

Abstract
Objective. To examine the effect of anti-tumor necrosis factor-α (anti-TNF) therapy in patients with reactive AA amyloidosis associated with rheumatoid arthritis (RA).
Methods. Fourteen patients with reactive AA amyloidosis associated with RA were prospectively evaluated. Four patients were treated with infliximab and 10 with etanercept. The mean period of anti-TNF therapy was 20.1 ± 13.8 months. Laboratory findings and renal function were examined before and after initiation of anti-TNF therapy. In 9 patients the area of amyloid deposits in serial gastroduodenal mucosal biopsy specimens was examined and image analysis was performed.
Results. C-reactive protein and serum amyloid A protein levels were significantly reduced after initiation of anti-TNF therapy. Twenty-four hour creatinine clearance improved in 4 patients, did not change in 5, and deteriorated in 3. Twenty-four hour urinary protein excretion was significantly decreased in 3 patients, not exacerbated in 6, and increased in 3 after initiation of anti-TNF therapy. The biopsy specimens from the 9 patients who underwent serial gastroduodenal biopsies showed significant decreases in the area of amyloid deposits, from 8.8% ± 6.4% to 1.6% ± 0.6% (p = 0.003) after initiation of anti-TNF therapy. Four patients showed a sustained decrease in the areas of amyloid deposits in their third biopsy specimens, and amyloid deposits were not detectable in 2.
Conclusion. Our results indicate a striking effect of anti-TNF therapy for rapid removal and sustained disappearance of amyloid deposits in gastric mucosal tissue with amelioration of renal functions in patients with reactive amyloidosis due to RA.
Recently it has become apparent that rheumatoid arthritis (RA) is not only an inflammatory disease affecting multiple joints but also a cause of systemic organ dysfunction in relation to persistent systemic inflammation; this dysfunction may increase the risk of organ failure and death in affected patients1–4. Reactive amyloid A (AA) amyloidosis is a serious and life-threatening systemic complication of RA that arises from chronic, systemic, long-lasting inflammation, with elevated levels of serum AA (SAA) protein5–7. SAA is an acute-phase 12.5-kDa apolipoprotein associated with high-density lipoprotein, and is the circulating precursor of amyloid A protein. Amyloid A fibrils are insoluble and can be deposited in systemic organs, including the kidneys, heart, or gastrointestinal (GI) tract, owing to the overproduction of SAA under such inflammatory conditions6–8.
The prevalence of reactive AA amyloidosis in patients with RA is still unclear, but is no longer considered rare. The frequency of AA amyloidosis associated with RA ranges from 7% to 26%9–13, although the prevalence of clinically symptomatic amyloidosis is reportedly lower14,15. Common clinical signs of reactive AA amyloidosis in patients with RA can be found by careful observation for the onset of proteinuria, kidney insufficiency, or GI tract symptoms, but amyloid deposition itself can be present before clinical signs of AA amyloidosis appear. This subclinical phase might explain the wide variation of disease prevalence.
Several studies have reported the beneficial effects of combination therapy with corticosteroid and cytotoxic reagents for AA amyloidosis with RA16–19, but this condition is often unresponsive to these therapies once organ dysfunctions have become apparent and progressive, leading to endstage renal disease, severe infection, or intractable diarrhea with high mortality rates20–24.
Recent studies have indicated the therapeutic potential of anti-tumor necrosis factor-α (anti-TNF) or anti-interleukin 6 (anti-IL-6) agents for AA amyloidosis secondary to inflammatory arthritides, including RA25–30, but the significance of any improvement in tissue levels has not been fully evaluated.
Our purpose was to prospectively examine the safety and efficacy of anti-TNF therapy in RA patients with reactive AA amyloidosis by following their clinical disease activity and laboratory findings, including renal function, as well as evaluating the changes in amyloid deposition in serial GI mucosal biopsy tissues.
MATERIALS AND METHODS
Patients
Fourteen patients with an established diagnosis of reactive AA amyloidosis participated in the study between December 2004 and July 2007. Each patient satisfied the 1987 American Rheumatism Association criteria for RA31. The study protocol was approved by the Institutional Review Board of Niigata University Hospital, and the subjects gave informed consent to participate.
All patients were treated with the anti-TNF reagent infliximab or etanercept as follows: after informed consent had been obtained, infliximab was assigned to 4 patients with normal renal function and who were receiving methotrexate; etanercept was assigned to 1 patient with the same conditions; etanercept was also assigned to 1 patient with normal renal function and interstitial pneumonia, and to 8 patients with renal insufficiency (24-h creatinine clearance < 50 ml/min).
