

Abstract
Objective. To describe cases of development of pulmonary nodulosis or aseptic granulomatous lung disease in patients with rheumatoid arthritis (RA) receiving anti-tumor necrosis factor-α (TNF-α) therapy.
Methods. A call for observation of such cases was sent to members of the French “Club Rhumatismes et Inflammation.” The cases had to occur after introduction of TNF-α-blocking therapy.
Results. Eleven cases were examined: 6 patients were treated with etanercept, 2 with infliximab, and 3 with adalimumab. Pulmonary nodular lesions were observed after a mean treatment period of 23.3 ± 15.3 months. Clinical symptoms were observed in 5 cases. Radiographs or computed tomography of the chest showed single or multiple nodular lesions in 10 cases and hilar adenopathies in 1 case. Biopsy of the nodular chest lesions or mediastinal lymphadenopathies were performed in 8 patients, and revealed typical rheumatoid nodules in 4 cases and noncaseating granulomatous lesions in 4 cases. Mycobacterial or opportunistic infections were excluded for all cases. Outcome was favorable for all the patients, with either discontinuation or maintenance of anti-TNF-α treatment.
Conclusion. Aseptic pulmonary nodular inflammation corresponding to rheumatoid nodules or noncaseating granulomatous inflammation can occur during anti-TNF-α therapy for RA, mainly etanercept. The mechanism explaining such a reaction is not clear but certainly includes different processes. These cases of pulmonary nodular inflammation generally have a benign course and do not systematically require withdrawal of treatment.
Rheumatoid nodules occur in approximately 25% of patients with rheumatoid arthritis (RA) and are mainly located subcutaneously at pressure points such as elbows or hands. They may also be observed in internal tissues and can compromise organ function leading to clinical symptoms. The liver, eyes, heart, and lungs may be affected by such nodules.
Tumor necrosis factor-α (TNF-α) antagonists are now widely used for treating RA. Various side effects have been described with the different TNF-α antagonists available, mainly infections. The efficacy of these agents for treatment of extraarticular features of RA such as rheumatoid nodules has not been specifically evaluated in large placebo-controlled randomized trials. However, it has been reported that etanercept has no influence on subcutaneous nodules in RA1. Conversely, there are some reports of accelerated cutaneous nodulosis2 and descriptions of development of histologically proved pulmonary rheumatoid nodules or granulomatous inflammation in patients receiving anti-TNF-α therapy3,4.
We report the largest series of patients with RA under treatment with TNF-α antagonist developing pulmonary nodular lesions that corresponded to rheumatoid nodules or aseptic noncaseating granulomatous inflammation.
MATERIALS AND METHODS
Between 2005 and 2008, all members of the Club Rhumatismes et Inflammation (a section of the French Society of Rheumatology including 866 rheumatologists and internal medicine practitioners) were contacted by e-mail to collect reports of patients with RA who presented with pulmonary nodules during anti-TNF-α therapy. To be enrolled in this case study analysis, the pulmonary nodules had to occur after the introduction of TNF-α-blocking agent and had to correspond to rheumatoid nodules that were proved histologically. A rheumatoid nodule was defined as a central necrotic fibrinoid tissue, surrounded by a palisaded layer of mononuclear cells and a peripheral vascular zone with chronic inflammation5. Alternatively, pulmonary nodules may also correspond to aseptic and noncaseating granulomatous inflammation that relates to a chronic organized inflammatory lesion defined by the presence of macrophages (some of which may be giant multinuclear or epithelioid cells) surrounded by a lymphoid infiltrate and fibrosis. This granuloma may be well formed or alternatively poorly organized, and may be centered on a noncaseating necrotic zone6. The patients also had to have a normal chest radiograph before the anti-TNF-α treatment. Patients who had preexisting nodular lung lesions prior to the anti-TNF-α treatment and who developed new pulmonary nodules were also included. Other causes of pulmonary nodules had to be excluded, especially opportunistic and mycobacterial infections and malignant neoplastic diseases. These conditions were excluded using specific bacteriological procedures and histological analysis.
