

Abstract
Objective. Interleukin 18 (IL-18) has a central role in the pathogenesis of adult-onset Still’s disease (AOSD). We investigated the functional association of −607 (C/A) IL-18 promoter polymorphisms with disease course in Chinese patients with AOSD.
Methods. Sequence-specific primer polymerase chain reaction and the restriction fragment-length polymorphism method were used to analyze the genotypes of IL-18 promoter polymorphism at position −607 in 96 unrelated patients with AOSD and 164 ethnically-matched healthy controls. Serum IL-18 levels were determined using ELISA in patients with active untreated AOSD.
Results. Significantly lower frequencies of single-nucleotide polymorphism −607/AA were observed in patients with AOSD compared to healthy controls (18.8% vs 31.1%, respectively; p < 0.05). Median levels of serum IL-18 were significantly lower in AOSD patients with AA genotype compared to those with CA genotype or CC genotype (147.5 pg/ml vs 410.5 pg/ml or 262.4 pg/ml, respectively; both p < 0.05). Significantly lower IL-18 levels were demonstrated in AOSD patients with a monocyclic systemic course than in those with a polycyclic systemic course or a chronic articular course. The AA genotype was more frequently observed in patients with monocyclic systemic course, which had the best prognosis, than in those with the other 2 disease courses. In contrast, a lower frequency of the AA genotype than the CA or the CC genotype was observed in patients with chronic disabling arthritis (5.5% vs 25.0% or 19.2%, respectively).
Conclusion. The SNP −607/AA genotype with lower IL-18 levels might be a genetically protective factor for the occurrence of AOSD in the Chinese population, against progression of chronic disabling arthritis.
Adult-onset Still’s disease (AOSD) is an inflammatory disorder characterized by fever, evanescent rash, arthritis, and multisystemic involvement as well as laboratory abnormalities1–7. Although the etiology and pathogenesis remain unclear, cytokine-mediated inflammation may occur in active AOSD8–14. Recent studies, including ours, showed that serum interleukin 18 (IL-18) levels were markedly elevated and correlated significantly with serum ferritin values and disease severity in AOSD10–13. Moreover, our previous study showed elevated levels of IL-18 transcripts in biopsy specimens of Still’s rash and synovitis from patients with AOSD13. These results suggested that IL-18 has a central role in the pathogenesis of AOSD.
Several reports have shown that nucleotide polymorphisms occur within the regulatory region of cytokine genes, and some of these are associated with an altered rate of gene expression15–17. The human IL-18 gene is located on chromosome 11q22.2–q22.318, and promoters of this gene are located upstream of exon 1 and exon 219,20. There are several specific groups of single-nucleotide polymorphisms (SNP) within IL-18 gene, which characterize haplotypes as reported by Sugiura, et al21. Recent studies showed that the frequency of the haplotype S01 that is composed of 12 SNP in the 6.7 kb region upstream of IL-18 gene was significantly higher in Japanese patients with AOSD than in healthy controls21,22. Two functional SNP at position −607 and −137 in the promoter region of human IL-18 exon 1 have been identified23. A recent report showed that only the SNP at position −607 in the IL-18 promoter is associated with the development of AOSD in a Korean population24. The SNP at position −607 of the IL-18 promoter region has been predicted to be a nuclear factor-binding site for the cAMP-responsive element binding protein (CREBP), and the change from cytosine (C) to adenosine (A) nucleotide may affect promoter activity23. The sequence upstream from human IL-18 exon 1 has clear promoter activity, which can be enhanced by stimulation with PMA/ionomycin23.
Patients with AOSD may vary regarding clinical features and disease course3–7. In contrast to the distribution of patterns of disease course reported by Cush, et al4, Chinese patients with AOSD tend to be less susceptible to development of disabling arthritis6,7. To our knowledge, the association of promoter polymorphisms of IL-18 exon 1 with disease course in patients with AOSD has not previously been reported.
We investigated whether promoter polymorphisms at position −607 of IL-18 exon 1 predispose to susceptibility of Chinese patients with AOSD. The functional consequences of the SNP −607 of IL-18 promoter were assessed by measuring circulating IL-18 levels in patients with AOSD during the active phase of disease. The association of IL-18 promoter polymorphisms with clinical manifestations and disease course was examined after adjustment for potential confounders in patients with AOSD who were followed for at least 2 years.