Diagnosis of reactive AA amyloidosis
All patients had undergone renal, rectal, GI tract, or abdominal fat biopsies and had been confirmed to have reactive AA amyloidosis before they entered the study. Congo-red staining of tissue specimens was performed for histopathological diagnosis, and green birefringence was considered indicative of the presence of amyloid deposits. These deposits were confirmed as AA-type amyloid using 2 techniques: disappearance of Congo-red-positive staining after incubation with potassium permanganate, and immunohistochemical analysis using anti-amyloid A antibody and anti-immunoglobulin light-chain (AL) antibody to exclude AL amyloidosis.
Treatment
Patients were treated with either etanercept (n = 10) or infliximab (n = 4). Etanercept, a recombinant form of the human 75-kDa TNF receptor fusion protein, was injected subcutaneously (25 mg twice a week). Infliximab, a humanized monoclonal anti-TNF antibody, was infused (3 mg/kg) at weeks 0, 2, and 6, and then every 8 weeks.
Assessment
Tolerance to, and adverse events during, anti-TNF therapy were recorded for every patient. Laboratory and clinical evaluation of disease activity included repeated determinations of creatininemia (Cr), 24-h proteinuria, 24-h creatinine clearance rate (Ccr), SAA protein, and C-reactive protein (CRP). Efficacy was defined as a sustained decrease in 24-h proteinuria and a stable or improved Ccr. Disease activity was assessed by Disease Activity Score, including a 28-joint count (DAS28(3)-CRP) calculated in accordance with an authorized formula (http://www.das-score.nl/). Serial gastroduodenal mucosal biopsies were performed in subjects who had undergone anti-TNF therapy for at least 1 year for comparison before and after anti-TNF therapy.
Image analysis of amyloid-positive areas
Gastroduodenal mucosal biopsies were performed before and after the initiation of anti-TNF therapy to evaluate the percentage changes in the amyloid-positive areas.
A total of 4 specimens (3 from the lesser curvature of the gastric antrum and 1 from the bulbus of the duodenum) were taken in each biopsy and fixed in 10% formalin, embedded in paraffin, and cut into sections 5 μm thick. Sections were considered suitable for quantitative analysis if they consisted of the full thickness of the mucosa with vascular components, and were cut perpendicular to the surface.
The amyloid-positive area in the gastroduodenal mucosa was determined on the Congo-red-stained sections. One section of whole gastroduodenal mucosal tissue was photographed. The borders of the amyloid-positive areas in each gastroduodenal mucosal specimen were traced in each photograph, excluding the tissue-free spaces. The total amyloid-positive area was measured with ImageJ v. 3.91 software (http://rsb.info.nih.gov/ij), and the percentage area of amyloid per whole-tissue section was calculated. All selected slides were evaluated for total amyloid-positive area, and the highest percentage for amyloid deposition in each biopsy sample was selected for analysis.
Statistical analysis
Differences between samples were analyzed by paired Student's t test at a significance level of p < 0.05, and the tests were 2-tailed.
RESULTS
Clinical characteristics of the study patients
The background data for patients are summarized in Table 1. The mean period between onset of RA and onset of reactive AA amyloidosis was 15.0 ± 7.1 years, and the mean period between onset of amyloidosis and the start of anti-TNF therapy was 3.9 ± 4.1 years. All patients received steroid treatment during the study period. The numbers of patients with accepted risk factors for chronic kidney disease, including use of nonsteroidal antiinflammatory drugs (NSAID), association of hypertension, dyslipidemia, and diabetes mellitus, was also recorded.
Clinical characteristics of patients enrolled in this study.
All 4 patients receiving infliximab treatment and 1 of 10 patients receiving etanercept treatment were given methotrexate together with anti-TNF therapy. The mean duration of anti-TNF therapy was 20.1 ± 13.8 months during the followup period.
Therapeutic effects of, and adverse events during, anti-TNF treatment
Table 2 shows the changes in clinical signs and laboratory variables in each subject following anti-TNF therapy. The mean numbers of tender joints and swollen joints and the mean DAS28(3)-CRP score were significantly lower after anti-TNF therapy. Levels of acute-phase reactant proteins such as CRP and SAA decreased dramatically after the start of anti-TNF therapy. No significant difference was observed in the mean level of renal function, as indicated by Cr, Ccr, and 24-h urinary protein excretion, before and after anti-TNF therapy.