RESULTS
Patient demographics
Eleven patients were reported, 8 men and 3 women, with a mean age of 56.3 ± 10.8 years and mean disease duration of 9.2 ± 7.1 years. Subcutaneous rheumatoid nodules were present in 3 cases before starting the anti-TNF-α agent. Two patients had preexisting lung pulmonary lesions prior to the anti-TNF-α treatment that were diagnosed as rheumatoid nodules. Other extraarticular findings were vasculitis in one patient and pulmonary fibrosis in another. Five patients had leflunomide and 3 had methotrexate as associated therapy to the TNF-α blocker. They all had corticosteroids at a mean dosage of 5.7 ± 4.6 mg prednisolone. Six patients received etanercept, 2 had infliximab, and 3 adalimumab. Before starting anti-TNF-α treatment, each patient was screened for tuberculosis and underwent a chest radiograph, a clinical pulmonary examination, and a PPD test according to French agency recommendations. The mean delay between onset of anti-TNF-α and development of lung nodular lesions was 23.3 ± 15.3 months (Table 1).
Case series of pulmonary nodulosis and hilar adenopathies occurring in patients with rheumatoid arthritis under anti-TNF-α treatment.
Clinical symptoms and biological findings
Asthenia, cough, dyspnea, or chest pain was reported by 5 patients, while the others were asymptomatic. Patients had active disease as shown by a mean Disease Activity Score (DAS28) of 3.5 ± 1.3 and increased values of erythrocyte sedimentation rate (23.5 ± 20.7 mm/h) and C-reactive protein (31.2 ± 37.9 mg/l). Rheumatoid factors were positive in 10 cases and anti-cyclic citrullinated peptide antibodies in 7 patients. Sputum cultures were performed for all patients and were negative for mycobacteria and fungi. No patient reported new onset of subcutaneous nodules. Ten patients responded to the anti-TNF-α treatment with a significant improvement of the DAS28 score.
Radiological and computed tomography findings
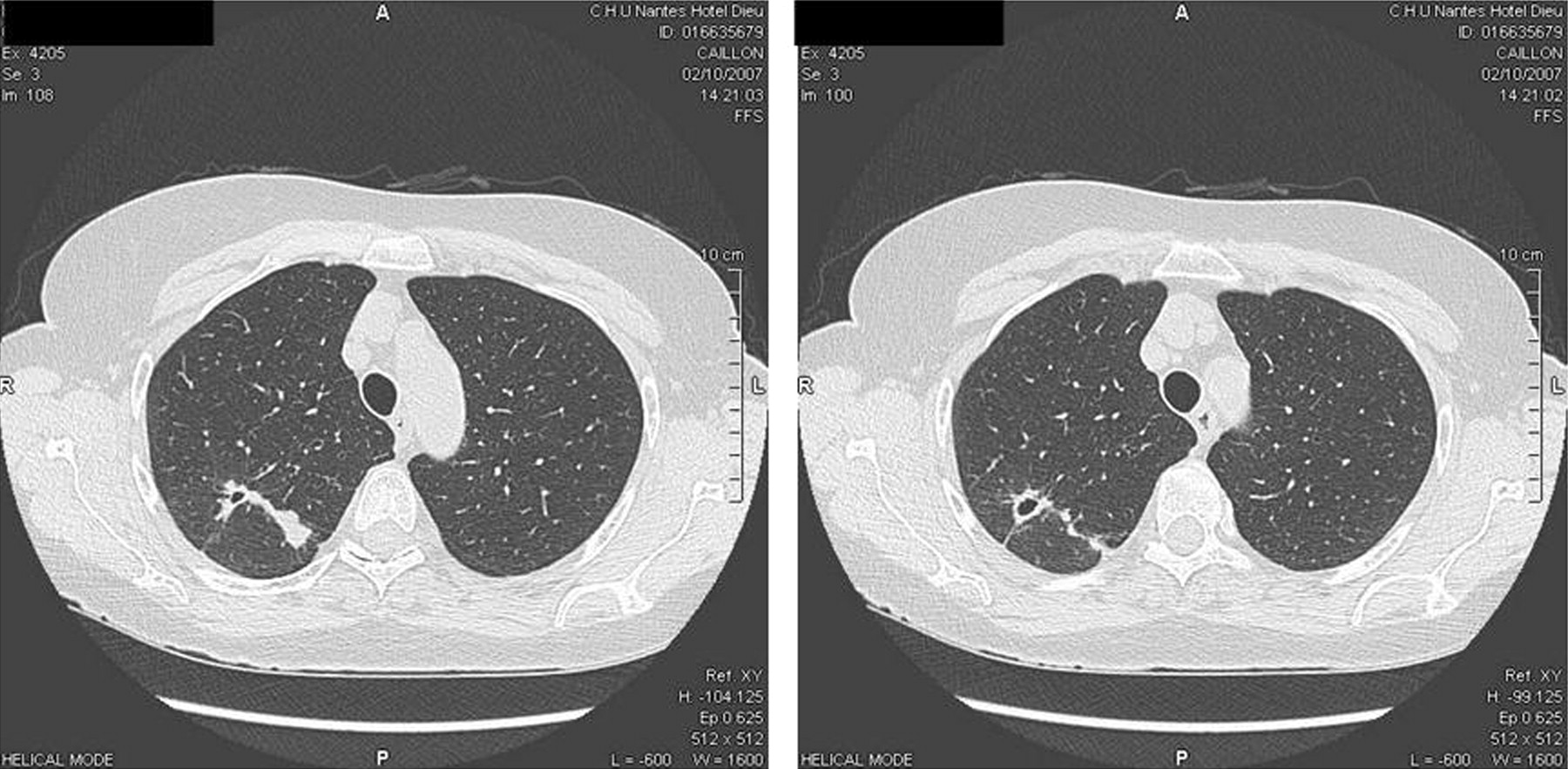
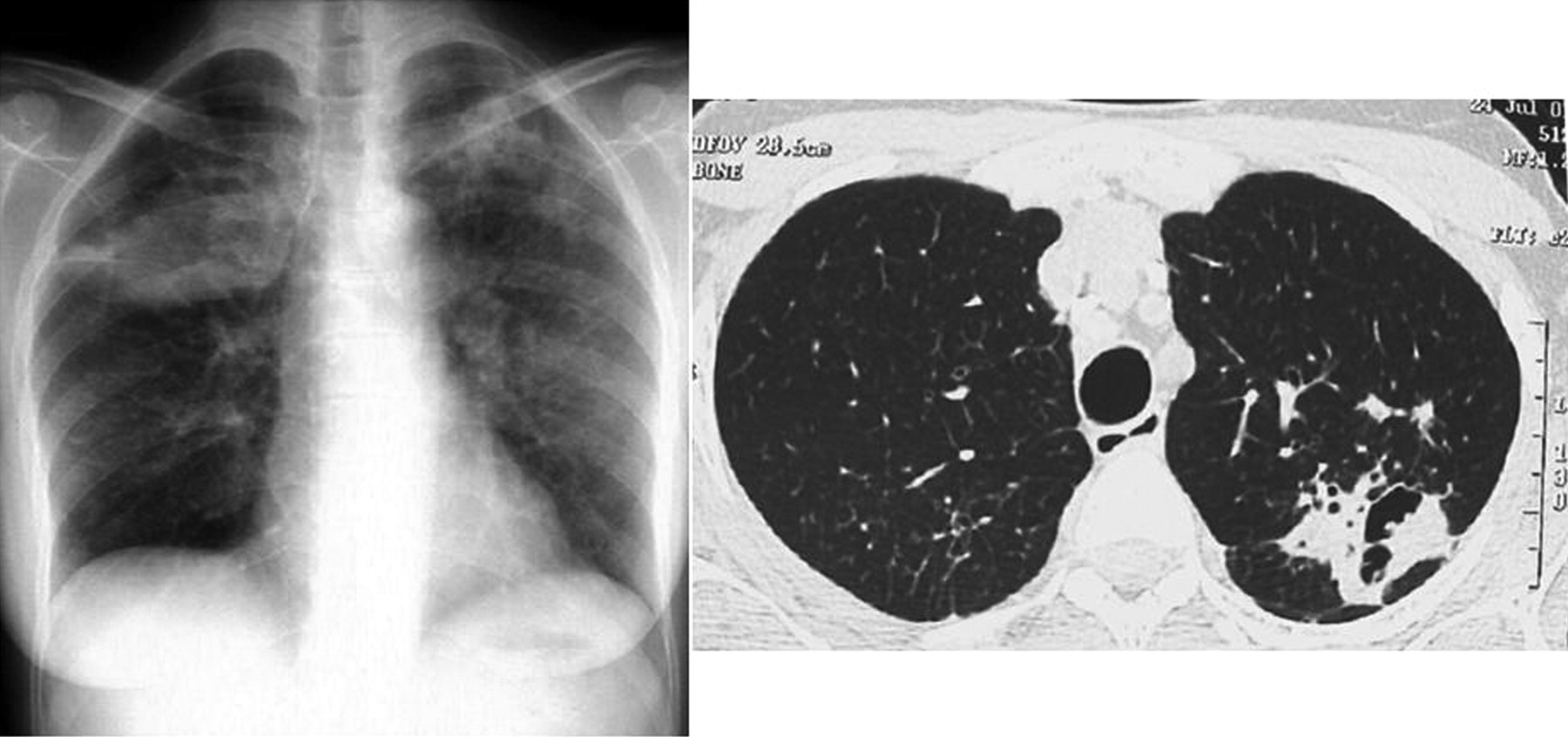
Single or multiple nodules were found in 10 cases and hilar adenopathies in one case. Cavitated lesions were observed in 2 cases (Cases 2 and 10 in Table 1). They were found in 2 male patients: the first was under adalimumab treatment and the second etanercept. Both were asymptomatic. Extensive studies for microbial organisms (mycobacteria and opportunistic infections) were all negative (including cultures from bronchoscopy and bronchoalveolar lavage specimens