MATERIALS AND METHODS
Patients
Ninety-six consecutive unrelated Chinese patients (71 women, 25 men; mean age at disease onset, 37.1 ± 15.0 yrs) fulfilling the Yamaguchi criteria for AOSD25 were enrolled. Patients with infections, malignancies, or other rheumatic diseases were excluded. The clinical activity score (range 0–12) for each patient with AOSD was assessed according to the criteria described by Pouchot, et al3. A prospective cohort design with collected outcome data was used in our study. Data were obtained on presenting manifestations and disease courses of all patients using standardized definitions and a standard extraction form. After diagnosis of AOSD and initial investigation of IL-18 levels, all patients were treated with non-steroidal antiinflammatory drugs or corticosteroids with or without disease-modifying antirheumatic drugs including hydroxychloroquine, sulfasalazine, methotrexate, and/or cyclosporine. According to the modified classification of the proposed disease course for AOSD4, 96 patients, followed for at least 2 years, were classified into 3 patterns defined as follows: monocyclic systemic — only 1 episode of systemic manifestation, followed by complete remission within 1 year after disease onset; polycyclic systemic — more than 1 episode of systemic manifestation, followed by partial or complete remission after onset of the initial or subsequent attack; and chronic articular — persistent arthritis involving at least 1 joint area, with radiographic evidence of bone erosion or ankylosis, lasting longer than 6 months13. One hundred sixty-four unrelated ethnically matched healthy volunteers (83 women and 81 men; mean age, 39.8 ± 12.4 yrs) living in Taiwan, without rheumatic disease, served as healthy controls. The Ethics Committee of Clinical Research, Taichung Veterans General Hospital, approved the study protocol and informed consent was obtained from each participant.
Determination of the −607* promoter polymorphisms of the IL-18 gene
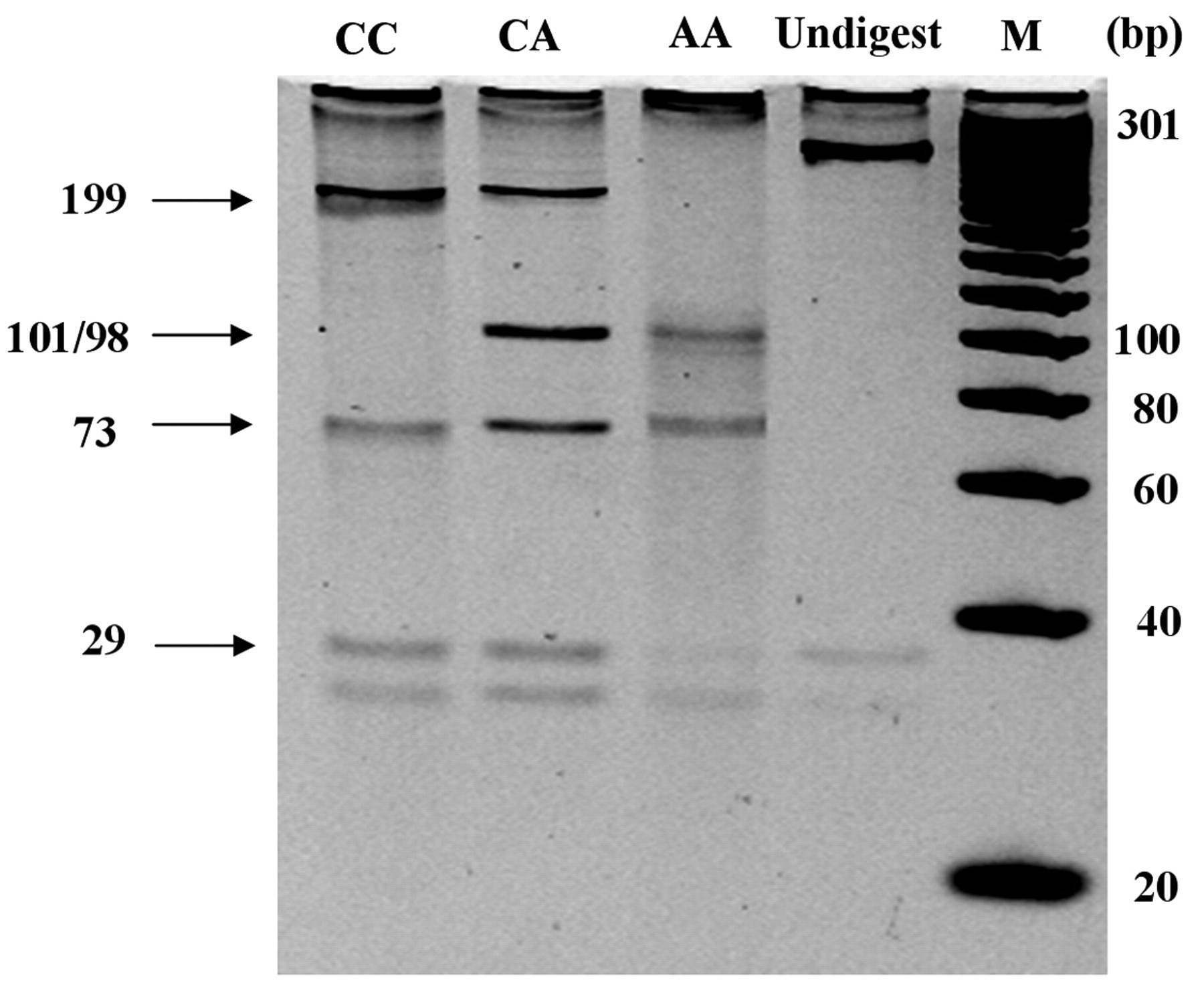
Genomic DNA was extracted and purified from whole blood of 96 patients with AOSD and 164 control subjects using the phenol-chloroform method26. The −607 genotypes of the IL-18 promoter were detected by restriction digestion of the polymerase chain reaction (PCR) product with Mse I27. PCR was performed using a set of primers described by Takada, et al27. The sense primer 5′-CTT TGC TAT CAT TCC AGG AA-3′ and antisense primer 5′-TAA CCT CAT TCA GGA CTT CC-3′ were designed to amplify a 301-bp DNA fragment covering the polymorphic site (GenBank accession number: rs1946518). Optimal PCR was performed in a thermocycler 9600 (Perkin-Elmer-Cetus, Norwalk, CT, USA) using a 30-cycle program (denaturation at 95°C for 5 min, followed by 95°C for 20 s, 60°C for 50 s, 72°C for 20 s, and a final extension at 72°C for 3 min). PCR products were digested with 5.0 U of Mse I (New England Biolabs, Beverly, MA, USA) at 37°C overnight, and run on a 4% ethidium bromide NuSieve GTG (BioWhittaker Molecular Applications, East Rutherford, NJ, USA) agarose gel (0.5 μg/ml gel). Mse I digested the 301-bp DNA segment from CC homozygous individuals into 199, 73, and 29-bp fragments; the DNA segment from AA homozygous individuals into 101/98, 73, and 29-bp fragments; and the DNA segment from CA heterozygous individuals into 199, 101/98, 73, and 29-bp fragments (Figure 1).

Mse I digested the 301-bp DNA segment from CC homozygous individuals into 199, 73, and 29-bp fragments; DNA segment from AA homozygous individuals into 101/98, 73, and 29-bp fragments; and DNA segment from CA heterozygous individuals into 199, 101/98, 73, and 29-bp fragments.
Determination of serum levels of IL-18
Serum levels of IL-18 were determined in 96 patients with active untreated AOSD using ELISA according to the manufacturer’s instructions (Bender MedSystems, Vienna, Austria). The overall intra- and interassay coefficients of variation were 2.9% and 12.5%, respectively.
Statistical analysis
Data were analyzed using SPSS 10.0 for Windows (SPSS, Chicago, IL, USA). The nonparametric Kruskal-Wallis test was used for between-group comparisons of serum IL-18 levels. Only when this test showed significant differences were the exact p values determined using the Mann-Whitney U-test. The correlation coefficient was obtained by the nonparametric Spearman’s rank correlation test. A multivariate logistic regression model was used to evaluate the simultaneous effects of genotypic variables on the occurrence of clinical manifestations in patients with AOSD. The differences in frequencies of alleles and genotypes of IL-18 promoter polymorphisms between patients with AOSD and healthy controls or among AOSD patients with different patterns of disease course were examined using the chi-squared method and Fisher’s exact test. p values less than 0.05 were considered significant.