Changes in clinical symptoms and laboratory findings following anti-TNF therapy. Data are expressed as mean SD.
Adverse events were observed in 2 patients during the followup period. Patient 1, who was treated with etanercept, developed a herpes zoster virus infection, and Patient 6, who was also treated with etanercept, developed acute bacterial cellulitis with rapid deterioration of renal function and started to receive hemodialysis therapy. These 2 patients continued to receive anti-TNF therapy after complete recovery from their respective infections.
Changes in renal function and proteinuria during anti-TNF treatment
The initial and last-visit laboratory findings for the study patients are summarized in Table 3, and the changes in 24-h Ccr and urinary protein excretion were recorded for 12 of the 14 patients. Twenty-four hour Ccr improved in 4 patients, remained unchanged in 5, and worsened in 3. In one patient hemodialysis therapy was started because of progression to renal failure during followup. Twenty-four hour urinary protein excretion was significantly decreased in 3 patients, not exacerbated in 6, and increased in 3 after the start of anti-TNF therapy. In our study, there was no significant trend between changes in kidney function and presence of established risk factors for chronic kidney disease.
Baseline characteristics and the initial and last visit laboratory data for all subjects.
Changes in areas of amyloid deposition in gastroduodenal mucosal tissue during anti-TNF treatment
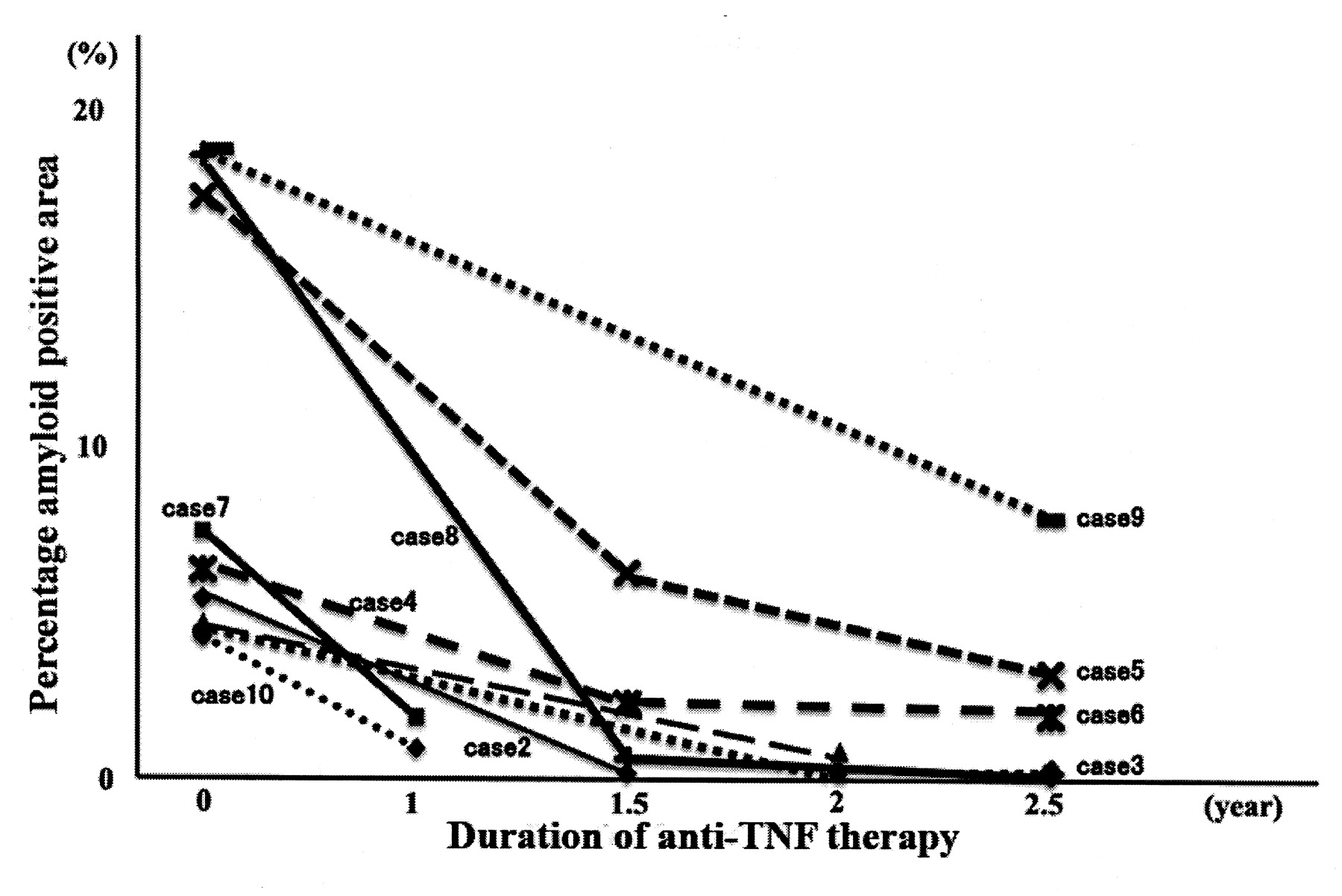
Figure 1 shows the changes in the percentage of amyloid-positive areas in gastroduodenal mucosal biopsy specimens after introduction of anti-TNF therapy in the 9 patients who received it. All of the patients achieved a significant decrease in the area of amyloid deposits in the second biopsy specimens, from 8.8% ± 6.4% before start of anti-TNF therapy to 1.6% ± 0.6% (p = 0.003) after. Four patients underwent a third biopsy and showed a sustained decrease in the area of amyloid deposits. In addition, amyloid deposits were not detectable in the third biopsy specimens from 2 patients (cases 3 and 8).