for Case 2 and nodular lung biopsy examination for Case 10 with tissue stains for acid-fast bacillus and fungi, as well as microscopic examination of stained specimens). One patient had conflating nodular lesions (Case 6 in Table 1). Nodular lesions were observed both at the bases and at the apical regions of the lungs. Subpleural nodules were also observed (Figures 1, 2, 3).
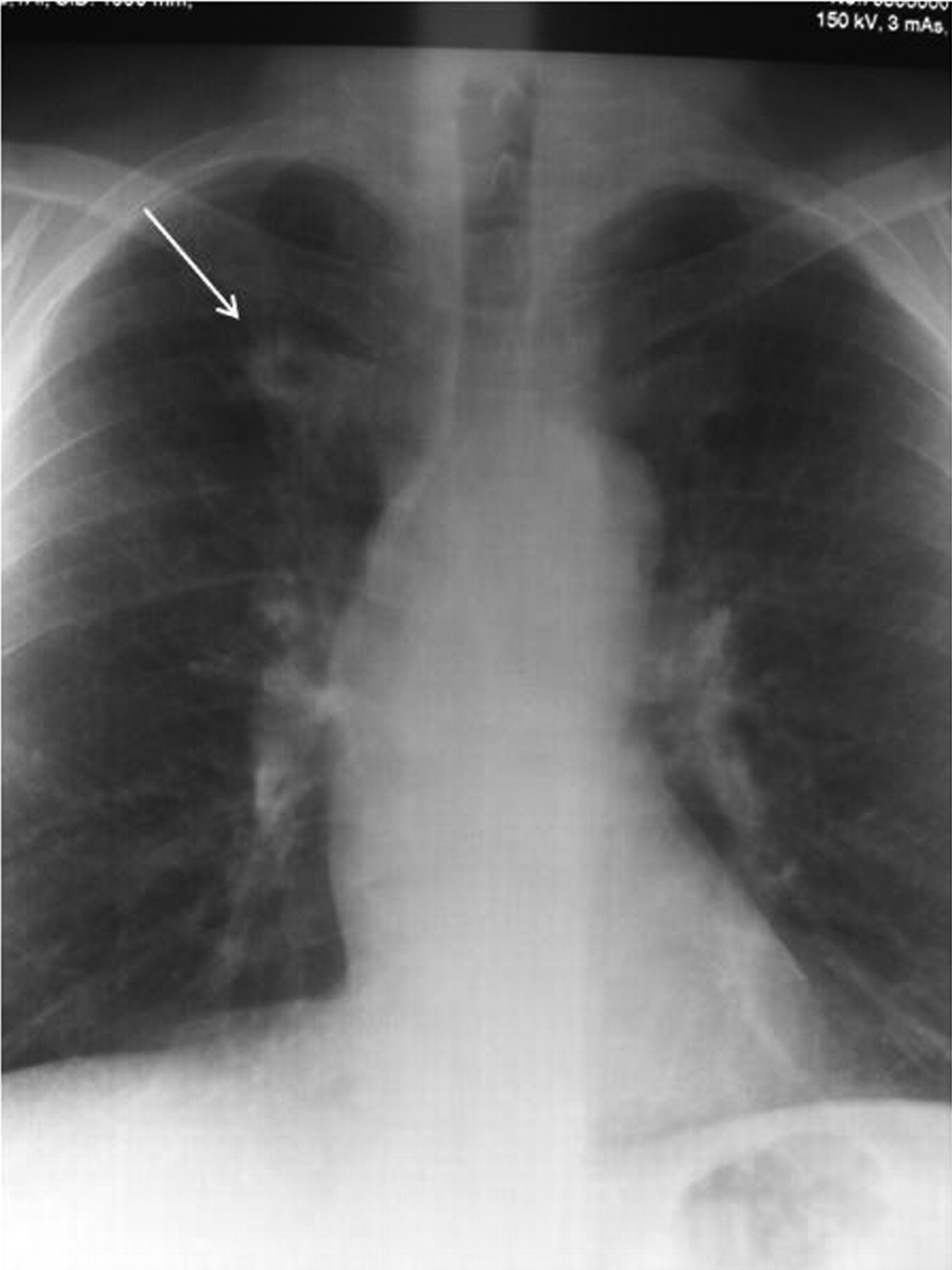
Chest radiograph showing cavitated nodular lesion in the apical part of the right lung (arrow).

Computed tomography of the chest showing a pulmonary nodule in the right lung with cavitation.

Chest radiograph and computed tomography showing disseminated bilateral and merging nodules.
Histological examination
An open lung biopsy of the nodules was performed in 7 cases and hilar adenopathies were also biopsied for the patient without a nodular lesion. A biopsy was not performed for the 3 other patients for various reasons (one patient had hemophilia, another had preexisting lung rheumatoid nodules and a systematic new chest radiograph showed the development of new multiple nodular lesions; after a followup of more than 2 years, outcome for the third patient was favorable with discontinuation of anti-TNF-α therapy; in addition, the pneumologist considered that the nodular chest lesion was very suggestive of a rheumatoid nodule). Characteristic rheumatoid nodule was found in 4 cases, one patient had a chronic and granulomatous inflammatory lesion, 2 others had a granulomatous lesion with central fibrinoid necrosis, and the last corresponded to lymphadenopathy, which showed noncaseating granuloma formation with silica particles. Cultures of biopsy specimens for all these patients were negative for opportunistic infectious agents including mycobacteria and fungi. In addition, angiotensin-converting enzyme levels were normal.
Patient outcomes
Anti-TNF-α treatment was discontinued in 6 cases and was maintained for the others. In most cases, including those who continued anti-TNF-α treatment and after a mean monitoring period of 2 years, there was no evidence of progression of the lung nodules; in one case (Case 2, who did not undergo a biopsy), the nodule resolved spontaneously. For one patient (Case 11), anti-TNF-α treatment was reintroduced after a 6-month withdrawal period, and again, new nodular lung lesions were observed. Finally, 2 patients who discontinued the TNF-α-blocking agent received rituximab, with resolution of the nodules.