RESULTS
Frequencies of −607* promoter polymorphisms of IL-18 gene
The frequencies of genotypes and alleles at position −607 of IL-18 promoter polymorphisms are summarized in Table 1. A significantly lower frequency of AA genotype was found in patients with AOSD compared to healthy controls (18.8% vs 31.1%, respectively; p < 0.05). We observed an increased frequency of CA genotype in patients with AOSD compared with controls (54.2% vs 42.1%), although this difference did not reach statistical significance (p = 0.079). Among patients with AOSD, the odds ratios of CA and CC genotypes for comparison with AA genotype were 2.14 [95% confidence interval (CI) 1.12–4.08, p = 0.030] and 1.67 (95% CI 0.82–3.45, p = 0.223), respectively. No gene dosage effect was found with the presence of the C allele. No significant differences in the distribution of allelic frequencies at position −607 were observed between patients with AOSD and controls.
Genotypic and allelic frequencies of interleukin 18 promoter polymorphisms at position −607 in patients with adult-onset Still’s disease (AOSD) and healthy controls.
Association of −607* promoter polymorphisms of IL-18 gene with clinical manifestations
All patients with AOSD had a high fever (> 39°C). Typical Still’s rash was present in 82 patients (85.4%) and arthritis was seen in 72 (75.0%). Hepatic dysfunction (alanine aminotransferase, ALT ≥ 40 IU/l) was present in 30 patients (31.2%), and lymphadenopathy was seen in 29 (30.2%). Multivariate logistic regression analysis showed no significant association between IL-18 promoter polymorphisms and clinical manifestations of patients with AOSD (data not shown).
Association of IL-18 promoter polymorphism with serum IL-18 levels in patients with AOSD during the active phase
Serum IL-18 levels correlated positively with clinical activity scores (r = 0.248, p < 0.05) in patients with AOSD (Figure 2A). Serum IL-18 levels were significantly lower in AOSD patients with SNP −607/AA genotype [median = 147.5 pg/ml, interquartile range (IQR) 90.9–330.7] than those with SNP −607/CA genotype (median = 410.5 pg/ml, IQR 160.0–696.9; p < 0.05) or those with SNP −607/CC genotype (median = 262.4 pg/ml, IQR 164.4−607.0; p < 0.05; Figure 2B). No significant difference in serum IL-18 levels between patients with CA genotype and those with CC genotype was observed.