Changes in percentage amyloid-positive area in gastric biopsy specimens after introduction of anti-TNF therapy.
Figure 2 demonstrates one of the striking cases (case 3) showing disappearance of Congo-red-positive lesions in gastroduodenal mucosal specimens before and after anti-TNF therapy. These lesions completely disappeared 2 years after the start of treatment.

Gastrointestinal tissue before and after anti-TNF therapy in Patient 4. A. Before anti-TNF therapy: Congo-red–positive deposits were seen in gastric mucosal and submucosal lesions before the initiation of anti-TNF therapy. B. Two years after anti-TNF therapy: no Congo-red–stained lesions were observed in gastric specimens 2 years after the beginning of treatment. (Congo-red staining, original magnification ×200.)
DISCUSSION
Endstage renal disease and GI disease, including intractable diarrhea, are well known complications in RA patients with AA amyloidosis, and are considered major causes of death20–24,32–34. The survival rate of RA patients with AA amyloidosis on hemodialysis therapy is known to be extremely poor compared with the survival of patients with other kidney diseases32,35–37. Simultaneously, intractable diarrhea is reported to have a poor prognosis in such patients once it has developed23. Prevention or treatment of these complications is thus a critical issue.
There have been several attempts to establish an effective protocol for treatment of reactive AA amyloidosis associated with RA, including use of corticosteroids and immunosuppressants to control RA disease activity and to improve kidney function and overall patient survival. There have been several case reports indicating that remission of nephrotic syndrome can be achieved in RA-associated AA amyloidosis through the use of combination therapy with corticosteroid plus cyclophosphamide, azathioprine, or methotrexate15–18. However, such reports have been limited in number, and no significant influence of such conventional therapeutic strategies on overall survival has been described32,36.
Recently, many rheumatologists have focused on therapy with biologics, not only for control of RA disease activity but also as potential agents for the treatment of reactive AA amyloidosis in RA patients through strong suppression of acute-phase reactants such as SAA. A retrospective study and several case reports have already indicated that such agents are effective against AA amyloidosis25–30. Gottenberg, et al retrospectively studied the effects of anti-TNF agents in 15 patients with AA amyloidosis who had renal involvement secondary to inflammatory arthritis26. Three of the patients in that study showed rapid reduction of blood urea nitrogen levels and increased glomerular filtration rate; the disease stabilized in 5 other patients, and amyloidosis progressed in the remaining 7.
In our study, we explored 3 essential aspects of anti-TNF therapy for reactive AA amyloidosis in patients with RA. First, we proved that anti-TNF therapy achieved a significant improvement in the control of persistent RA disease. In such patients, the diagnosis of amyloidosis is often made when renal function has already deteriorated, and there is a need to avoid using immunosuppressants such as methotrexate and cyclophosphamide because of exacerbation of adverse effects. Recently, etanercept has been reported to be safe and effective in RA patients with kidney failure or receiving hemodialysis38; similarly, in our study, etanercept was effectively administered without any major adverse events in 8 patients whose Ccr were under 50 ml/min before the start of anti-TNF therapy. However, it is also well known that some RA patients do not respond to anti-TNF therapy39. It will be necessary to accumulate more data from patients with longer followup periods in order to clarify the overall effect of anti-TNF therapy for AA amyloidosis associated with RA.