DISCUSSION
Rheumatoid nodules are considered the most characteristic extraarticular feature of RA. Predisposing factors for development of rheumatoid nodules in RA have been identified as genetic factors (HLA-DRB1*04), smoking, severe articular disease, and positivity for rheumatoid factors. Pathogenic mechanisms leading to the development of rheumatoid nodules are not well understood, but it is thought that local trauma, vasculitis, proteolytic enzymes, and immune complexes play a role. Vascular events probably initiate the nodule formation, followed by immune complex activation of local monocytes and macrophages and then by the release of cytokines and proteinases by activated macrophages, resulting in the palisaded arrangement of cells5. Some similarities between the rheumatoid nodule and the rheumatoid synovium have been emphasized; indeed, they both included activated macrophages and a process of new vessel formation3. However, compared to inflamed synovium, the anatomical organization of the rheumatoid nodule has some differences3: there is no lymphoid organization, no B cells or plasma cells, no major cellular infiltration by T cells, and interleukin 1 concentrations are higher in rheumatoid nodules, while TNF-α concentrations are lower7.
We describe here 11 cases corresponding to the development of nodular lung lesions in 8 cases, the appearance of new nodular lesions in 2 cases, and the development of hilar adenopathies with granulomatous reaction in another case. The nodular lung lesions corresponded to typical histologically proved rheumatoid nodules in 4 cases and aseptic and noncaseating granulomatous lung inflammation in 3 cases. These cases were mainly observed with etanercept (6/11) and occurred in patients receiving associated disease-modifying antirheumatic drugs (DMARD) such as methotrexate or leflunomide in 8 cases. However, we did not observe cutaneous nodulosis in this series. With the discontinuation of the TNF-α-blocking agent, all the patients had a favorable outcome, with stability or even resolution of the nodular lesion. Interestingly, 4 patients continued their treatment (including etanercept in 2 cases) without progression of the nodular lesion. Conversely, in one patient, the reintroduction of the TNF-α-blocking agent again induced the development of nodular lung lesions.
Uncommon cases of cutaneous nodulosis have been reported under treatment with the 3 anti-TNF-α agents2,3,8 (Table 2). There are also a limited number of reports of pulmonary nodulosis in patients with RA receiving anti-TNF-α therapy: 5 cases were identified in the literature search3,9–12. All these patients were treated with etanercept with a treatment duration ranging from 2 months to 2 years. In 3 cases, patients with RA had subcutaneous nodules before the administration of etanercept3,10,11. Clinical symptoms for pulmonary nodulosis were cough or dyspnea in 2 cases. All the nodular lesions were biopsied, revealing characteristic rheumatoid nodules. These nodular lung lesions were resolved with discontinuation of etanercept. In one case, etanercept was maintained, and there was no evidence of progression of the lung nodules12. In common with the 4 cases from our series, pulmonary granulomatous inflammation or sarcoid-like granulomatous disease located in the lungs was reported in 10 patients with RA under etanercept treatment4,13–15. A biopsy of the nodular lesions showed well formed or less organized aseptic and noncaseating granulomatous inflammation with negative cultures for mycobacteria or fungi. All these patients had a favorable outcome after cessation of the drug, and no recurrence of the pulmonary disease was observed with the introduction of adalimumab in 4 cases4.
Cases of subcutaneous and pulmonary nodulosis in patients receiving anti-TNF-α agents.
An unexpected finding in one patient in our series was silica particles within the noncaseating granulomatous reaction. This patient had mediastinal lymphadenopathies without lung involvement. He was not known to have silica exposure. The relationship between silica exposure and the development of autoimmune disease such as RA has been reported, and pathological findings of silica-infiltrated lymph nodes correspond to granuloma-like structures16. Microscopic crystalline particulates have been identified from lung biopsy specimens in a patient with RA who had diffuse reticulonodular infiltrate while receiving etanercept13. In this case, transbronchial lung biopsy showed noncaseating granuloma, and it is thought that these particulates may favor inflammatory reaction. The addition of anti-TNF-α treatment in this situation may interfere with this reaction, and one may hypothesize that blocking TNF-α may be a predisposing factor for the development of this granulomatous reaction (resulting in pulmonary infiltrate or adenopathies).