A. Correlation between clinical activity score and serum IL-18 levels in patients with AOSD. B. Median levels of serum IL-18 in AOSD patients with different genotypes of IL-18 promoter at position −607. CC represents homozygotes for the C allele, CA heterozygotes for the C and A alleles, and AA homozygotes for the A allele. Boxes represent the range of levels from 25th to 75th percentile. Horizontal line within the box indicates median value; horizontal lines above and below represent maximum and minimum values for each group. *p < 0.05, vs group with AA genotype.
Association of IL-18 promoter polymorphisms and serum IL-18 levels with patterns of disease course
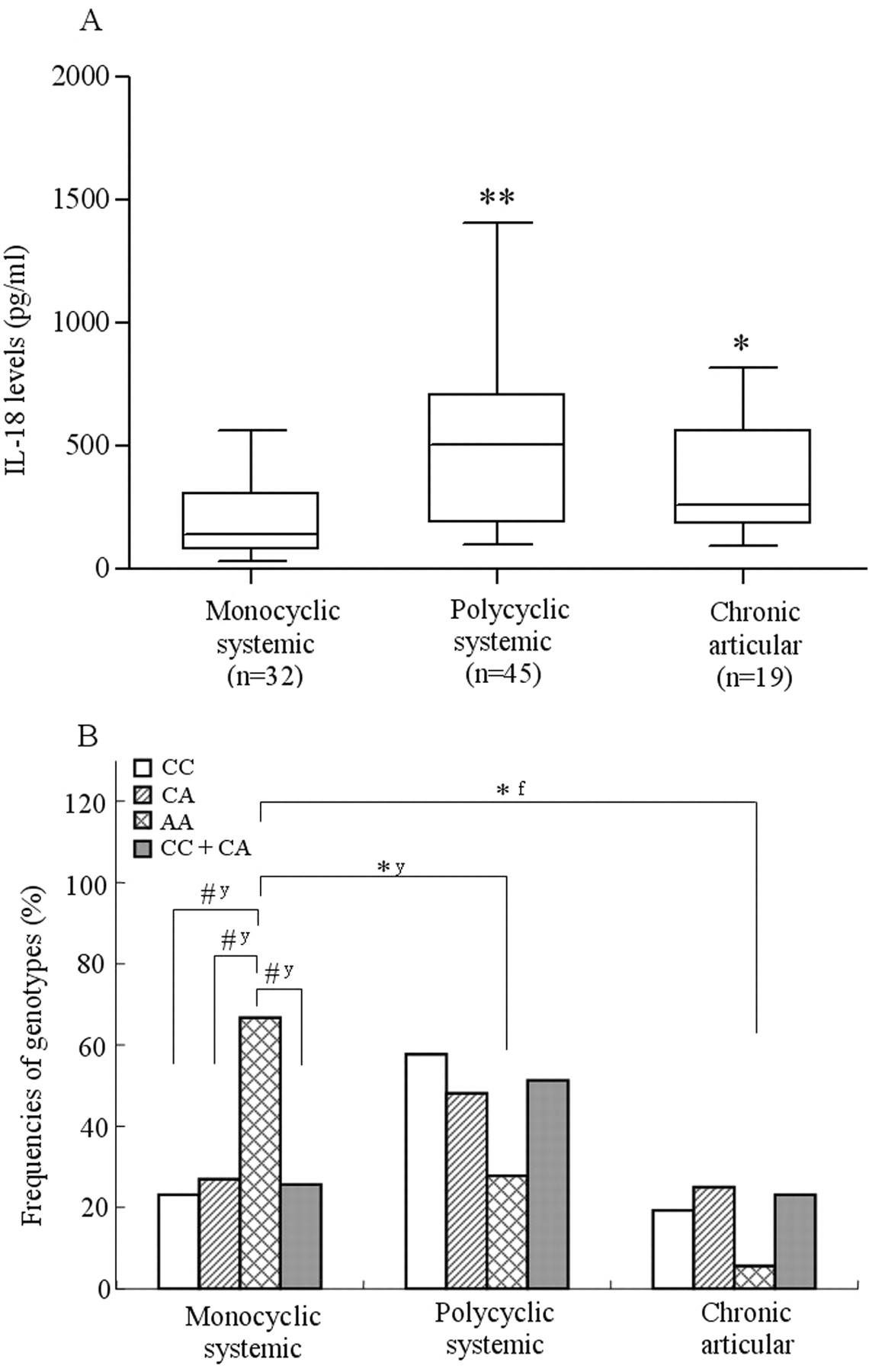
A followup analysis of 96 patients with AOSD was performed over a mean period of 70.9 ± 36.4 months (range 28 to 206 mo); 45 patients (46.9%) had a polycyclic systemic course, 32 (33.3%) a monocyclic systemic course, and the remaining 19 (19.8%) a chronic articular course. As shown in Figure 3A, significantly lower levels of serum IL-18 were demonstrated in AOSD patients with a monocyclic systemic course (median 140.1 pg/ml, IQR 80.0–309.6) than in those with a polycyclic systemic course (median 505.2 pg/ml, IQR 190.3–707.0; p < 0.01) or those with a chronic articular course (median 263.2 pg/ml, IQR 183.0–562.0; p < 0.05). As shown in Figure 3B, the AA genotype was more frequently observed in patients with monocyclic systemic course than in those with polycyclic systemic course and in those with chronic articular course (66.7% vs 27.8% or 5.5%, respectively; both p < 0.05). A significantly higher proportion of AOSD patients with a monocyclic systemic course had AA genotype (12/18, 66.7%) compared with CA genotype (14/52, 26.9%), CC genotype (6/26, 23.1%), and CA+CC genotype (20/78, 25.6%); all p values < 0.01 by chi-squared test with Yates’ correction of contingency. Although there was no statistical significance (p = 0.112, Fisher’s exact test), the frequency of patients with AA genotype (1/18, 5.5%) was lower than of CA genotype (13/52, 25.0%), CC genotype (5/26, 19.2%), and CA+CC genotype (18/78, 23.1%) in patients with chronic disabling arthritis. There was no significant difference in the frequency of chronic disabling arthritis between patients with CC genotype and CA genotype, or between those with CC genotype and AA genotype.