Second, we showed that the percentage areas of amyloid deposition in gastroduodenal mucosal tissue were significantly decreased after initiation of the biologic treatment, indicating that amyloid deposits could be removed from gastroduodenal mucosal tissue by strict control of RA disease. Several indirect observations of renal function have suggested resolution of amyloid deposition in the kidneys18,19,25,27, but this has not been proved using repeat renal biopsies. Several reports have also suggested decreased amyloid deposition in the GI tract, but only on the basis of macroscopic observation28,30. Therefore our study is the first to have demonstrated a significant improvement in gastroduodenal amyloidosis on the basis of semiquantitative estimation of changes in amyloid deposition using microscopic observation, and our findings indicate a striking effect of anti-TNF therapy in removing amyloid deposits from tissues.
We used gastroduodenal mucosal biopsy to evaluate changes in the extent of amyloid deposits. A histopathological diagnosis of reactive AA amyloidosis can be established using tissue biopsy samples from the lip, kidney, rectal, or gastroduodenal mucosa, and from abdominal fat tissue9,13,40,41. We previously demonstrated that specimens obtained by gastroduodenal mucosal biopsy from RA patients had a higher rate of positivity for amyloid deposits than those from abdominal fat biopsy; the extent of gastroduodenal amyloid deposits was highly correlated with that of renal amyloidosis diagnosed by kidney biopsy, showing that gastroduodenal mucosal biopsy can reflect systemic organ involvement in amyloidosis13. Thus, serial gastroduodenal mucosal biopsy is a safe and appropriate way of evaluating systemic amyloid deposition in patients with RA.
Third, anti-TNF therapy may improve kidney function in some patients in terms of improved Ccr and/or reduced proteinuria, although 3 of our patients developed progressive renal disease and one began hemodialysis therapy during the followup period. Although we found a significant decrease in the percentage area of GI mucosal amyloid deposition in our patients, this change did not necessarily lead to an improvement of kidney function. It seems reasonable to suggest that the rapid therapeutic effect we observed in gastroduodenal lesions was due to the high turnover of gastroduodenal mucosal cells in comparison with kidney tissue. Longterm followup should be able to clarify whether this striking effect of biologic therapy for AA amyloidosis occurs only in gastroduodenal lesions.
The other potential benefit of the present therapy was improved control of SAA levels. Recently, it has been recommended that strict control of SAA to below 10 μg/ml is necessary to prevent the progression of AA amyloidosis6,33. However, although most of our patients showed a dramatic reduction in SAA levels after the start of anti-TNF therapy, only one patient had achieved the recommended level at the last visit.
Genetic background is thought to play a role in disease course and prognosis of reactive AA amyloidosis with RA. In Japanese RA patients, the SAA1.3 allele is known to be associated with increased susceptibility to reactive AA amyloidosis42, and our study of SAA1 gene polymorphism in Japanese RA patients supported this43. We have also reported a high prevalence of serum apolipoprotein E4 isoprotein in RA patients with reactive AA amyloidosis44. Although it is still unclear whether there are differences in therapeutic response between patients with AA amyloidosis secondary to RA who have or do not have such a genetic background, careful and intensive monitoring of these populations might be necessary, even when potent treatments such as anti-TNF therapy are used.
Recently, Okuda, et al reported an excellent effect of the anti-IL-6 receptor antibody tocilizumab in a case of reactive AA amyloidosis associated with juvenile inflammatory arthritis; the drug induced a marked and lasting suppression of SAA28. IL-6 is known to have a potent role in synergistic induction of the expression of the human SAA gene; it would therefore be a reasonable therapeutic option to use this newly developed approach to treat AA amyloidosis in RA patients whose SAA levels have not been fully suppressed by other agents.
In conclusion, our prospective study has demonstrated a striking effect of anti-TNF therapy for rapid resolution and sustained removal of gastric amyloid deposits, improved control of RA disease activity, and amelioration of kidney function in RA patients with reactive AA amyloidosis. We will continue our followup in order to obtain longer-term results, not only with regard to therapeutic efficacy and tolerability, but also the overall survival of the patients.
Footnotes
-
Supported by a grant from the Intractable Disease Division of the Ministry of Health and Welfare of Japan, and the Research Committee for Epochal Diagnosis and Treatment for Amyloidosis in Japan.
- Accepted for publication June 9, 2009.








{kind=link}
{kind=link}