The mechanisms that may explain nodular lung lesions under anti-TNF-α are unclear. Pulmonary rheumatoid nodules were mainly observed with etanercept, but not exclusively (5 cases per 5 in the literature but only one case per 4 in our series). It is known that rheumatoid nodules are characterized by low levels of apoptosis, and etanercept does not induce apoptosis compared to the anti-TNF-α monoclonal antibodies. Thus, the different immunological properties of etanercept may account in part for the differences in incidence of pulmonary nodulosis17. Alternatively, vasculitis is involved in rheumatoid nodule formation and anti-TNF-α agents may paradoxically induce vasculitis18,19. Anti-TNF-α agents reduce cell trafficking to inflamed joints, and it has been suggested that they may favor the cellular infiltration of other inflamed tissue such as rheumatoid nodules3. TNF-α concentrations are lower in the supernatants of rheumatoid nodule cultures and the administration of TNF-α-blocking agents may have fewer effects on rheumatoid nodules compared to the inflamed synovium.
Interestingly, cases of pulmonary sarcoidosis were described in patients receiving anti-TNF-α agents20. The cases of pulmonary aseptic and noncaseating granulomatous inflammation described previously had features similar to sarcoidosis and were exclusively observed during etanercept therapy (10 cases per 10 in the literature and 4 in 4 in our series). The mechanisms that have been proposed to explain such reactions (sarcoidosis and sarcoidosis-like diseases) resemble those leading to rheumatoid nodules, i.e., distinctive immunological properties and differing modes of action of etanercept and the anti-TNF-α monoclonal antibodies (including binding avidity, clearance, binding to membrane TNF-α, and binding to lymphotoxin-α)4,13,14,15,20. In addition, variation in cytokine concentrations during anti-TNF-α treatment may also play a role: indeed, anti-TNF-α monoclonal antibodies inhibit interferon-γ (IFN-γ) expression, in contrast to etanercept, and IFN-γ contributes to granuloma formation17. TNF-α inhibits transforming growth factor-ß, which is known to downregulate granuloma formation in conditions such as sarcoidosis21. Of interest, the pulmonary nodular lesions in our series occurred while patients were improved by the anti-TNF-α treatment, suggesting a different mechanism of action for the 2 manifestations.
Accelerated cutaneous or pulmonary nodulosis is a well recognized complication of methotrexate and leflunomide11. In our series, 8 patients had leflunomide (n = 5) or methotrexate (n = 3) as associated therapy. However, these DMARD had been taken for many years, and it was thus unlikely that they could be related to the lung injury.
Pulmonary nodulosis and aseptic granulomatous lung disease are rare during anti-TNF-α therapy. The exact incidence of this side effect is difficult to estimate but is probably around 0.042%, since 26,000 patients are currently receiving TNF-α-blocking agents in France (11 cases/26,000). However, our study has limitations deriving from the observational design and some cases would certainly have been missed, or not declared, or alternatively not diagnosed in the case of asymptomatic patients.
We conclude that aseptic and inflammatory pulmonary nodules may appear in patients receiving anti-TNF-α agents, and that they correspond to rheumatoid nodules or granulomatous inflammation. These lesions are mainly observed during etanercept therapy, particularly in cases of granulomatous inflammatory disease. The mechanism explaining such a reaction is not clear, but certainly includes several different processes. These cases of inflammatory pulmonary nodules generally have a benign course and do not systematically require withdrawal of treatment. Since the differential diagnosis of such pulmonary lesions includes a large spectrum of diseases, mainly infections and malignancies, it is essential for clinicians to be aware that a pulmonary rheumatoid or granulomatous inflammatory nodule may develop during anti-TNF-α therapy.
Acknowledgments
The authors are indebted to Frances Sheppard (CIC-Biotherapy 506, Besançon, France) for help in preparing the manuscript.
Footnotes
- Accepted for publication June 27, 2009.








{kind=link}
{kind=link}
{kind=link}