A. Median levels of serum IL-18 in AOSD patients with different disease courses. *p < 0.05, **p < 0.01, vs group with monocyclic course. B. Genotypic frequencies of IL-18 promoter in patients with different disease courses. *p < 0.05, vs polycyclic systemic or chronic articular course. #p < 0.01, AA genotype vs other genotypes among patients with monocyclic systemic course. y: Yates’ correction of contingency; f: Fisher’s exact test.
DISCUSSION
Our study, which includes the largest number of patients with AOSD from a single center, was to investigate functional association of promoter polymorphisms at position −607 of IL-18 exon 1 with clinical manifestations and various patterns of disease course in Chinese patients. We found that the frequencies of the SNP −607/AA genotype were significantly lower in patients with AOSD compared to healthy controls, suggesting that the SNP −607/AA genotype of the IL-18 promoter might be a genetically protective factor against occurrence of AOSD in the Chinese population. In contrast, significantly higher frequencies of the CA genotype relative to the AA genotype were observed in our patients with AOSD. Although the studied diseases were different, our data were similar to the findings of previous studies, which showed that the SNP −607/AA genotype might confer a protective effect against development of rheumatoid arthritis28 and lupus nephritis29 in Chinese populations. A recent study showed that the A allele at position −607 in the IL-18 promoter region may be associated with the susceptibility to AOSD in a Korean population24. The A allele at position −607, one component of haplotype S01 of IL-18 gene reported by Sugiura, et al21,22, was associated with the development of AOSD in a Japanese population. An explanation for this discrepancy between previous reports21,22,24 and our study might be the variation of genetic susceptibility between ethnic groups30. Nevertheless, our results and recent reports supposed that the regulatory regions of IL-18 gene are related to the development of AOSD.
Previous studies have shown that promoter polymorphisms of IL-18 exon 1 were associated with variable levels of IL-18 mRNA expression in Swedish patients with multiple sclerosis23, and that promoter activity at the upstream site of exon 1 could be upregulated by activation20. Our results demonstrated that serum IL-18 levels were significantly lower in AOSD patients with the AA genotype than in those with the CA genotype or CC genotype (Figure 2B). Our data were consistent with recent results that showed lupus patients with AA genotype had significantly lower IL-18 levels than those with the CC and CA genotypes29,31. Comparison of promoter polymorphisms of IL-18 gene with sequences in the TRANSFAC (Gene Transcription Factor) database suggest that the change from C to A at position −607 possibly disrupts a potential CREBP binding site and may reduce IL-18 production23. However, interindividual differences in the capacity to produce IL-18 may be affected by differences in transcription rate, translation efficiency, or protein processing: this gene dosage effect was not expected. It is possible that unidentified genetic polymorphisms exist in IL-18 gene and affect the expression of IL-18 protein.
The disease course and prognosis of patients with AOSD may vary considerably3–7. Although the prognosis of AOSD is generally considered to be relatively benign, patients with the chronic articular course exhibited greater disability and had a worse prognosis than those with the other 2 disease courses1–4. In our study, significantly lower frequencies of the SNP −607/AA genotype were observed in those with chronic articular course compared with those with the SNP −607/CA genotype (Figure 3B). Concerning their functional associations, we found that the AA genotype was more frequently observed in patients with monocyclic systemic course, which had lower levels of serum IL-18, than in those with the other 2 disease courses. Based on these data, we speculate that patients with AOSD carrying the SNP −607/AA genotype might have a lower risk of progression to chronic disabling arthritis. However, we cannot exclude the possibility that other genetic factors are important in determining the disease outcome of AOSD, and additional investigation will be needed to clarify the prognostic importance of polymorphisms in other cytokines.
The SNP −607/AA genotype, which is associated with lower IL-18 levels, is also associated with a favorable prognosis in Chinese patients with AOSD. Because AOSD has diverse disease phenotypes, complex roles of multiple cytokines32, and the possible polygenic etiology32–34, investigation of a single gene polymorphism is probably insufficient to explain the effects of a particular gene on the susceptibility of this disease. Further investigation of genetic polymorphisms of various pathogenesis-associated molecules in different ethnic groups is needed.
Footnotes
- Accepted for publication May 12, 2009.








{kind=link}
{kind=link}
{kind=link}