cohorts. In our clinical study the association of fatigue and DAS28 was r = 0.399, similar to their clinical studies.
Our current study adds additional important information to the fatigue-RA activity issue by examining individual components of RA activity as measured by the DAS28. In agreement with Pollard, et al14 we found a moderate association between DAS28 and fatigue. However, we found that 79% of the explainable variance was attributable to patient global, and not to swollen joints, tender joints, and ESR. Further information regarding the weak association between RA and inflammation comes from our data that demonstrated that RA and OA patients in the clinical and in research settings had similar levels of fatigue.
The failure to demonstrate an association between fatigue and RA activity is not to downplay the importance of fatigue in RA or, for that matter, in any illness situation. In addition, a 1-unit change in the DAS score was associated with a 0.54-unit (95% CI 0.45, 0.63) change in fatigue levels. Fatigue is a very distressing symptom, and persons with substantial levels of fatigue have impairment in quality of life, however assessed. The authors use VAS to assess fatigue in every patient they see, and find that measurement of fatigue adds substantially to clinical understanding and clinical care. Our study and the RA fatigue literature call into question the usefulness of fatigue in clinical trials of medical therapy and of its association with RA activity. Even so, we recommend the use of fatigue scales in clinical practice to assess all patients, regardless of diagnosis, because fatigue occurs as frequently in other rheumatic diseases as in RA.
There are currently many accepted tools to measure fatigue15,26⇓⇓–29, including the Medical Outcome Study Short-Form 36 vitality scale and the VAS scale that we used. And, in general, they yield similar results15. We recommend the VAS because it is simple to use and score in clinical settings where other scales are already being used.
In our study we addressed fatigue and its relation to inflammation in RA and to levels of fatigue in inflammatory and noninflammatory disorders, but we did not explore other factors that might contribute to, or be correlated with, fatigue, such as anxiety, depression, sleep problems, learned helplessness, social support, comorbidity, illness severity, and psychosocial and demographic characteristics6,30⇓⇓–33. While we found that RA and OA had similar levels of fatigue, the predictors of fatigue, including psychosocial factors, may differ in their contribution and importance over the spectrum of rheumatic illnesses. These contributors are worthy of further investigation. In many of the analyses described above we used patient global rather than patient pain as a predictor of fatigue since patient global is a component of the DAS28. However, pain is more correlated with fatigue than global, and we recommend its use in clinical care.
The association between fatigue and RA inflammation is weak. Although the DAS-fatigue association appears stronger, it is largely the result of the relation between a DAS component, patient global, and fatigue. Adding to the noninflammatory associations is our observation that fatigue levels in RA and OA do not differ.
- Accepted for publication July 16, 2009.








{kind=link}
{kind=link}